Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Jatene procedure wikipedia , lookup
Remote ischemic conditioning wikipedia , lookup
Antihypertensive drug wikipedia , lookup
Heart failure wikipedia , lookup
Hypertrophic cardiomyopathy wikipedia , lookup
Electrocardiography wikipedia , lookup
Coronary artery disease wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Cardiac surgery wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
Heart arrhythmia wikipedia , lookup
Ventricular fibrillation wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
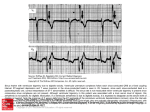
51A JACC Vol. 5, No.5 May 1985:5 1A- 59A Effects of Digitalis on the Normal and the Failing Heart EUGENE BRAUNWALD, MD, FACC Boston , Massachusetts Although it has been known for more than a century that digitalis glycosidesexert a powerful beneficialeffect on patients with heart failure, atrial fibrillation and a rapid ventricular rate, it was believed for many years that the drug exerts this clinical effect primarily by slowing the heart rate. It was also thought that the extracardiac vascular actions of digitalis might be responsible for its therapeutic effect. It has now been established that cardiac glycosidescause arteriolar and venous constriction in a variety of mammalian species including human beings, and that this vasoconstriction involves the coronary vascular bed as well, but it is believed that these actions are not responsible for any beneficial clinical effect. A variety of investigations on cardiac muscle in vitro, anesthetized and conscious dogs and anesthetized and conscious human subjects have shown that cardiac glycosides improve the contractility of failing mammalian myocardium. It has become clear that digitalis also stimulates the contractility of the nonfailing heart. The degree of augmentation of contractility induced by cardiac glycosides is related inversely to the baseline contractile state. Myocardial oxygen consumption, which is increased in the normal heart by the positive inotropic action of glycosides, is actually reduced or remains constant in the failing heart. Cardiac glycosides increase the contractility of the globally ischemic William Withering (1) was well aware that digitalis is effective only in certain forms of dropsy , but because edema had not been clearly identified as a cardinal manifestation of heart failure two centuries ago, he did not associate this clinical effect with the cardiac actions of the drug. However, Withering did recognize that the drug causes an improvement in the pulse, and he stated that digitalis " has a power over the motion of the heart with a degree yet unobserved in any other medicine" (1) . Fourteen years later, John Ferriar correctly ascribed a primary effect of digitalis on the heart and assigned secondary importance to its diuretic actions (2). Subsequently , on the basis of auscultatory studies, From the Departments of Medicine. Harvard Medical School, Brigham and Women 's Hospital and Beth Israel Hospital, Boston, Massachusetts. Address for reprints: Eugene Braunwald , MD, 75 Francis Street, Boston, Massachusetts 02115. © 1985 by the American College of Cardiology heart, but their actions in chronic ischemic heart disease with regional impairment of function are complex. Deterioration of segmental performance occurs in ischemic and necrotic segments, while improvement of contractility occurs in adjacent normal segments. A modest improvement in left ventricular pump performance occurs in patients with chronic ischemic heart disease with impairment of global left ventricular function. There has been considerable debate concerning the clinical value of digitalis therapy in heart failure. Simple withdrawal of digitalis resulted in no clinical deterioration in many patients with mild to moderate heart failure. However, in patients with more severe impairment of cardiac function, aggravation of heart failure occurred after digitalis withdrawal, and striking clinical improvement was noted when the drug was readministeredo Thus, cardiac glycosides are relatively weak inotropic agents, have a low therapeutic ratio and are moderately effectivein heart failure secondary to ventricular volume overload. However, when properly used in patients with severe heart failure and sinus rhythm, particularly in patients with atrial fibrillation, cardiac glycosides improve both cardiac performance and the clinical state and can be administered effectively for years. Am Coli CardioI1985;5:51A-59A) a Bouillard (3) reported that a rapid and irregular pulse was improved by digitalis, which he considered to be "opium" for the heart. By the latter half of the 19th century , it was well recognized that digitalis enhances ventricular contraction (4). It had also become clear that digitalis glycosides exert a powerful beneficial clinical effect on patients with heart failure who had atrial fibrillation and a rapid ventricular rate, but it was believed that the drug exerted its clinical effect in such patients primarily by slowing the heart rate. Actions on the Vascular Bed Normal subjects. Early in this century it was suggested that a principal circulatory action of digitalis might be extracardiac, and that the direct effects of the drug on the vascular bed might be mainly responsible for its therapeutic action (5). More recently it was established that cardiac glycosides do exert a distinct direct action on the vascular 0735-1097/85/$3.30 BRAUNWALD CLINICAL EFFECTS OF DIGITALIS S'lA lACC Vol. 5, No. 5 May 1985:5IA-59A bed; they cause arteriolar and venous constriction in anesthetized dogs (6,7) and human subjects (8) (Fig. l) as well as in conscious normal humansubjects (9). In the conscious dog ouabain causes markedelevationof coronary and total systemic vascular resistance (10). Although cardiac glycosides have a local direct action on vascular smooth muscle, they also act indirectly by causing neurogenically mediated coronary vasoconstriction (2). Patients with heart failure. In patients with congestive heart failure, baseline levels of total cardiac output and forearm blood flow are lower, whereas total and forearm vascularresistances and venous tone are higher than in normal subjects (9). In such patients, the effect of ouabain on the vascular bed is directionally opposite to that observed in normal subjects; that is, it causes reductions of total systemic forearm vascular resistance and forearm venous tone (9). It is likelythat these vasodilator actionsare indirect and result from the reduction of reflex sympathetically mediated arteriolar and venoconstriction that occurs as a consequenceof the elevation of cardiac output induced by digitalis in patients with heart failure. It now appears that rather than being responsible for the beneficial effects of these drugs, the systemic and coronary vascularconstriction producedby rapidly acting glycosides given intravenously mayactually be responsible for a variety of complications (11,12) including acute exacerbation of heart failure. The vasoconstrictor effect of digitalis has a morerapid onset than its inotropic action(8). Thus, to avoid systemic and coronary vasoconstriction when rapidly acting glycosides are indicated, intravenous administration as a bolus should generally be avoided, particularly in patients with ischemic heart disease. Figure 1. Recording of brachial artery pressure in a 27 year old woman during repair of an atrial septal defect using cardiopulmonary bypass at a constant systemic perfusion rate. Arterial pressure, which at a constant perfusion rate reflects systemic vascular resistance, begins to increase 20 seconds after the injection of acetylstrophanthidin. Seven minutes after injection the pressure has already fallen, and 12 minutes after injection it is only slightly higher than the control level. (Reproduced with permission from Braunwald E, Bloodwell RD, Goldberg LI, Morrow AG. Studies on digitalis. IV. Observations in man on the effects of digitalis preparations on the contractility of the non-failing heart and on total vascular resistance. J Clin Invest 1961;40:52-9.) Effects on the Failing Heart Atrial fibrillation versus sinus rhythm. It is now beyond dispute that the digitalis glycosides display efficacy, both immediately and over the long term, in the control of heart failure and ventricular rate in patients with atrial fibrillation, Indeed, the development of an increase in atrioventricular block resulting in slowing of an excessive ventricular rate remains a principal indication for the use of digitalis (13). However, Christian (14) and other investigators suggested early in this century that this drug may also be effective in the treatment of patients with heart failure and sinus rhythm. Although cardiac glycosides are still advocated as the principal inotropic agents for the treatmentof heartfailure (13), and although studiesofthe effects of their short-term administration to patientshave confirmed that they improve myocardial performance in patients with heartfailure and sinusrhythm(15), thereis stillconsiderable controversy about whether patients with sinus rhythm who receive maintenance therapyderive clinical benefit (16). To understand this controversy, it is necessary to reviewseveral aspects of the action of this drug. Inotropic action of digitalis. The modem era of digitalis pharmacology began in 1940 when Gold and Cattell (17) demonstrated that digitalis increases the contractility of failing isolated cat papillary muscle in a dose-dependent manner (Fig. '-). Subsequently, it was shown that digitalis also improves the function of the failing heart-lung preparation of the dog (18). It is now clear that the extent of the positive inotropic action of the drug is related inversely to the baseline condition of the myocardium, cardiac muscle with depressed function showing a more vigorous response to the glycoside than normally contracting myocardium. These observations on the direct positive inotropic actions of cardiac glycosides have been extended to human subjects, and it has been demonstrated (19) that the contractility of papillary muscle removed from patients with heart failure, as reflected in the time-tension and forcevelocity relations, is enhanced by the addition of strophanthidin(Fig. 3). Hemodynamic studies(2,13,15) haveshown that when glycosides are administered to patients with heart failure, they elevate the ventricular function curve, causing a reduction in ventricular end-diastolic pressureand volume and an augmentation of cardiac output and stroke work. .-• S/I.I" "'''' HlJ 120 BRACHIAL ARTtIW PR£SalRE .......JtAI;!II . ., 40. .... .........;r .... 80~ t ACFTYLSTROPHANTHI»N I.S"'9 II". lACC Vol. 5, No.5 BRAUNWALD CLINICAL EFFECTS OF DIGITALIS May 1985:51A-59A 11.30 11:25 4:15 2:00 5:21 OUABAIN rrrrrr mrrnrrmr fffrm nrm ~m 4:40 5:20 5:35 5:55 8:15 6:44 Figure 2. The effect of ouabain on force of contraction of an isolated papillary muscle from the right ventricle of a cat heart. (Reproduced from [17) with permission.) Effects on the Nonfailing Heart While there is now general agreement regarding the positive inotropic effect of digitalis in the failing heart, there has been considerable dispute concerning its actions on the normal heart and the nonfailing though diseased heart. DigFigure 3. The effect of the addition of strophanthidin on the forcevelocity relation of a human left ventricular papillary muscle studied in vitro. The addition of strophanthidin increased both Vmax and Po (the maximal force of isometric contraction, that is, intercept on the abscissa), while decreasing the time from stimulation to maximal shortening from 390 to 340 ms. (Reproduced with permission from Sonnenblick EH, Braunwald E, Morrow AG. Contractile properties of human heart muscle: studies on myocardial mechanics of surgically excised papillary muscles. J Clin Invest 1965;44:966-77.) Slrophonlhidin 6 'U ....~ 5 o contra! • Slrop/lonlhidin o.5p/cc E E ;;4 z J.S. OS-/~-/7 z ~4,~ ~ FfllICI cl." II w RHOl Mil ~ 3 R.,~" :I: Ul 15 >- ~ u 2 ooJ w > o 4 6 53A italis does not increase the cardiac output at rest or during exercise in subjects without heart failure (20), but its cardiac stimulating action is reflected in the finding that the same levels of cardiac output and stroke work are delivered from a lower ventricular filling pressure or during a shorter period of time, or both. Several other lines of evidence indicate that cardiac glycosides do indeed exert a positive inotropic effect on nonfailing cardiac muscle. The effects of the longterm administration of digitoxin on the contractile state of nonfailing myocardium were studied in papillary muscles obtained from normal cats and from cats in which ventricular hypertrophy had been produced by banding of the pulmonary artery (21). While the muscle's length-tension relations at rest were not affected by the glycoside, the isometrically developed force and the maximal rate of force development were increased in both normal and nonfailing hypertrophied myocardium. Canine studies. In investigations on the conscious dog, it was found that at similar heart rates and left ventricular end-diastolic pressures, the long-term administration of digoxin increased left ventricular force, maximal rate of rise of left ventricular pressure (dP/dt) and the velocity of myocardial shortening (22). McRitchie and Vatner (23) also showed that in normal conscious dogs ouabain increases arterial pressure as well as indexes of myocardial contractility, such as left ventricular dP/dt divided by pressure ([dP/dt]/P) and the velocity of fiber shortening. The positive inotropic effect of the drug was also reflected in its ability to maintain stroke volume and to reduce left ventricular endsystolic dimensions at a constant preload, despite an increase in arterial pressure. However, in the intact heart of the conscious dog (for example, in isolated cardiac muscle), the degree of the augmentation of contractility induced by cardiac glycosides is related inversely to the baseline contractile state. Thus, in the normal conscious dog, when myocardial contractility is stimulated by adrenergic activity, as occurs during exercise, cardiac glycosides exert only a negligible positive inotropic effect (24). Conversely, the inotropic effects of glycosides are more prominent in the failing than in the nonfailing heart; the effects of ouabain on right ventricular segment length, pressure, velocity of shortening and (dP/dt)/P were studied in conscious dogs before and after the induction of chronic right heart failure (25). Although ouabain exerted an inotropic effect in normal healthy, conscious dogs, this effect was substantially greater in the presence of chronic heart failure (Fig. 4). Similarly, acute depression of myocardial function in the normal dog induced by sodium pentobarbital or large doses of propranolol enhanced the inotropic effects of ouabain (Fig. 5) (26). There is also evidence that cardiac glycosides elevate the performance of the canine heart when the latter is depressed by halothane (27) or thiopental (28) and reduce the oxygen debt after exercise in patients with cardiac enlargement but without heart failure (29). BRAUNWALD CLINICAL EFFECTS OF DIGITALIS 54A lACC Vol. 5, No.5 May 1985:5I A- 59A OUABAIN MYOCARDIAL <> +40[ +20 ,.- /./ -_2.:':~~/J ..... --....--......- ......... AFTER CHF -...._- ... ~-6- - - 3mi n ' 41 SeCJ + + 40[ 20 ~~ ::::~~:i' CO NT ROL ....-_..... _-...... ~~~:::~-~~-""._- - , "" 30 60 TIME (MINUTES) 0 90 120 Figure 4. Comparison of the effects of ouabain in the same conscious dog before (triangles) and after (circles) congestive heart failure (CHF) had been induced. Not only was the peak effect greater but the positive inotropic action of the drug was more sustained in the failing heart. Baseline measurements are shown at the left. VISO = velocity of shortening at the same length (isolength). (Reproduced with permission of the American Heart Association, Inc. from VatnerSF, Braunwald E. Effects of chronic heart failure on the inotropic response of the right ventricle of the conscious dog to a cardiac glycoside and tachycardia. Circulation 1974;50:728-34.) Human studies. The effects of digitalis on the force of contraction of the nonfailing human heart were studied using a force transducer sewn to the right ventricle of patients without heart failure undergoing cardiopulmonary bypass (8). Both acetylstrophanthid in and lanatoside C produced a Figure 5. The average (± SEM) values for the quotient of dP/dt and developed left ventricular (LV) pressure, an index of myocardial contractility, before and 30 minutes after ouabain for conscious dogs (left panel), afteranesthesia (middle panel) andconsciousdogs after propranolol (rightpanel); thesmallest augmentation occurs in the normal conscious dog (left panel). (Reproduced with permission from Vatner SF, Higgins CB. Patrick T, Franklin D. Braunwald E. Effects of cardiac depression and of anesthesia on the myocardial action of a cardiac glycoside. J Clin Invest 1971;50:2585-95.) 70 -=-, ANESTHETIZED CONSCIOUS l 0 CIl lfl W PROPRANOlOL 11 S EM 60 tr :::> VI VI w tr 50 a. -0 .....0.. "0 0 W a. 9 w 40 > w 0 ~ 30 5 min 7m in 10 min 15min ACETYLSTROPHANTHIDIN 1.5 mv V ' SO ( "i.. ll. ) o FORCE ir---.l BEFORE CHF dP~d !.- o, ll.) o CON TRACTILE CONTROL OUABAIN CONTROL OUABAIN Figure 6. Right ventricular contractile force recordings immediately before and at intervals after the administration of 1.5 mg of acetylstrophanthidin in a 27 year old woman with atrial septal defect (same patient as in Fig. I). Augmentation of contractile force is evident 3 minutes after injection. (Reproduced with permission from Braunwald E, Bloodwell RD, Goldberg LI, Morrow AG. Studies on digitalis. IV. Observations in man on the effects of digitalis preparations on the contractility of thenon-failing heart and on total vascular resistance. J Clin Invest 1961;40:52-9.) prompt increase in isometric force development, indicating that the digitalis glycosides do stimulate the nonfailing heart of anesthetized human patients (Fig. 6). These studies were then extended to' conscious human subjects without heart failure in whom the measurement of maximal dP/dt was recorded using a high fidelity rnicromanometer catheter; ouabain increased both right and left ventricular dP/dt (Fig. 7) (30). The results of several additional studies on the action of cardiac glycosides on nonfailing human myocardium are in accord wiith these findings. Thus. the effects of ouabain on ventricular force-velocity relations were studied in conscious patients without heart failure who had previously undergone corrective cardiac operations, at which time radiopaque markers had been sewn to the external surfaces of the ventricle (31). The glycoside augmented myocardial contractility, simultaneously increasing velocity of shortening and intraventricular pressure (Fig. 8). Crawford et at. (32) examined the effects of digoxin on left ventricular function in normal subjects using echocardiography. They observed a positive inotropic action, as reflected in an increase in the left ventricular ejection fraction and an augmentation of the extent and rate of left ventricular shortening as well as significant improvement in left ventricular performance after acute pressure loading. The observations just summarized indicate quite clearly that digitalis glycosides stimulate the contractility of the nonfailing human heart. However , these drugs do not affect cardiac output at rest or maximal levels of oxygen uptake, pulmonary ventilation or heart rate in normal subjects (20) . Therefore, adjustments of the other determinants of cardiac output, such as preload, afterload and heart rate, prevent this increase in contractility from being translated into an augmentation of cardiac output (33). There is no evidence that the administration of digitalis is of any clinical value in patients with sinus rhythm without heart failure and its administration prophylactically to such patients is not ordinarily indicated (13). BRAUNWALD CLINICAL EFFECTS OF DIGITALIS lACC Vol. 5, No.5 May 1985:5IA-59A OUABAIN 0 .6 mg. CONTROL 1005mm Hlj/sec. dp/dt Figure 7. Recordings of left ventricular (LV) pressure and rate of change of pressure (dP/dt) before and30 minutes after ouabain administration in a patient without heart failure . EKG = electrocardiogram . (Reproduced with permission from Mason OT. Braunwald E. Studies on digitalis. IX . Effects of ouabain on the non-failing human heart. J Clin Invest 1963; ""ft. Hlj/St< 1495 mm. Hglsec. f I '~ 100 5 2000 1500 "1ft .... 1000 HljISoc. LV o 55A 500 ..Ill HQ 150 100 75 42: 1105-11 .) 25 '---l,_--~_'---"""oIo 0 ----..._""----le_'---~ EKG Effects in Myocardial Ischemia and Ischemic Heart Disease Figure 8. The effects of ouabain on the instantaneous force-velocity relations of the right ventricle (R.V,) of a conscious human subject with radiopaque markers implanted on the epicardium at the time of corrective surgery . The velocity of shortening of the segment of myocardium between themarkers at theisolength (ISL) point is plotted ontheordinate. Thecorresponding right ventricular pressure is plotted on the abscissa. Each point represents a single ventricular contraction, and the crossbars represent ± I SO. (Reproduced with permission of the American Heart Association . Inc. from Sonnenblick EH , Williams JF Jr, Glick G, Mason OT. Braunwald E. Studies on digitalis. XV. Effects of cardiac glycosides on myocardial force-velocity relations in the non-failing human heart. Circulation 1966;34:532-9.) • • •• • 7h •• u :: 5 <, '" '0 L: .. • c: --' 'al -s: z z w ~ 4 o J: Vl u, o >- lU o 0 ~ :3 0 > » ci a a ~ CONTROL 0 OUABAIN O.Olmo/Ko • a 40 35 R.V PRESSURE ISL 45 - mmH9 Myocardial oxygen consumption (MVO z). To understand the action of glycosides in myocardial ischemia and ischemic heart disease, it is useful, first, to consider their effects on MVOz. Because the MVOz is determined largely by intramyocardial tension. myocardial contractility and heart rate, the net action of digitalis on these three hemodynamic variables governs its effect on MVOz (34) . In anesthetized dogs without heart failure or cardiac dilation, digitalis augments myocardial contractility with little effect on intramyocardial tension and heart rate; therefore, it might be expected to, and indeed it does, elevate MVOz in the nonfailing heart. However, in the presence of heart failure, digitalis reduces ventricular volume and thereby intramyocardial tension. Heart rate may also be slowed in heart failure as a consequence of diminished sympathetic drive, and these two effects tend to balance the increase in MVOz resulting from augmented myocardial contractility; the net effect is to produce either no change or a small increase in MVOz (35). DeMots et al. (36) demonstrated in patients with chronic ischemic heart disease without heart failure that ouabain reduces left ventricular end-diastolic pressure and volume and augments the maximal velocity of estimated contractile element shortening; it causes no significant change in MVOz, presumably because of the opposing effects of the glycoside-induced reduction in tension and augmentation of contractility. Acute hypoxia, ischemia and infarction. There is considerable evidence that digitalis glycosides are capable of stimulating the acutely hypoxic or ischemic heart (37). Thus, in dogs in which severe systemic hypoxia was induced by respiring 7 to 10% oxygen, acetylstrophanthidin caused elevations of left ventricular dP/dt and stroke work that were distinct but smaller than the changes induced by identical doses of the drug in nonhypoxic animals (38). Similarly, Sarnoff et al. (39) reported that the intracoronary injection 56A BRAUNWALD CLINICAL EFFECTS OF DIGITALIS of acetylstrophanthidin into a globally ischemic isolated canine heart caused a marked improvement of cardiac contractility. In the conscious dog with acute coronary occlusion, ouabain improves global left ventricular performance (40), and in the nonfailing dog heart cardiac glycosides intensify the ischemia produced by coronary occlusion (41), presumably by augmenting myocardial oxygen requirements. However, in the failing heart, digitalis has the apposite effect (42); by reducing myocardial oxygen requirements. cardiac glycosides may reduce the severity 'of ischemia induced by coronary occlusion (Fig. 9) . The routine use of digitalis in the management of patients with acute myocardial infarction was first suggested by Herrick in 1912 (43) and the drug was initially employed widely in this condition (44). Subsequently, its use became more Figure 9. Average effecIs (:!: SEM) of ouabain on mean ST segment elevation and hemodynamic variables after coronary ligation and with arterial pressure increased in six anesthetized open chest dogs with experimentally produced heart failure. There is little effect on mean aortic pressure or heart rate . Ouabain caused a striking decline of markedly elevated mean left atrial pressure , accompanied by a striking reduction of ST segment elevation of the ischemic myocardium. (Reproduced with permission from Watanabe A, Covell JW. Maroko PR, Braunwald E, Ross J Jr. Effects of increased arterial pressure and positive inotropic agents on the severity of myocardial ischemia in the acutely depressed heart . Am J Cardiol 1972;30:371 -7.) 0....1---'---'-----'--'--- 150 rX '0 u:r ~1100 ~W ~iil 50 ",III 2'" f 0....1---'---'-----'--'--- 30l cf 20 SoJ !CO! ~'" ""c ~! ~W 10- ~A. O--'----'--L----'---'--- ...E elOO '" !c c ~ 50 c c '" :r 0 --I----'--=-'----=-~=-':-:-:-:-- c OUABAIN lACC Vol. 5, No.5 May 1985:5IA-59A controversial (37) . Thus , Cohn et al. (II) administered cardiac glycosides intravenously to patients with cardiogenic shock . They reported a short-term increase in systemic vascular resistance that was associated with the development of pulmonary edema in one patient. Later, there was an increase in myocardial contractility, as reflected in an increase in the left ventricular maximal dP/dt, usually accompanied by a decrease in the left ventricular end-diastolic pressure; however, cardiac output was not increased significantly . In patients with acute myocardial infarction and congestive heart failure without cardiogenic shock, several investigators (45,46) observed that digitalis increases ejection fraction slightly . Morrison et al. (47) also reported that in patients with acute myocardial infarction, digoxin causes a modest but significant elevation of a depressed ejection fraction (from 0.29 to 0.33). Chronic ischemic heart disease. Kleiman et al. (48,49) studied the effects of both intravenous and oral digoxin in patients with stable coronary artery disease without clinical evidence of heart failure after coronary artery bypass grafting. Using computer-assisted fluoroscopic analysis of the motion of markers implanted into the myocardium at operation, they observed that the ejection fraction and the velocity of circumferential fiber shortening both increased, while the left ventricular end-diastolic volume and cardiac output did not change significantly. The improvement in performance induced by digoxin was greater in normal myocardial segments than in segments that were contracting abnormally due to ischemia or fibrosis. Indeed, deterioration of segmental performance occurred in approximately half of the segments with depressed function, a deterioration that may be due to the inability of infarcted segments of myocardium to sustain the increased wall tension resulting from the digitalis-induced augmented contractility of the normal myocardium. Therefore, in patients with ischemic heart disease, the response of particular segments of the myocardium to cardiac glycosides appears to depend on the relative quantity of viable nonischemic muscle, on the one hand, and of ischemic or infarcted muscle in the particular segment, on the other. It has been suggested that it is the failure of ischemic and necrotic segments of the myocardium to respond to digitalis which is responsible for the lack of impressive improvement of left ventricular function in patients with acute myocardial infarction who are treated with the drug (50). In patients with chronic ischemic heart disease, the acute administration of digoxin had a mild beneficial effect on global left ventricular performance at rest, but did not alter the onset of exercise-induced angina or affect exerciseinduced deterioration of left ventricular function (51) . Similarly, Firth et al. (52) reported that digoxin did not cause any significant change in left ventricular function at rest in patients with ischemic heart disease. Although the glycoside prevented the exercise-induced increases in left ventricular BRAUNWALD CLINICAL EFFECTS OF DIGITALIS IACC Vol. 5. No.5 May 1985:5IA-59A end-diastolic and end-systolic volumes in patients with a normal ejection fraction at rest, it failed to do so in patients with a depressed ejection fraction. Thus, the positive inotropic effects of long-term digoxin therapy could be demonstrated more readily in patients with chronic ischemic heart disease whose left ventricular function was well preserved than in those with an extensive infarct. These observations support those of Kleiman et al. (48,49) and suggest that the extent of improvement of left ventricular function by glycosides in chronic ischemic heart disease without overt heart failure depends on the relative quantities of well preserved and extensively damaged myocardium. In light of the foregoing data, there is little doubt that cardiac glycosides can improve myocardial performance in patients with ischemic heart disease. The degree of improvement, however, varies among different patients and in different portionsof the ventriclein anyone patient. Thus, glycosides cause no improvement or can even result in systolic expansionof severelyischemic or scarredmyocardium. They cause only slight augmentation of contractility in normal myocardium that is adrenergically stimulated because of left ventricular failure as a consequence of extensive ischemia or infarction. Therefore, digitalis glycosides cause only modest improvement of global left ventricular function in heart failure occurring as a consequence of acute myocardial infarction. Indeed, transient acute deterioration of left ventricular function may occur when a rapidly acting glycoside is administered intravenously and elevates systemic vascular resistance and ventricular afterload acutely in patients with heart failure secondary to ischemic heart disease. Digitalis may cause a modest improvement of left ventricularpump performance in patients with chronic ischemic heart disease and impaired global left ventricularfunction. However, the salutary effects of glycosides on left ventricular pump function in such patients are less than in patients with left ventricular failure secondary to chronic ventricular volume overload, such as occurs in valvular regurgitation. Clinical Implications Mulrow et al. (53) recently provided a critical appraisal of the 16 articles published in English between 1960 and 1982 which specifically address the clinical evaluation of digitalis therapy in heart failure. In the nine studies in which the effects of simple withdrawal of digitalis therapy were studied, no consistent evidence of clinical deterioration was noted. However, because detailed criteria for patient selection were not provided in these studies, few conclusionscan be drawn from them. In three other investigations, the addition of digoxin was not found to have any beneficial effects over therapy with diuretic drugs alone. Arnold et al. (54) foundthat left ventricularfunctiondeterioratedafter digitalis withdrawal, whereas Gheorghiade and Beller (55), who 57A studied patients with chronic ischemic heart disease and heart failure who were also treated with diuretic drugs and vasodilators, reported that withdrawal of digoxin had no adverse clinical or hemodynamic effects. Murray et al, (56) reported that long-termtreatment with digitalis in patients with sinus rhythm and symptomatic cardiac failure caused little change in hemodynamic measurements at rest, but did result in lower left ventricular enddiastolic pressures and higher cardiac index and stroke work during exercise. These changes were observed both after the short-term administration of ouabain and long-term oral digoxin therapy. Fleg et al. (57) carried out a placebocontrolled crossover study with digoxin and reported that the withdrawal of digitalis in patients with compensated heart failure increased ventricular end-diastolic dimensions and decreased the velocity of fiber shortening, but did not cause a clinical exacerbation of heart failure. They concluded that the drug is of little benefit in elderly patients with stable congestive heart failure, because none manifested deterioration in the 3 months during which they received placebo in place of digoxin. Lee et al. (58) found that 14 of 25 patients with heart failure showed clinical improvement while receiving digoxin; improvement was most striking in patients with severe heart failure and a protodiastolic gallop. The majority of the patients whose condition did not improvewith digitalis might not have been expected to show improvement because they had a normal left ventricular ejection fraction at rest, were asymptomatic or had hypertrophic cardiomyopathy. Other Considerations Cardiac glycosides are relatively weak inotropic agents in comparison with catecholamines and the newer inotropic agents (the bipyridines, amrinone and milrinone) (59). In a comparison of the inotropic effects of isoproterenol and ouabain in the normal anesthetized dog (60), isoproterenol produced a peak increase in contractile force of approximately 160% of control, compared with an increase of only 50% resulting from the administrationof ouabain. However, the very fact that glycosides are relatively weak inotropic agents may make them particularly suitable for long-term administration because it is possible that prolongedvigorous stimulation of failing myocardium , that is, so-called "flogging" the failing heart, may be deleterious. Conclusions The cardiac glycosides have been used continuously in clinicalmedicinefor two centuries. Duringthe past 25 years, a great deal has been learned about the cellular mechanism of action of these drugs: these appear to result from an inhibition of sarcolemmal Na + -K + adenosine triphosphatase, which causes an augmentation of intracytoplasmic cal- 58A BRAUNWALD CLINICAL EFFECTS OF DIGITALIS cium concentration, which in tum is responsible for the stimulation of myocardial contractility. The positive inotropic action is seen in normal as well as in failing hearts, and has been demonstrated in isolated cardiac muscle, heartlung preparations, anesthetized and conscious dogs and human subjects. Although a positive inotropic action is present in the normal heart, it is not translated into an augmentation of a normal cardiac output or reduction of a normal left ventricular filling pressure. However, substantial hemodynamic benefits have been demonstrated in the dilated failing heart. The augmentation of contractility, as shown by an increase in both dP/dtJP and velocity of myocardial fiber shortening, is reflected by an improvement in pump performance, with an elevation of depressed cardiac output and a reduction of elevated ventricular filling pressure. Secondary vasodilation occurs, presumably as a consequence of the withdrawal of sympathetic stimulation characteristic of heart failure. Digitalis remains a mainstay ofthe therapy for congestive heart failure. Its effects are most prominent in heart failure associated with atrial fibrillation and a rapid ventricular rate, but it is also effective in severe heart failure and cardiac dilation secondary to volume overload, as well as in patients with a dilated, failing ventricle secondary to hypertension. Little improvement is observed in patients with left ventricular failure secondary to ventricular outflow tract obstruction (aortic or pulmonary stenosis) or in patients with acute left ventricular failure secondary to myocardial ischemia or infarction, or both. When it is administered in proper doses and for the proper indications, glycoside therapy may be well tolerated by a patient for decades. Therefore, despite its modest inotropic action and therapeutic ratio, digitalis remains a useful drug in the therapy of many patients with chronic congestive heart failure. References I. Withering W. An Account of the Foxglove, and Some of Its Medical Uses: With Practical Remarks on Dropsy and Other Diseases. Birmingham, England: M. Swinney, 1785. 2. Hoffman BG, Bigger JT Jr. Digitalis and allied cardiac glycosides. In: Gilman AG, Goodman LS, Gilman A, eds. The Pharmacologic Basis of Therapeutics. New York: Macmillan, 729-60. 3. Bouillard J. Traite Clinique des Maladies du Cour. Paris: 1835. 4. Fothergill JM. Digitalis: Its Mode of Action. London: 1871. 5. Dock W, Tainter ML. The circulatory changes after full therapeutic doses of digitalis, with a critical discussion of views on cardiac output. J Clin Invest 1930;8:467-84. 6. Ross J Jr, Waldhausen JA, Braunwald E. Studies on digitalis. I. Direct effects on peripheral vascular resistance. J Clin Invest 1960;39:930-6. 7. Ross J Jr, Braunwald E, Waldhausen JA. Studies on digitalis. II. Extracardiac effects on venous return and on the capacity of the peripheral vascular bed. J Clin Invest 1960;39:937-42. 8. Braunwald E, Bloodwell RD, Goldberg LI, Morrow AG. Studies on digitalis. IV. Observations in man of the effects of digitalis preparations on the contractility of the nonfailing heart and on total vascular resistance. J Clin Invest 1961;40:52-9. lACC Vol. 5, No.5 May 1985:51A-59A 9. Mason DT, Braunwald E. Studies on digitalis. X. Effects of ouabain on forearm vascular resistance and venous tone in normal subjects and in patients with heart failure. J Clin Invest 1964;43:532-43. 10. Vatner SF, Higgins CB, Franklin D, Braunwald E. Effects of a digitalis glycoside on coronary and systemic dynamics in conscious dogs. Circ Res 1971;28:470-9. I I. Cohn IN, Tristani FE, Khatri 1M. Cardiac and peripheral vascular effects of digitalis in clinical cardiogenic shock. Am Heart J 1969;78:3I8-30. 12. Baleon R, Hoy J, Sowton E. Haemodynamic effects ofrapid digitalization following acute myocardialinfarction. Br Heart J 1%8;30:373-6. 13. Smith TW, Braunwald E. The management of heart failure. In: Braunwald E, ed. Heart Disease: A Textbook of Cardiovascular Medicine. 2nd ed. Philadelphia: WB Saunders 1984:503-59. 14. Christian MH. Digitalis therapy. Satisfactory effects in cardiac cases with regular pulse rate. Am J Med Sci 1919;157:593-602. 15. Bloomfield RA, Rapoport B, Milnor JP, Long WK, Mebane JG, Ellis LB. Effects of cardiac glycosides upon dynamics of circulation in congestive heart failure. Ouabain. J Clin Invest 1948;27:588. 16. Hamer J. The paradox of the lack of the efficacy of digitalis in congestive heart failure with sinus rhythm. Br J Clin Pharmacol 1979;8:109-13. 17. Gold H, Cattell M. Mechanism of digitalis action in abolishing heart failure. Arch Intern Med 1940;65:263-78. 18. Farah A, Maresh G. Determination of the therapeutic irregularity, and lethal doses of cardiac glycosides in the heart-lung preparation of the dog. J Pharmacol Exp Ther 1948;92:32-42. 19. Sonnenblick EH, Braunwald E, Morrow AG. The contractile properties of human heart muscle: studies on myocardial mechanics of surgically excised papillary muscles. J Clin Invest 1965;44:966-77. 20. Williams MH Jr, Zohmar LR, Ratner AC. Hemodynamic effects of cardiac glycosides on normal human subject during rest and exercise. J Appl Physiol 1958;13:417-21. 21. Williams JF Jr, Potter RD. The effect of chronic digitoxin administration on the contractile state of normal and nonfailing hypertrophied myocardium. J Clin Invest 1975;56:71-8. 22. Mahler F, Karliner JS, O'Rourke RA. Effects of chronic digoxin administration on left ventricular performance in the normal conscious dog. Circulation 1974;50:720-7. 23. McRitchie RJ, Vatner SF. The role of arterial baroreceptors in mediating the cardiovascular response to a cardiac glycoside in conscious dogs. Circ Res 1976;38:321-6. 24. Horowitz LD, Atkins JM, Saito M. Effect of digitalis on left ventricular function in exercising dogs. Circ Res 1977;41:744-50. 25. Vatner SF, Braunwald E. Effects of chronic heart failure on the inotropic response of the right ventricle of the conscious dog to a cardiac glycoside and to tachycardia. Circulation 1974;50:728-34. 26. Vatner SF, Higgins CB, Patrick T, Franklin D, Braunwald E. Effects of cardiac depression and of anesthesia on the myocardial action of a cardiac glycoside. J Clin Invest 1971;50:2585-95. 27. Goldberg AH, Maling HM, Gaffney TE. The value of prophylactic digitalization in halothane anesthesia. Anesthesiology 1962;23:207-12. 28. Goldberg AH, Maling HM, Gaffney TE. The effect of digoxin pretreatment on heart contractile force during thiopental infusion in dogs. Anesthesiology 1961;22:974-6. 29. Kahler RL, Thompson RH, Buskirk ER, Frye RL, Braunwald E. Studies on digitalis. VI. Reduction of the oxygen debt after exercise with digoxin in cardiac patients without heart failure. Circulation 1963;27:397-405. 30. Mason DT, Braunwald E. Studies on digitalis. IX. Effects of ouabain on the nonfailing heart. J Clin Invest 1963;42:1105-1 I. 31. Sonnenblick EH, Williams JF Jr, Glick G, Mason DT, Braunwald E. Studies on digitalis. XV. Effects of cardiac glycosides on myocardial force-velocity relations in the nonfailing human heart. Circulation 1966;34:532-9. l ACC Vol. 5, No. 5 May 1985:5I A-5 9A BRAUNWALD CLINICAL EFFECTS OF DIGITALIS 59A 32. Crawford MH, Karliner JS , O 'R ourke RA, Amon KW. Favorable effects of oral maintenance digoxin therapy on left ventricular performance in normal subjects: echocardiographic study . Am J Cardiol 1976:38:843-7 . 48. Kleiman JH, Ingels NB , Daughters G, Stinson EB, Alderman EL, Goldman RH. Left ventricular dynamics during long-term digoxin treatment in patients with stable coronary artery disease. Am J Cardiol 1978:4 1:937-42. 33. Braunwald E. On the difference between the heart's output and its contractile state. Circulat ion 1971 :43 :171-4. 49. Kleiman JH, Alderman EL, Goldman RH. Effects of digitalis on normal and abnormal left ventricular segmental dynamics. Am J Cardiol 1979;43:1001-8. 34 . Braunwald E. Control of myocardial oxygen consumption: physiologic and clinical considerations. Am J Cardiol 197 1;27:416-32. 35. Cove ll JW , Braunwald E, Ross J Jr , Sonnenblick EH. Studies on digitalis. XVI. Effects on myocardial oxygen consumption. J Clin Invest 1966;45: 1535-42. 36 . DeMots H, Rahimtoola SH , Kremkau EL, Bennett W, Mahler D. Effects of ouabain on myocardial oxygen supply and demand in patients with chronic coronary artery disease. J Clin Invest 1976:58:312- 9. 37. Karliner JS , Braunwald E. Present state of digitalis treatment of acute myocardial infarction. Circulati on 1972 :45:891-902. 38. Donlon JV, Yu PN. Cardiovascular response of hypoxic myocardium to acetyl strophanthidin. Am Heart J 1969:78:238-44. 39 . Sarnoff SJ, Gilmore JP, Wallace AG , Skinner NS Jr, Mitchell JH, Daggett WM . Effect of acetyl strophanthidin therapy on cardiac dynamics. oxyge n consumpti on and efficiency in the isolated heart with and without hypoxia. Am J Med 1964;37:3-11. 50. Hodges M, Friesinger GC, Riggins RCK, Dagenais GR . Effect of intravenously administered digoxin on mild left ventricular failure in acute myocardial infarction in man. Am J Cardiol 1972;29:749- 55 . 51. Verani MS, Zacca NM, Miller RR, Luchi RJ, Chahine RA. Effects of digoxin on left ventricular function in coronary artery disease patients. Int J Cardiol 1982:2:221- 3 1. 52. Firth BG, Dehmer OJ, Corbett JR , Lewis SE, Parkey RW, Willerson JT. Effect of chronic oral digoxin therapy on ventricular function at rest and peak exercise in patients with ischemic heart disease. Assessment with equilibrium gated blood pool imaging. Am J Cardiol 1980;46:481-9. 53. Mulrow CD, Feussner JR, Velez R. Reevaluation of digitalis efficacy . New light on an old leaf. Ann Intern Med 1984;101: 113-7. 54 . Arnold SB, Byrd RC, Meister W. Long-term digitalis therapy improves left ventricular function in heart failure. N Engl J Med 1980;303:1443-8. 40 . Vatner SF, Baig H. Comparison of the effects of ouabain and isoproterenol on ischemic myocardium of conscious dogs. Circulation 1978;58:654-62. 55. Gheorghiade M, Beller GA . Effects of discontinuin g maintenance digoxin therapy in patients with ischemic heart disease and congestive heart failure in sinus rhythm. Am J Cardiol 1983;51:1243-50. 4 1. Maroko PR, Kjekshus JK , Sobel BE, et at. Factors influencing infarct size following experimental coronary artery occlusion. Circulation 1971 ;43:67- 82. 56 . Murray RG. Tweddel AC, Martin W , Pearson 0 , Hutton I, Lawrie TDV. Evaluation of digitalis in cardiac failure . Br Med J 1982: 284:1526-8 . 42. Watanabe T , Covell JW . Maroko PR, Braunwald E, Ross J Jr. Effects of increased arterial pressure and positive inotropic agents on the severity of myocardial ischem ia in the acutely depressed heart. Am J Cardiol 1972:30:371-7 . 57. Fleg JL, Gottlieb SH . Lakatta EG. Is digoxin really important in treatment of compensated heart failure? A placebo-controlled crossover study in patients with sinus rhythm . Am J Med 1983;73:244-50. 43 . Herrick JB. Clinical features of sudden obstruction of the coronary arteries. JAMA 1912;49:2015- 7. 44 . Hamman L. The symptoms of coronary occlusio n. Johns Hopkins Med J 1926 ;38:273-5. 45 . Bostrom PA, Andersson J , Johansson BW, et at. Haemodynami c effects of prenaterol and cardiac glycosi des in patients with recent myocardial infarction. Eur J Clin Invest 1984;14:175-80. 46. Marchionni N, Vannucci A, Pini R, et at. Hemodynamic effects of digoxin in acute myocardial infarction. Eur Heart J 1980;1:319-26. 47 . Morrison J. Coromilas J, Robbins M, et at. Digitalis and myocardial infarction in man . Circulation 1980;62:8-1 6. 58. Lee DC, Johnson RA, Bingham JB. Heart failure in outpatients: a randomized trial of digoxin versus placebo. N Engl J Med 1982; 306:699- 705. 59 . Braunwald E, Sonnenbl ick EH. Chakrin LW, Schwartz RP Jr, eds. Milrinone: Investigation of New Inotropic Ther apy for Congestive Heart Failure. New York: Raven , 1984 . 60 . Beiser GO . Epstein SE . Goldstein RE , Stampfer M. Braunwald E. Comparison of the peak inotropic effects of a catecholamine and a digitalis glycoside in the intact canine heart. Circulation 1970;42:805-13.