Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Vasopressin wikipedia , lookup
Hormone replacement therapy (female-to-male) wikipedia , lookup
Neuroendocrine tumor wikipedia , lookup
Sex reassignment therapy wikipedia , lookup
Hypothyroidism wikipedia , lookup
Signs and symptoms of Graves' disease wikipedia , lookup
Bioidentical hormone replacement therapy wikipedia , lookup
Hyperandrogenism wikipedia , lookup
Hormone replacement therapy (menopause) wikipedia , lookup
Hormone replacement therapy (male-to-female) wikipedia , lookup
Hyperthyroidism wikipedia , lookup
Graves' disease wikipedia , lookup
Kallmann syndrome wikipedia , lookup
Hypothalamus wikipedia , lookup
Pituitary apoplexy wikipedia , lookup
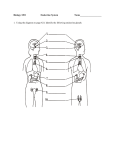
Endocrinology 1a –Anterior -Pituitary Disorders Anil Chopra 1. Define the term pan-hypopituitarism (Simmond’s disease) and describe the specific aetiology of the form of hypopituitarism called Sheehan’s syndrome. 2. Describe the more common signs and symptoms of pan-hypopituitarism. 3. Describe how a) anatomical pituitary disruption and b) pituitary hormone deficiency can be evaluated, including the use of stimulation tests. 4. Describe how the endocrine consequences of pan-hypopituitarism can be treated, using the term hormone replacement therapy 5. List the various possible individual pituitary hormone deficiencies that can occur and explain how the conditions can be diagnosed and treated (when appropriate). 6. List the principal endocrine causes of short stature, identifying those that are caused by lack or excess of specific hormones and those that are related to receptor and post-receptor defects (e.g. Laron dwarf). 7. State that short stature can also be related to non-endocrine causes such as malabsorption, malnutrition and psychological deprivation. 8. Explain how the diagnosis of endocrine-related short stature can be made, including a description of the use of standard growth charts and stimulation tests. 9. Explain why provocative tests are useful in the diagnosis of pituitary insufficiency. Give examples of tests used to diagnose GH deficiency. 10. Describe the pharmacodynamic and pharmacokinetic properties of human growth hormone (hGH) and explain the rationale governing its use in the treatment of GH deficiency in (a) children and (b) adults. As the hypothalamo pituitary axis is a 3 hormone system – disorders can occur in any stage: 1) Endocrine gland Primary endocrine gland disease 2) Anterior Pituitary Secondary endocrine gland disease 3) Hypothalamus Tertiary endocrine gland disease Somatotrophin Releasing Hormone (SRS, GHRH) Somatostati n + _ Somatotrophin (GH) + _ IGF-1 Dopamine (DA) Thyrotrophin Releasing Hormone (TRH) _ Ghrelin + GHRP Prolactin + Thyrotrophin + Corticotrophin Releasing + Corticotrophin (ACTH) Hormone (CRH) + + Ghrelin Vasopressin (VP) + Gonadotrophin Luteinizing Hormone Releasing Hormone + (LH) (GnRH) Follicle Stimulating Hormone (FSH) Adenohypophysial Hormones and their main target cells: Somatotrophin → General body tissues, particular they liver Prolactin → Breasts, particularly in lactating women Thyrotrophin → Thyroid Gonadotrophins → Testes in men, ovaries in women Corticotrophin → Adrenal Cortex Hypopituitarism PANHYPOPITUITARISM all pituitary gland has decreased production. This is a gradual reduction of pituitary secretion including: - Gonadotrophin disorders - Growth hormone - Thyrotrophin - Corticotrophin - Occasionally prolactin although this is uncommon. Signs and Symptoms of Pan- Hypopituitarism Secondary amenorrhoea or oligomenorrhoea in women Impotence in men Tiredness Waxy skin Loss of body hair Hypotension Loss of libido Testing for Pituitary Disorder Measurement of the basal levels of pituitary or primary endocrine gland hormones – compare to normal Use of provocation (stimulation) tests – e.g. a combined function test involving rapid and sequential infusion of GHRH, CRH, GnRH, and TRH Specific tests for individual hormones – e.g. insulin-induced hypoglycaemia for GH Types: Simmonds disease: slow onset o Causes: infiltrative processes, head injury, pituitary adenomas or cranial injury after surgery. o Symptoms: gradual loss of thyroid, adrenal and gonadal function e.g. loss of periods, loss of libido, hypotension, tiredness, loss of body hair, impotence, waxy skin. o Diagnosis: measure plasma hormone values, stimulate endocrine hormones themselves (i.v.) and then measuring hormones levels. e.g. insulin-induced hypoglycaemia for GH o Treatment: Hormone replacement therapy. Sheehan’s Syndrome: (specific to WOMEN) sudden onset due to ischaemia of pituitary. o Causes: post partum haemorrhage resulting in pituitary infarction. The blood loss results in the hypophysial arteries vasoconstricting which results in the ischaemia and necrosis is of the pituitary tissue. Pituitary Apoplexy: similar to Sheehan’s in that intra-pituitary haemorrhage can occur with an often dramatic presentation in patients with pre-existing pituitary tumours which suddenly infarct. If there is a deficiency in a particular hormone, then secondary hypopituitarism develops. These can generally be treated with hormone replacement therapy. HYPOGONADISM lack of Gonadotrophins. HYPOTHYROIDISM lack of Thyrotrophin HYPOADREONO-CORTICALISM lack of corticotrophin PITUITARY DWARFISM lack of Somatotrophin in children. In adults, the effects are uncertain. NB: the most important hormone to replace is cortisol (life threatening) followed closely by thyroxine Causes of Short stature: - genetic predisposition - malnutrition - emotional deprivation - endocrine disorders Congenital - deficiency of GHRH - mutations of GH gene - developmental abnormalities of pituitary gland. Acquired - tumours of hypothalamus or pituitary (disrupt GH production) - other intracranial tumours nearby (e.g. optic nerve glioma) - secondary to cranial irradiation - head injury - infection or inflammation - severe psychosocial deprivation Laron dwarfism = GH receptor deficiency in the liver. SOME CAUSES OF ENDOCRINE-RELATED SHORT STATURE hypothalamus adenohypophysis liver IGFI I GH receptor defect LARON DWARFIS M IGF IGFI receptor I defect PYGM Y target tissues Diagnosis Mainly used as a confirmation after a preliminary guess GH Provocation Tests: Insulin Induced Growth Hormone secretion Give i.v. GHRH (tells you whether deficiency is hypothalamic or pituitary) Give i.v. arginine (an amino acid) Exercise induced growth hormone secretion SS GHRH SOMATOTROPHIN (GROWTH HORMONE) Lack of GH HYPOPITUITAR Y DWARFISM SS IGFI GH Lack PYG LARO HYPO IGFI IGFII aden GHR hypo targe liver SO of GH recept N PITUI MY SOM ohyp H thala t ME or DWA TARY ATOT ophy mus tissu defect RFIS DWA CA ROP sis es M RFIS HIN US M (GRO ES WTH HOR OF MON EN E) DO CRI NEREL ATE D SH OR T STA TU RE Treatment: Hormone replacement Growth hormone therapy in Children: Acceleration of linear growth Decreases body fat. Effects are most marked in the first year of treatment Younger children respond better Obese children respond better Resistance may develop due to antibody formation Give human recombinant growth hormone o Somatotropin Given intramuscular or subcutaneous Daily or 4-5 times per week – adjust dose to size Plasma concentration takes effect between 2-6 hrs Metabolised in liver/kidney Short half life of 20 mins Lasts long time – peak effect around 20 hours Side effects o Lipoatrophy (loss of fat) at site o Intracranial hypertension o Headaches o Increased incidence of leukaemia. GH Deficiency in Adults Signs Reduced lean mass Reduced muscle strength & bulk reduced exercise performance Decreased plasma HDL-cholesterol & raised LDL-cholesterol Impaired ‘psychological well being’ and reduced quality of life Diagnosis Lack of responose of GH stimulation test Low plasma IGF 1 Potential benefits of HRT Body composition increases Increases lean body mass Exercise capacity and strength increases Increase bone mineral content Psychological well being Normalisation HDL and LDL content. Risks Increase of cardiovascular accidents Increase size of soft tissue organs (liver) Stimulation of tumour development.