Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Cancer immunotherapy wikipedia , lookup
Immune system wikipedia , lookup
Innate immune system wikipedia , lookup
Adaptive immune system wikipedia , lookup
Surround optical-fiber immunoassay wikipedia , lookup
Globalization and disease wikipedia , lookup
Thiomersal controversy wikipedia , lookup
Whooping cough wikipedia , lookup
Hygiene hypothesis wikipedia , lookup
Herd immunity wikipedia , lookup
Eradication of infectious diseases wikipedia , lookup
Psychoneuroimmunology wikipedia , lookup
Vaccination policy wikipedia , lookup
DNA vaccination wikipedia , lookup
Non-specific effect of vaccines wikipedia , lookup
Immunocontraception wikipedia , lookup
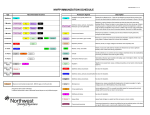
Childhood immunizations in the United States wikipedia , lookup
Global Advisory Committee on Vaccine Safety 6 - 7 June 2006 Potential immunogenic overload resulting from concomitant vaccination with too many antigens David Goldblatt Professor of Vaccinology and Immunology/ Consultant Paediatric Immunologist Director of Clinical R&D Institute of Child Health, UCL And Great Ormond Street Children’s Hospital Director, WHO Pneumococcal Serology Reference Laboratory Is there a scientific question to answer? • What is “injection overload” or “immune overload”? • How is it identified? • What would the symptoms of overload be? – reduced responses to multiple vaccines given at the same time? – increased risk of other infections after vaccination? 1946 1946 Pneumococcal PneumococcalHexavalent Hexavalent 1955 1955 Tetanus Tetanusand andDiphtheria DiphtheriaToxoids Toxoids(Td) (Td) 1975 1975 Meningococcus MeningococcusAACC 1977 1977 Pneumococcal Pneumococcal14 14Valent Valent 1981 1981 Meningococcus MeningococcusAACCYYW135 W135 1983 1983 Pneumococcal Pneumococcal23 23Valent Valent 1960 1960 Smallpox Smallpoxand andYellow YellowFever Fever 1967 1967 Smallpox Smallpoxand andMeasles Measles(Swz) (Swz) 1977 1977 OPV OPVand andMMR MMR 1983 1983 Hib Hiband andMMR MMR 1989 1989YF YFand andMeasles Measles(Swz) (Swz) 1 Live Viral Vaccines Multi-component Combination Vaccines FcγR Simultaneous Administration Of Childhood Vaccines È È IL12 IL12production production Ç Ç IL10 IL10production production Ç Lymphocyte Ç Lymphocyteapoptosis apoptosis APC CD46 È ÈAntigen Antigenspecific specific TTcell cellproliferation proliferation È ÈHypersensitivity Hypersensitivity responses responses T MV Proteins J Infect Dis 1996 Does MMR “overwhelm” the immune system? % seroconversion Measles Mumps Rubella Single Measles 100 -- Single Mumps -- 92 --- Single Rubella -- -- 100 MMR Vaccine 96 90 100 Pediatrics 1981 2 Response of 12-23 month old children receiving MMR and VZV vaccines alone or in combination 1000 100 MMRV + Placebo Hep A/B + DTaP-IPV/Hib Hep A/B + MMR MMR + VV 10 1 Measles Mumps Rubella VZV Vaccine 2005 Shinefield et al 2005 Live Viral Vaccines Multi-component Combination Vaccines Simultaneous Administration Of Childhood Vaccines Co-administration of DTaP and Hib conjugate vaccine at 4 and 6 m of age following DTaP at 2 m. Anti-Hib Polysaccharide Ab 4 What is the mechanism? 3.5 3 A DTP-a, Hib, IPV 2.5 B DTP-a + IPV, Hib 2 C DTP-a + Hib, IPV 1.5 D DTP-a + Hib + IPV 1 0.5 0 4 months 6 months 7 months Eskola et. al. 1996 Lancet;348:1688-92 Is this immune overload? 3 Claesson et al J Pediatr 1988 DTaP 10.1 aP Tetanus Al(OH)3 11 Dip aP No PncT PncT 12.5 + 9 µg TT + 24 µg TT + 72 µg TT 2 Anti PRP (µg/ml) -T PRP Pn cT ( 4va len t) 4.1 2, 4, 6 months Dagan et al, Infect & Immun 66:266:2-9393-8, 1998 12 11 11.5 10 7.8 8 6 PncD PncD1 (low dose) PncD PncD3 (medium dose) PncD PncD10 (high dose) -T P RP 7.2 4 No PncD PncD P = NS PncT PncT1 (low dose) PncT PncT3 (medium dose) PncT PncT10 (high dose) / Pw DT Geometric mean concentration after dose 3 aP Tetanus 6 0 Tet aP w/ 8 Hib DTP 10 Hib Dip aP P = 0.0121 12 + Tetanus ( 4va l en t) Tet aP Al(OH)3 aP aP Pn cD aP Al(OH)3 Dip Geometric mean concentration after dose 3 Tet Hib Hib 2, 4, 6 months 4 2 0 Anti PRP (µg/ml) Dagan et al, Infect & Immun 66:266:2-9393-8, 1998 4 *iC3b * CR2 Protein B B7-1/-2 CD28 II IL4 CD40 CD40L CD4 IL2 Journal of Infectious Diseases 2005 Protein *iC3b * CR2 B Polysaccharide Specific Antibody g chin swit n ype atio Isot tur ma y t i in Aff B CD40 CD40L Cytokines Cytokines II II CD4 Cytokines Cytokines II B II B Protein CD4 CD4 CD4 Memory B Cells BSI-99b 5 Protein B II B Cytokines CD4 II Cytokines CD4 Tetanus conjugates DTwP/IPV/PRPT 1 DTwP/IPV/PRPT * 2 7 10 13 4 2 7 * 0.1 2 12 100 13 7 12 5 * * 0.1 2 7 12 * * 0.1 * 1 * 0.1 2 10 7F 1 13 7 12 Age (months) 13 7 12 13 23F 1 * * 0.1 2 13 19F 10 1 10 * * * 0.1 10 9V 2 7 2 10 7 12 13 6B 1 0.1 2 10 7 12 14 13 * 1 0.1 2 10 7 12 13 18C * 1 12 13 DTwP/IPV/PRPT * 2 12 2 7 12 Age (months) 10 13 4 * 0.1 2 7 12 100 13 7 12 5 * * 0.1 2 7 12 13 * 1 * * 1 * 0.1 2 10 7F 7 12 Age (months) 13 7 12 13 23F 1 * * 0.1 2 13 19F 10 1 13 * * * 0.1 10 9V 1 2 3 1 DTaP/IPV/PRP-T 0.1 7 1 10 10 * 0.1 0.1 Age (months) 1 0.1 10 Diphtheria conjugates Concomitant Administration: DTwP/IPV/PRPT 1 0.1 12 1 1 3 1 DTaP/IPV/PRP-T * 0.1 Tetanus conjugates 10 Anti-capsular IgG concentrations (µg/ml) Anti-capsular IgG concentrations (µg/ml) 1 10 10 Anti-capsular IgG concentrations (µg/ml) 10 Serotye specific Pneumococcal IgG following an 11-valent experimental Pneumo-Conjugate Vaccine Diphtheria conjugates Concomitant Administration: 2 7 Anti-capsular IgG concentrations (µg/ml) Serotye specific Pneumococcal IgG following an 11-valent experimental Pneumo-Conjugate Vaccine 2 10 7 12 13 7 12 13 6B 1 0.1 2 10 14 * 1 0.1 2 10 7 12 13 18C * 1 0.1 12 Age (months) 13 2 7 12 Age (months) 13 Dagan, Goldblatt, Maleckar et al Inf & Imm, In Press Effect on Hib, tetanus and diphtheria responses to DTaP/Hib-TT from co-administration of different MCC vaccines 7 6 GMC (ug/ml) Providing extra carrier mediated help (at a separate site) can help overcome the attenuation seen with DTaP/Hib-TT combinations 5 4 MCC-CRM + PNC-CRM * 3 MCC-CRM * 2 MCC-TT ** 1 0 Hib tetanus diphtheria *Southern et al 2006 **Goldblatt et al 2006 6 • Responses to Measles, Mumps and Rubella are similar irrespective if given singly or in combination • MMR does not interfere with responses to concomitant vaccines • MMR does not lead to susceptibility to infections in the 90 days post infection • Combined vaccines may display reduced responses due to individual components • These are due to physical degrading of vaccine components or skewing of the immune response to those components present in high dosage We conclude that although there is no scientific evidence that supports parents’ fears about combined vaccines causing “immune overload”, policy makers need to recognise these concerns if they are to successfully persuade parents that combined vaccines are safe. 7