Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Management of acute coronary syndrome wikipedia , lookup
History of invasive and interventional cardiology wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Coronary artery disease wikipedia , lookup
Heart failure wikipedia , lookup
Rheumatic fever wikipedia , lookup
Electrocardiography wikipedia , lookup
Myocardial infarction wikipedia , lookup
Mitral insufficiency wikipedia , lookup
Hypertrophic cardiomyopathy wikipedia , lookup
Cardiac surgery wikipedia , lookup
Lutembacher's syndrome wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Atrial septal defect wikipedia , lookup
Ventricular fibrillation wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
Heart arrhythmia wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
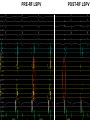
RADIOFREQUENCY ABLATION OF FIBRILLATION: What clinicians should know. DR CARLOS LABADET Electrophysiology Sector Dr. Cosme Argerich Hospital WHAT ARRHYTHMIAS ARE CURED? • • • • • Wolff-Parkinson-White syndrome Supraventricular paroxysmal tachycardia Atrial flutter Atrioventricular node Atrial tachycardias SUCCESS 90 - 100 % ADVANCEMENTS IN ABLATION • • • • ATRIAL FIBRILLATION VENTRICULAR TACHYCARDIAS VENTRICULAR EXTRASYSTOLE ATYPICAL ATRIAL FLUTTERS Sucess…~ 70% ATRIAL FIBRILLATION Problems • • • • Increase in mortality! Embolism and stroke Hospitalization CHF: lack of atrial systole Cardiomyopathy by tachycardia • Left atrial (LA) dilatation by AF • Chronic anticoagulation • Chronic symptoms of AF (palpitations, fatigue, etc.) HOW TO AVOID THIS WITH AN “ANTIARRHYTHMIC” DRUG?? Degenerative Age Increase of LA diseases LV systolic dysfunction Tachycardia begets more tachycardia Obesity ATRIAL FIBRILLATION Atrial fibrosis LV diastolic dysfunction HTN Inflammation Toxic Metabolic syndrome Genetic Diabetes Sleep apnea Pericardial fat Endocrinological disorders Respiratory disorders Spanish Registry of Ablation 2007 Rev Esp Cardiol 2008;61:1287 Male, 26 years old, he consults due to palpitations Male, 40 years old, no heart disease, palpitations 5h ORAL PROPAFENONE 450 mg AF: WHAT IS THE MECHANISM • AF is started by focused triggers, 95% in the pulmonary veins (PV) • AF is perpetuated by multiple microreentries or “rotors” • Dominant rotors locate in the PV-LA junction • Vagal impulse can trigger and maintain AF. There are vagal ganglionic areas in the PV-LA junction. MECHANISM OF AF AND OBJECTIVES OF ABLATION Anatomia e Histologia de venas pulmonares Anatomy and histology of pulmonary veins LSVP Myocardial bands LA FOCUSED TRIGGERS IN PULMONARY VEINS Haissaguerre et al. Circulation 1997;95:1120 TECHNIQUE OF ELECTRIC DISCONNECTION OF PULMONARY VEINS LSPV LIPV CIRCUNFERENTIAL ISOLATION RSPV LSPV RIPV LIPV ANTRUM PRE-RF LSPV VP S POST-RF LSPV PRE ABLATION POST ABLATION 120 mseg DESCONEXION ELECTRICA VP-AI A V A V A V A V REGISTRO DE VENAS PULMONARES FA Ablación unión VP-AI A A A A PULMONARY VEIN ABLATION – Potential mechanisms • • • • PV and foci isolation Removal of focused triggers Modification of substrate Autonomic denervation (vagal plexi) AF ABLATION IN REFERENCE CENTERS RESULTS ABLATION OF AF RECURRENCE Pappone et al J Am Coll Cardiol 2003;42:185–97) 70% success 50% 2nd RFA 2-3% complic. NEJM 2004;351:2373 (AFFIRM type) >65 y.o.+ HTN-Diab-CHF-ACV-LVEF<40% EF>40 SR EF<40 SR EF>40 AF EF<40 AF STROKE /YEAR: SINUS RHYTHM AF Nademanee JACC 08,50:843 0.4% 2% European Guidelines of Cardiology 2010 AF ABLATION IN THE REAL WORLD COMPLICATIONS Circulation 2005;111:1100 • 162 centers with 45,115 procedures in 32,569 pts.(1995-2006) Mortality at 30 days = 0.98/1,000 pts. SPANISH REGISTRY OF ABLATION 2007 1,624 accessory pathways: mortality = 1/1000 2,065 nodal reentry: mortality = 0.5/1000 JACC 2009;53:1798 Spanish Registry of Ablation 2007 Complications Rev Esp Cardiol 2008;61:1287 CURRENT INDICATIONS OF AF ABLATION Post-AF ablation – immediate control • Remain with anticoagulation for 1-3 months • During first 72 hs pericarditis may appear (fever, precordial pain, effusion, evaluate by echo) • PAF commonly appears as an effect of rF • Discharge at 24-48 h • Maintain antiarrhythmic agents during the first 1 to 3 months Post-AF ablation Long term • Patients may present left AF or AFl during the first 3 months, not associated to subsequent recurrene. • The most severe complication: atrioesophageal fistula (0.01%). It appears between the first and second week: fever, bacteriemia, leukocytosis, epigastric pain, neurological focus=hospitalization=NMR or CT=NONendoscopic surgery or contrast study. Post-AF ablation Long term • PV stenosis: around 1%: between the 2nd and 5th months: dyspnea, cough, hemoptysis, chest pain • Severe stenosis of a vein or multiple veins • Angioplasty with stent 3-D navigation system of AF ablation LA USEFULNESS OF 3-D NAVIGATORS VPSI VPSD LAA VPII Catéter circular Catéter de ablación AF ablation: Who are the main candidates? • PAROXYSMAL or PERSISTENT AF <1 year, symptomatic, recurrent with drugs. • Age <65 years old • Minimal or no heart disease • Left atrium <50 mm CONCLUSIONS • The patients with paroxysmal forms of AF and with minimal heart disease obtain the greatest results with radiofrequency ablation. • Those wiht persistent forms greater than 1 year or permanent, require more prolonged procedures and frequently require a second ablation. CONCLUSIONS • Although the information comes from observational studies, those with AF + left ventricular dysfunction present an improvement in ejection fraction • Currently, studies on heart failure and ventricular impairment are being developed to assess this phenomenon. Thank you for your attention!!