Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Cardiac contractility modulation wikipedia , lookup
Heart failure wikipedia , lookup
Hypertrophic cardiomyopathy wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Electrocardiography wikipedia , lookup
Antihypertensive drug wikipedia , lookup
Mitral insufficiency wikipedia , lookup
Coronary artery disease wikipedia , lookup
Artificial heart valve wikipedia , lookup
Lutembacher's syndrome wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Cardiac surgery wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
Heart arrhythmia wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
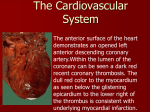
The Heart Dr. Rob Anderson Rowan University The Heart -Function • To pump blood around the body – Delivers nutrients and O2 to cells – Enables blood to radiate heat via convection/conduction – Homogenizes blood Heart Orientation • Located in the mediastinum – the median cavity of the thorax – from the 2nd rib to the 5th intercostal space Heart Anatomy - Pericardium • Pericardium – double-walled sac that covers the heart • 2 layers – Fibrous pericardium – protects the heart, anchors to surrounding tissues (e.g. diaphragm) – Serous pericardium • Parietal Layer – lines internal surface of the fibrous pericardium • Visceral layer (epicardium) – part of heart wall (covers myocardium) Pericardium Pericarditis • Inflammation of the pericardium (usually due to infection) • May prevent heart from beating efficiently in severe cases (cardiac tamponade) Heart Wall Anatomy • Epicardium – thin covering of tissue (visceral layer of pericardium) • Myocardium – the muscle tissue of the heart, interlace in a spiral pattern around heart – Interspersed with connective tissue (collagen) that acts as an insulator to e- charge, limiting action potential to specific pathways Endocardium • Layer of squamous endothelium that lines the inside surface of the heart • Very slick surface • Continuous with tunica media in blood vessels External Anatomy of the Heart • 4 Chambers – 2 Atria (superior aspect) – 2 Ventricles (inferior aspect) • Heart “Grooves” – Coronary sulcus – encircles the boundary between atria and ventricles – Interventricular Sulcus – Cradles the Anterior Interventricular artery and great cardiac vein Heart Internal Anatomy • Atria – Receiving chambers, separated by the inter-atrial septum • Ventricles – Sending chambers, separated by the interventricular septum Septum Blood Flow Through the Heart – Right Atrium • Receives blood from: – Superior Vena Cava – collects blood from body above the level of the diaphragm – Inferior Vena Cava – collects blood from body below the level of the diaphragm – Coronary Sinus – collects blood from cardiac circulation Right Ventricle • Receives blood from right atrium and pumps it to lungs via the pulmonary artery (left and right branches) Left Atrium • Receives oxygenated blood from the lungs via the pulmonary veins, sends to left ventricle Left Ventricle • Receives blood from right atrium, pumps blood out to body cells via the aorta • Most heavily muscled of the heart chambers – Why? Coronary Circulation • Coronary Arteries – Arise from base of aorta and encircle the heart in the coronary sulcus • Critical in supplying myocardium with O2, food and in removing wastes Left Coronary Artery • Left Coronary Artery – Branches into – Anterior interventricular artery • Supplies interventricular septum and ventricles – Circumflex Artery • Supplies left atrium and posterior wall of left ventricle Right Coronary Artery • Supplies right side of heart and branches into – Right marginal artery – serves lateral right side of heart – Posterior interventricular Artery – serves posterior ventricle walls Cardiac Veins • Collects blood from myocardium and merge to form the cardiac sinus (empties into right atrium) • Great – anterior interventricular sulcus • Middle – Posterior interventricular sulcus • Small – Right inferior margin Myocardial Infarction (MI) a.k.a. Heart Attack • The myocardium needs a tremendous amount of resources (glucose, O2, etc.) to keep beating • Coronary circulation can get blocked by damage or fatty deposits (plaque) • If flow of blood is prevented long enough, the heart muscle itself can die, reducing or eliminating the heart’s ability to pump blood Heart Valves • 4 Valves in the heart prevent backflow of blood – Atrioventricular valves – located between atria and ventricles – Semilunar valves – located between ventricles and arteries • Valves are NOT under muscular control, they only close due to the differences in pressure created during the cardiac cycle Atrioventricular Valves • Right AV valve – composed of three flaps of endocardium (tricuspid valve) • Left AV valve – composed of two flaps of endocardium (mitral valve or bicuspid valve) Semilunar Valves • Aortic Valve – prevents blood flow back into left ventricle after contraction • Pulmonary Valve prevents blood flow back into right ventricle after contraction Valve Connections • The flaps of tissue (endocardium) that make up the AV valves are connected to the muscular walls of the heart – Chordae tendineae – chords of connective tissue (collagen) that attach to the “ventricle-side” of the AV valves – Papillary muscles – Connect chords to the ventricle wall and maintain chord tension Valve Reinforcement • The ventricles produce a tremendous amount of blood pressure • What prevents the valves from “blowing out”? Heart Murmurs • Valves do not close properly or open fully • Incompetent Valves – valve does not close properly, leading to blood backflow (prolapse) • Stenosis – valve narrowing – makes the heart work harder to push blood through a smaller opening The Heart “Pacemaker” • In order to effectively pump blood, the heart needs to contract with a rhythm – alternating contractions between atria and ventricles • How is this accomplished? Autorythmic Cells (Centers) • Initiate their own contraction of the heart muscle http://www.youtube.com/watch?v=U4A_1Igh_2w • Is that it? Autorhythmic Centers Autorhythmic Cells in the Heart • Sinoatrial Node – (Right atrial wall) • Atrioventricular Node (just above tricuspid valve) • Atrioventricular Bundle (Bundle of His) (superior part of ventricular septum) • Right and left bundle branches (in ventricular septum) • Purkinje Fibers (from ventricular septum to heart apex and around to ventricular walls) Rhythms • Pacemakers (nodes) follow a hierarchy in setting the rhythm of heart depolarization • Each node (bundle of autorhythmic cells) has its own rhythm – E.g. - Sinoatrial node drives heart rate at ~75 bpm Arrhythmias – Irregular Heartbeat • Pacemakers follow a hierarchy in setting the rhythm of depolarization • Each node (bundle of autorhythmic cells) has its own rhythm • Occasionally, this hierarchy can be upset, SA node may be damaged or malfunctioning – AV node – only 50 bpm (junctional rhythm) – AV bundle and Purkinje fibers (30 bpm) Fibrillation – out of phase contractions • “Squirming bag of worms” • Out of phase contractions means that there is no coordinated movement and thus no efficient blood flow • Can be “reset” by shocking the heart (defibrillator) to depolarize the entire heart, causing the SA node to restore rhythm http://www.youtube.com/watch?v=UAs6SDI7HZw Heart Block • Damage to the AV node prevents SA impulses from reaching ventricles • The ventricles then beat at their intrinsic rhythm (~30 bpm) • Pacemakers are inserted to reestablish the connection and restore functional rhythm Extrinsic Innervation of the Heart • Autonomic Nervous system modifies the heartbeat set by the autorhythmic cells • Cardioacceleratory Center – regulated by sympathetic division of the autonomic nervous system • Cardioinhibitory Center – regulated by parasympathetic division of the autonomic nervous system Monitoring the Heart (pg 680) • Electrocardiograph (EKG) – can monitor and record action potentials of the heart as it beats – P wave – depolarization of the pacemaker cells (the SA node) – QRS complex – Recording of ventricular depolarization – T wave – Ventricular repolarization – P-Q interval – time between atrial and ventricular excitation – S-T segment – beginning of ventricular depolarization to the end of repolarization The QRS Wave Heart Sounds • Lub-dub! • First sound in the cycle is when the atrioventricular valves (AVs) close – Ventricular pressure higher than atrial pressure • Second sound occurs as the semilunar valves (SLs) close – Aortic SL valve slightly before the pulmonary SL valve Heart Murmurs • May be normal in older and younger people • Can also signify a “leaky valve” – Failure to fully close = incompetent • Swishing sound is heard – Failure to completely open = stenotic • High pitched or gurgling sound is heard Cardiac Cycle • Systole – contraction period – Atrial and ventricular • Diastole – relaxation period – Atrial and ventricular • Important to understand! Mechanical Events of the Heart: Ventricular Filling (Step 1) • Blood flows passively through the atria into the ventricles via the open AV valves • Aortic and pulmonary valves are closed • Atria contract, pushing blood into ventricles • Ventricles are at end of diastole, and fully relaxed to receive blood from atria Heart Diastole (1st part of cardiac cycle) Mechanical Events of the Heart: Ventricular Systole (Step 2) • Atria relax and ventricles begin to contract • AV valves snap shut • Ventricular pressure rises, overcoming the pressure in the arteries and blood flows out of the heart (SL valves are forced open) • Atria are relaxed and filling with blood to start the next cycle Heart Systole (2nd part of cardiac cycle) Mechanical Events of the Heart: Isovolumetric Relaxation (Step 3) • Ventricles relax and ventricular pressure drops • Remaining pressure in the aorta and pulmonary artery closes the SL valves • As pressure from blood in atria increases, AV valves open, refilling the ventricles with blood Cardiac Output • Cardiac Output - The amount of blood moved by the heart in one minute in each ventricle • Stroke Volume (SV)– Amount of blood pumped out by one ventricle during each contraction (~70 ml) • Cardiac Output (CO) = Heart Rate (HR) x Stroke Volume (SV) • Let’s do an experiment! Stroke Volume Regulation • Stroke volume is the difference in the volume left in a ventricle at diastole (end diastolic volume or EDV) minus the blood left in a ventricle at the end of systole (end systolic volume or ESV) • SV = EDV – ESV • Can be affected by preload, contractility and afterload Stroke Volume Factors • Preload – the degree to which cardiac muscle cells are stretched just before they contract – Determined by • Maximum # of active cross-bridge attachments between actin and myosin • The force of contraction is maximal • In the heart this is determined by venous return – the amount of blood extending the ventricles prior to contraction. Stroke Volume Factors • Because cardiac muscle is normally shorter than optimal length, stretching cells can produce a huge increase in contractive force • Increases in ventricular volume = increase in stroke volume • Increase in ventricular volume caused by – Exercise – Resting • Decrease caused by – Hemorrhage – Tachycardia Stroke Volume Factors • Contractility - the contractile strength of a muscle at a certain length – Contractility is increased by greater Ca2+ influx into the cytoplasm from extracellular fluid and sarcoplasmic reticulum (SR) • Increased contractility results in a lower end systolic volume (ESV) – Contractility can be increased by • Sympathetic stimulation • Norepinephrine release (hormones!) Stroke Volume Factors • Afterload - The arterial pressure that must be overcome for the ventricles to eject blood • Pressure required by the heart ventricles to “open the door” of the aortic and pulmonary (semilunar) valves due to blood pressure – Pressure in aorta is about 10x the pressure in the pulmonary artery • Usually only a problem in people with hypertension (reduction in stroke volume) Heart Rate Regulation • Heart rate (and thus cardiac output) is relatively constant in healthy individuals, but can be affected by: • Factors that increase HR and CO are positive chronotropic factors, while those that decrease are negative chronotropic factors Autonomic Control of Heart Rate • Positive Chronotropic factors are under sympathetic control – Norepinephrine is released – Norepinephrine binds to cardiac cell membrane receptors (see pathway on pg. 685) – Ca2+ enters (and is removed) more rapidly into cytoplasm to facilitate increased in heart rate Autonomic Control of Heart Rate • Negative Chronotropic Factors are under parasympathetic control – K+ channels are opened via acetylcholine (neurotransmitter) release, which hyperpolarizes sarcolemma Simultaneous Autonomic Influence • The heart is constantly under BOTH sympathetic and parasympathetic influence, however, the parasympathetic influence (via the vagal nerve) is dominant under normal conditions • If the vagal nerve is cut, HR immediately increases 25bpm (to ~ 100 bpm) • However, stimulation of one arm of the autonomic nervous system depresses the other – E.g. Bainbridge reflex (increased atrial volume = increased heart rate) Chemical Regulation of HR • Hormones – Epinephrine – Thyroxine – Hormones that regulate K+, Ca+ or Na+ Other factors that affect HR • Age – Prenatal heartrate ~ 140-170 bpm • Exercise • Fever Fast and Slow HR • Tachycardia – abnormally fast HR • Caused by – Drugs – Heat stress – Emotional Stress • Bradycardia – Lower HR – Physically fit people have hypertrophy of the ventricles – May lead to clotting and edema in sedentary people CO Problems • Important to maintain balance between arterial flow and venous return • Congestive heart failure (CHF) – blood pumping is not sufficient to meet the demands of the body Reasons for Heart Failure • Coronary Atherosclerosis – Fatty buildup (plaque) in coronary arteries that limits flow of blood to the myocardium • Chronic High blood Pressure – Leads to gradual weakening of the left ventricle • Damage from Heart Attacks (Myocardial Infarction) • Dilated Cardiomyopathy – Heart becomes overstretched – CO is impaired Heart Attack (Myocardial Infarction) Right vs. Left Ventricle Failure • The heart has to maintain an even flow between right and left ventricles • Right ventricle failure = pulmonary congestion – Lungs become over engorged with blood resulting in pulmonary edema • Left ventricle failure = peripheral congestion – Blood stagnates in body organs resulting in blood pooling and swelling Heart Developmental Defects • Ventricular Septal Defect - “hole in the heart” – During development, the hole in the interventricular septum does not close, resulting in mixing of high and low O2 blood • Coarctation “constriction” of the aorta – narrowing causes heart to work harder • Tetrology of Fallot – – Multiple defects