Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Management of acute coronary syndrome wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Hypertrophic cardiomyopathy wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Ventricular fibrillation wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
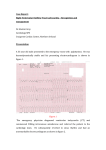
PARASYMPATHOMIMETIC STIMULATION PROVOKES VAGALLY MEDIATED PREMATURE VENTRICULAR CONTRACTIONS DURING ELECTROPHYSIOLOGIC STUDY AND ABLATION Kassenberg W, vd Heijden J, Hassink R, Doevendans P, Loh P. Department of Cardiology, Heart Lung Center Utrecht, University Medical Center, Heidelberglaan 100, P.O. Box 85500, 3508 GA Utrecht, The Netherlands. Background During electrophysiologic study (EPS) and radiofrequency (RF) ablation of mainly vagally mediated, symptomatic premature ventricular contractions (PVC), ectopy may be absent due to stress induced sympathetic stimulation or sedative drugs. We hypothesized that pharmacological stimulation of the parasympathetic nervous system may provoke PVC’s. Methods and results We included three female patients with symptomatic PVC’s with left bundle branch block morphology and vertical axis (right ventricular outflow tract (RVOT) origin). Previous ablation attempts failed because PVC’s were absent and could not be provoked by sympathetic stimulation (isoprenaline), atropine, adenosine, esmolol or sedation. Antiarrhythmic drugs were withheld 5 half-lives before the procedure. Procedures were conducted under general anaesthesia or Propofol sedation. A parasympathomimetic drug (Neostigmine, 1 mg) was administered intravenously (iv). After 7-15 minutes clinical PVC’s appeared (figure 1) and enabled activation mapping and successful ablation in all 3 patients. Earliest activation during mapping was found postero-lateral, septal and anterior in the RVOT. Early signals were found up to 40ms before QRS. Post ablation provocation with Neostigmine was done in two patients. No PVC’s were induced. One patient received the maximum dose pre ablation. Follow up of 4 and 21 months respectively showed no recurrence of ectopic contractions on Holter monitoring in 2 patients. One patient had recurrence of ventricular ectopy with other morphologies. All three procedures were free of complications. Conclusion In electrophysiological study and ablation procedures where mainly vagally mediated PVC’s are non-inducible due to sympathetic stimulation (stress) and/or sedative drugs, stimulation of the parasympathetic nervous system with Neostigmine provokes ventricular ectopy and enables activation mapping and ablation.