Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Adaptive immune system wikipedia , lookup
Hygiene hypothesis wikipedia , lookup
Drosophila melanogaster wikipedia , lookup
Psychoneuroimmunology wikipedia , lookup
Monoclonal antibody wikipedia , lookup
Human cytomegalovirus wikipedia , lookup
Hepatitis B wikipedia , lookup
Pathophysiology of multiple sclerosis wikipedia , lookup
Innate immune system wikipedia , lookup
Cancer immunotherapy wikipedia , lookup
DNA vaccination wikipedia , lookup
Infection control wikipedia , lookup
Adoptive cell transfer wikipedia , lookup
Hospital-acquired infection wikipedia , lookup
Immunosuppressive drug wikipedia , lookup
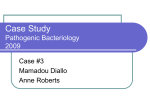
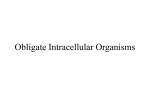
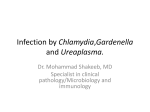
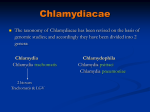
MAJOR ARTICLE Identificatio of CT521 as a Frequent Target of Th1 Cells in Patients with Urogenital Chlamydia trachomatis Infection Anja Weinreich Olsen,1 Frank Follmann,1 Klaus Jensen,1 Peter Højrup,4 Robert Leah,1,a Hanne Sørensen,3 Steen Hoffmann,4 Peter Andersen,1 and Michael Theisen1 1 Chlamydia Research, Department of Infectious Disease Immunology, and 2Department of Bacteriology, Mycology, and Parasitology, Statens Serum Institute, 3Department of Dermatovenerology, Bispebjerg Hospital, Copenhagen, and 4Department of Biochemistry and Molecular Biology, University of Southern Denmark, Odense, Denmark Background. The human immune response to a Chlamydia trachomatis serovar D lysate was investigated in patients with urogenital C. trachomatis infection, to identify novel T cell targets. Methods. A C. trachomatis lysate was fractionated on the basis of molecular mass, and each fraction was used to stimulate peripheral-blood mononuclear cells from patients with C. trachomatis infection. In frequently recognized fractions, proteins were identifie by mass spectrometry, recombinantly expressed, and tested for T cell recognition. Results. T cell recognition of the fractions was highly heterogeneous in patients with C. trachomatis infection (n p 16). Four patients exhibited responses that were strongly targeted to antigens of 16–20-kDa molecular mass. Three proteins were identifie in this fraction: CT043, CT511, and CT521. The T cell response to the individual recombinant proteins were investigated, and CT521 was found to induce the highest level of interferon (IFN)–g. The recognition of CT521 was investigated in a larger study population (n p 41 ), and a positive IFN-g response was measured in 83% of the patients. Several T cell epitopes were identifie in CT521; in particular, peptide 5 in the central part of the protein was frequently recognized by T cells (63%). Conclusion. We have identifie a novel C. trachomatis antigen, CT521, that is frequently recognized in patients with urogenital C. trachomatis infection. The intracellular bacterium Chlamydia trachomatis remains the most prevalent cause of sexually transmitted bacterial infections in humans, with an estimated 90 million new infections occurring globally every year [1]. In women, this infection can cause the onset of pelvic inflammato y disease and tubal factor infertility (TFI) [2, 3]. The infection is effectively cured by antibiotic therapy, but the high prevalence of asymptomatic cases makes a vaccine-based prevention strategy a very attractive goal. The search for potential vaccine candidates has high- Received 7 March 2006; accepted 27 June 2006; electronically published 22 September 2006. Potential conflicts of interest: none reported. a Present affiliation: UNIZYME Laboratories, Hørsholm, Denmark. Reprints or correspondence: Dr. Anja Weinreich Olsen, Chlamydia Research, Dept. of Infectious Disease Immunology, Statens Serum Institute, Artillerivej 5, DK-2300 Copenhagen S, Denmark ([email protected]). The Journal of Infectious Diseases 2006; 194:1258–66 2006 by the Infectious Diseases Society of America. All rights reserved. 0022-1899/2006/19409-0011$15.00 1258 • JID 2006:194 (1 November) • Olsen et al. lighted the relative lack of knowledge about the interactions between C. trachomatis and its human host [4]. Thus, it is still not clear what constitutes a protective immune response in humans, and little is known about the recruitment of specifi lymphocyte subsets and the roles played by cytokines after genital C. trachomatis infections in humans [5, 6]. Immunoepidemiological studies, therefore, are an important tool for definin the immune response to C. trachomatis infection and the resultant immunopathology. In this regard, increased interferon (IFN)–g production has been associated with immunity against Chlamydia infection [7, 8], whereas recurrent genital C. trachomatis infection and severe pathology leading to TFI have been associated with increased levels of interleukin (IL)–10 [9, 10]. In a recent study, production of IFN-g by peripheral-blood mononuclear cells (PBMCs) stimulated with C. trachomatis heat shock protein 60 (hsp60) was the strongest predictor of protection against reinfection among female sex workers in Kenya [9]. Figure 1. Protein fractions of Chlamydia trachomatis serovar D. A C. trachomatis lysate was separated into narrow molecular-mass fractions by the multielution technique. The fractions were analyzed by SDS-PAGE and silver staining. The migration of molecular-weight markers is shown at the far left, in kilodaltons (lane 1). The whole unfractionated lysate is shown before and after the fractions. The potential importance of IFN-g as an immune correlate of protection is also supported by numerous studies in murine models that have demonstrated that CD4+ Th1 cells, which produce IFN-g, play an important role in the ability of the murine immune system to control bacterial multiplication [11– 16] and by the observation that IFN-g can inhibit the growth of human Chlamydia strains in vitro [17–19]. Despite the importance of T cell responses for protection against infection with C. trachomatis, to date, few Chlamydia antigens have been identifie as targets for human T cells. The best characterized are the major outer membrane protein (MOMP) [20–23], hsp60 [24, 25], the histone-like protein Hc1 [25], the 60-kDa cysteine-rich outer membrane 2 (OMP2) [26, 27], YopD homologue, enolase, and polymorphic membrane protein D [28]. The identificatio and characterization of novel targets for human T cell responses to C. trachomatis is a priority, because this could facilitate the design of an optimal vaccine for Chlamydia infections. Here, we describe a stepwise antigen-discovery program based on an initial screening of T cell recognition of narrow molecular mass fractions from C. trachomatis serovar D. This led to the identificatio of a frequently recognized novel C. trachomatis antigen, CT521. PATIENTS, MATERIALS, AND METHODS Patients and samples. A total of 96 individuals (47 women and 49 men; mean age, 27 years) attending an outpatient sexually transmitted disease clinic at Bispebjerg Hospital who had tested positive for C. trachomatis by a specifi polymerase chain reaction assay were included after informed consent was obtained. Of these, 57 patients (23 women and 34 men; mean age, 27) who responded positively to a whole C. trachomatis lysate were selected for further investigation. PBMCs from 16 of these patients were stimulated with the protein fractions, to identify frequently recognized fractions. Results from 4 of the patients are shown here. To investigate the recognition of CT521 in a larger study population, PBMCs from 41 patients (15 women and 26 men; mean age, 26 years) were analyzed. Twenty-four blood donors with no history of positive C. trachomatis testing were enrolled as control subjects (16 women and 8 men; mean age, 31 years). For 2 of the CT521 high responders, follow-up samples were taken 2 times over a period of 10 months. The present study was approved by the local ethics committee for Copenhagen (01-008/03). Cultivation and harvestation of C. trachomatis serovar D. C. trachomatis serovar D (strain UW-3/Cx) was propagated in HeLa 229 cells (American Type Culture Collection). The cells were cultivated in RPMI 1640 passage medium (Gibco BRL) containing 5% heat-inactivated fetal calf serum (Gibco BRL), 1% (vol/vol) HEPES, 1% (vol/vol) l-glutamine, 1% (vol/vol) pyrovate, and 10 mg/mL gentamicine. For infection, semiconfluen monolayers of HeLa 229 cells in 175-cm2 flask were pretreated for 15 min at room temperature with diethylaminoethyl-dextran (Sigma-Aldrich; 45 mg/mL in Hanks’ balanced salt solution) and inoculated with 1 inclusion forming unit per cell of C. trachomatis serovar D. After 2 h of incubation at 35C, RPMI 1640 passage medium supplemented with 5% glucose and 1 mg/mL cycloheximide was added. After an additional 72 h of incubation, bacteria were harvested by repeated centrifugation (30,000 g for 30 min at 4 C, 2 times) and sonication (12 s at 50 W, 2 times) steps. Finally, the bacterial suspension was layered on a 30% renografi solution and was centrifuged at 40,000 g for 30 min. After centrifugation, the pellet was resuspended in 250 mmol/L sucrose, 10 mmol/L NaH2PO4, 5 mmol/L l-glutamic acid (SPG buffer) and was stored at ⫺70C until use. Preparation and fractionation of C. trachomatis serovar D lysate. C. trachomatis serovar D in SPG buffer was centrifuged at 30,000 g for 30 min, and the pellet was resuspended 1:1 in sterile water and laemmli-reducing sample buffer and then boiled for 5 min. After repeated sonication (12 s at 50 W, 2 times), the suspension was centrifuged at 30,000 g for 30 min. The supernatant (C. trachomatis lysate) was stored at ⫺70C until use. The C. trachomatis lysate was fractionated as described by Andersen and Heron [29]. Briefl , C. trachomatis lysate in a quantity of 6–8 mg of protein was separated by 10%–20% SDS-PAGE (11-cm-wide center well; 0.75-mm-thick gel; 20 cm long). Gels preequilibrated in an ammonia/3-(cyclohexylamino)-1-propanesulfonic acid (CAPS) elution buffer (37 mmol/ L ammonia and 20 mmol/L CAPS buffer [pH 10.2]) were transferred to a Multi-Eluter (Bio-Rad) and electroeluted for 20 min. The protein fractions were aspirated, separated by 10%–20% SDS-PAGE, and analyzed by silver staining [30]. The protein T Cell Recognition of Chlamydia CT521 • JID 2006:194 (1 November) • 1259 Figure 2. T cell recognition of Chlamydia trachomatis serovar D protein fractions. Peripheral-blood mononuclear cells isolated from 4 patients with C. trachomatis infection (A) and from 4 control subjects (B) were stimulated with the individual fractions (2 mg/mL). The release of interferon (IFN)– g was measured in the supernatants after 5 days. Each point represents the mean SE of triplicate values. Asterisks indicate a highly recognized fraction. concentration in each fraction was determined by the Micro BCA method (Pierce). Fractions (0.5 mL) were stabilized by use of human AB serum (0.5%) and were kept frozen at ⫺70C until use. Samples were also frozen directly at ⫺70C without serum for use in mass-spectrometry (MS) analysis. MS analysis. Five bands were cut out of a silver-stained SDS-PAGE gel. The bands were washed, dried, reduced, and alkylated with iodoacetamide before overnight digestion at 37C with modifie trypsin (Promega), essentially as described elsewhere [31]. The resultant peptides were micropurifie with Poros R250 (Applied Biosystems) as column material and were eluted directly onto the matrix-assisted laser desorption ioni- zation (MALDI) target plate by use of a-cyano-4-hydroxycinnamic acid (10 mg/mL) in 70% acetonitrile and 0.1% trifluo roacetic acid. Mass spectra were acquired on a PerSeptive Voyager Elite MALDI MS instrument (PerSeptive Biosystems), with delayed extraction. Some peptides were analyzed by tandem MS analysis on a PerSeptive 4700 MALDI MS instrument. Proteins were identifie using the Mascot search engine (Matrix Science). Expression of C. trachomatis genes and purificatio of recombinant proteins. The full-length genes encoding CT043, CT511, and CT521 were amplifie from C. trachomatis serovar D [32] and expressed via the pDEST 17 expression vector (In- Table 1. Proteins identified in fraction 7 by mass spectrometry. Protein Average mass Theoretical pI Name CT521 CT043 15802.6 18384.1 11.9 4.8 L16 ribosomal protein Hypothetical protein P28535 O84047 CT511 16086.5 10.9 L15 ribosomal protein P28534 Accession no. NOTE. The average mass and theoretical isoelectric point (pI) were calculated by the ProtParam program (available at: http://www.expasy.org). The accession number is for the SwissProt database. 1260 • JID 2006:194 (1 November) • Olsen et al. Figure 3. T cell responses to recombinant (r) CT521, rCT511, and rCT043 in 4 patients with Chlamydia trachomatis infection (A) and in 4 control subjects (B). Peripheral-blood mononuclear cells were stimulated with 5, 1.25, and 0.31 mg/mL protein. The release of interferon (IFN)–g was measured in the supernatants after 5 days. Each point represents the mean SE of triplicate values. vitrogen). The corresponding recombinant proteins were initially purifie by metal chelate affinit chromatography, essentially as described elsewhere [33, 34], followed by size fractionation by SDS-PAGE and electroelution from SDS-PAGE gel pieces; precipitated with 80%–95% acetone (Aldrich HPLC grade), to remove SDS; washed in 95% ethanol; resuspended in 50 mmol/L Tris [pH 7.5], 150 mmol/L NaCl, and 40% glycerol; and stored at ⫺20C. Overlapping synthetic peptides. Ten synthetic 22–23mer peptides (9–12-aa overlap; see the figu e 5 legend) covering the complete primary sequence of CT521 were synthesized by standard solid-phase methods at Schafer-N (Copenhagen, Denmark). The peptides were lyophilized and stored dry until reconstitution in PBS. Lymphocyte preparation and cell culture. PBMCs were separated from whole blood by density gradient centrifugation (Lymphoprep; Nycomed) and frozen in liquid nitrogen until use. For use in assays, PBMCs were thawed and resuspended in RPMI 1640, supplemented with 1% penicillin/streptomycin, 1% nonessential amino acids, 1% glutamine, 1% pyrovat, 1% HEPES, and 10% human AB serum (local blood bank, Rigshospitalet, Copenhagen). The viability and number of cells were determined by nigrosin staining. The cells were cultured in triplicate in round-bottom microtiter plates (Nunc) at 1.25 ⫻ 105 cells/well in a total volume of 100 mL. Antigens were added at the following concentrations: 2 mg/mL, for the serovar D fractions; 5, 1.25, and 0.31 mg/mL, for recombinant (r) CT521, rCT511, and rCT043, respectively; and 10 mg/mL, for the overlapping CT521 peptides. Phytohemagglutinin (2 mg/ mL) was used as a positive control, and cell cultures without antigen were included as negative controls. The cells were incubated at 37C in humidifie air (5% CO2 and 95% air). The supernatants were harvested after 18 h for quantificatio of IL4 and after 5 days for quantificatio of IFN-g. Cytokine assays. The quantity of cytokines in supernatants was determined by standard sandwich ELISA. The level of IFNg was determined by use of commercially available monoclonal antibodies (Endogen), in accordance with the manufacturer’s T Cell Recognition of Chlamydia CT521 • JID 2006:194 (1 November) • 1261 Figure 4. Recognition of recombinant (r) CT521 in 41 patients with Chlamydia trachomatis infection and in 24 control subjects. Peripheralblood mononuclear cells were stimulated with 5 mg/mL rCT521, and the level of interferon (IFN)–g was measured in the supernatants 5 days later. The dashed horizontal line depicts the selected cutoff level for a positive response (509 pg/mL, which is the upper 95% confidence interval of the geometric mean for the control subjects). instructions. Recombinant IFN-g was used as a standard (Endogen). The limit of detection of the assay was 20 pg/mL, and IFN-g release into unstimulated wells was below the level of detection. The level of IL-4 was detected in the supernatants by use of a commercially available human IL-4 set (BD OptEIA Set Human IL-4; BD Bioscience), in accordance with the manufacturer’s instructions. Cytokine levels are given in picograms per milliliter of supernatant. The cutoff levels for positive protein and peptide responses were set at the upper limit of the 95% confidenc interval (CI) of the geometric mean for the control subjects. ELISAs. ELISAs were performed essentially as described elsewhere [35]. Microtiter plates were coated with rCT521 (0.5 mg/mL), and serum samples were tested at a 1:200 dilution. Antibody binding was detected by use of peroxidase-conjugated rabbit anti–human immunoglobulin (Dako). The cutoff level was adjusted to a specificit of 95%, based on 24 negative control samples. Statistical methods. The Mann-Whitney rank sum test was used for analyzing differences between groups. P ! .05 was considered to be statistically significant RESULTS Human T cell recognition of fractionated C. trachomatis antigens. To identify novel T cell targets during a C. trachomatis infection, we initiated a comprehensive analysis of the human T cell response to C. trachomatis. Patients with C. trachomatis infection from a local district hospital in Copenhagen 1262 • JID 2006:194 (1 November) • Olsen et al. who responded to a whole C. trachomatis lysate (59%) were enrolled in the study. The specificitie of T cell responses were analyzed by measuring the IFN-g response to 30 narrow protein fractions with a minimal overlap between neighboring fractions (figu e 1). PBMCs from a total of 16 patients were stimulated with the panel of protein fractions (data not shown). The immune responses showed a marked heterogeneity, and in each case the response was directed to multiple fractions. Four of the patients showed a characteristic profil with a preferential recognition of fraction (F) 7, which consisted of molecules of molecular masses between 16–20 kDa (figu e 2A). In all 4 patients, this fraction was 1 of the 2 most powerful inducers of IFN-g. In contrast, the fractionated proteins induced no or only a minimal response by lymphocytes from control subjects (figu e 2B). We therefore decided to focus on this fraction. To identify proteins that could be responsible for the T cell stimulatory activity of F7, proteins in this fraction were further separated by SDS-PAGE with a 22-cm-long gel. Under these conditions, ∼5 bands were detected in F7 by silver staining (data not shown). These 5 bands were excised from the silverstained gel, digested with trypsin, and subjected to peptide mass mapping by MALDI MS. The resultant peptide mass maps were matched against the National Center for Biotechnology Information nonredundant database for identification Three C. trachomatis proteins—CT521, CT511, and CT043, all with molecular masses in the expected size range—were identifie (table 1). CT521 and CT511 are similar to the ribosomal proteins L16 and L15, respectively, whereas the function of CT043 is unknown. T cell recognition of recombinant antigens. The full-length genes encoding CT043, CT511, and CT521 were each cloned into an expression plasmid producing in-frame fusion proteins with a stretch of 6 histidine residues. The products were firs purifie by metal chelate affinit chromatography, followed by elution from SDS-polyacrylamide gels. Different concentrations (5, 1.25, and 0.31 mg/mL) of the recombinant proteins were added to PBMCs isolated from the 4 patients with C. trachomatis infection who responded to F7 and from 4 control subjects. Cytokine (IFN-g and IL-4) release was measured by ELISA (figu e 3). Three of the 4 patients responded to rCT521 with an IFN-g level 12000 pg/mL at at least 1 of the antigen concentrations tested; in particular, 2 of the 4 patients responded strongly with high levels of IFN-g (15000 pg/mL). Overall, rCT043 and rCT511 both induced lower levels of IFN-g; however, in 1 patient (patient 2), rCT043 induced a higher level than did rCT521. IL-4 was not detected in any of the culture supernatants (data not shown). Taken together, these results suggest that CT521 is the antigen responsible for the majority of the observed T cell recognition of F7. CT521-specifi responses in patients with genital C. tra- chomatis infection. To further investigate the CT521-specifi human immune response elicited by a C. trachomatis urogenital infection, PBMCs collected from 41 patients and 24 control subjects were analyzed for their T cell responses to rCT521 (figu e 4). T cell responses specifi to rCT521 were significantl higher in the patients than in the control subjects (P ! .0001, Mann-Whitney rank sum test). PBMCs from 34 (83%) of the 41 patients responded to stimulation with rCT521 at levels above the cutoff (509 pg/mL, which is the upper 95% CI of the geometric mean for the control subjects), whereas PBMCs from only 6 (25%) of 24 control subjects showed a positive response at this cutoff level (figu e 4). Having demonstrated that CT521 is a T cell antigen, it was of interest to examine whether CT521 is also recognized by serum antibodies. Thus, rCT521 was evaluated by an IgG ELISA using serum samples from the same 41 patients and 24 control subjects tested for T cell recognition. None of the evaluated serum samples from the patients gave a positive signal above the cutoff level (data not shown), suggesting that CT521 is rarely recognized by serum IgG antibodies. Identificatio of T cell epitopes in CT521. To further characterize the molecule and analyze the fin specificit of the T cell responses to CT521, overlapping peptides covering the fulllength CT521 sequence were analyzed individually. The peptides were synthesized as 22–23mers with 9–12-aa overlap and were used to stimulate PBMCs from 34 CT521-positive patients and 18 CT521-negative control subjects (figu e 5A and 5B). With a cutoff level of 23 pg/mL IFN-g (the upper 95% CI of the geometric mean for the control subjects), all peptides were recognized by T cells from at least 2 patients, thereby demonstrating a wide array of T cell epitopes in this molecule (figu e 5A). However, although the responses were heterogeneous, a hierarchy existed, with certain regions being strong targets for the response. Peptide (P) 2 (aa 14–36) and the peptides in the central region (P4–P6, covering aa 40–88), especially, were more dominant than the others. In particular, the peptide present in the central part, aa 53–75 (P5), was frequently recognized by PBMCs from the patients (figu e 5A). P5 was recognized by 23 (68%) of the 34 patients, with a median IFN-g release of 335 pg/mL. In contrast, the IFN-g responses for the control subjects were all !100 pg/mL, and PBMCs from only a few control subjects (10%–20%) responded above the cutoff level (figu e 5B). Two of the patients who responded strongly to rCT521 and P5 were followed for 10 months, to further analyze recognition of CT521 and the individual peptides (figu e 6). The epitope recognition pattern did not change when the patients were studied at consecutive time points before and after treatment—at all 3 time points, P5 was the dominant epitope in both patients. The cellular response to P5 was further characterized by subset depletion in 1 of the patients. The response Figure 5. Recognition of CT521 peptides in patients with Chlamydia trachomatis infection. A, Interferon (IFN)–g release. Ten synthetic peptides (P1–P10) spanning the whole protein were tested by measuring IFN-g release after stimulation of peripheral-blood mononuclear cells from patients (n p 34) and control subjects (n p 18 ) (except for P10, which was tested in only 17 patients and 14 control subjects). The dashed horizontal line depicts the selected cutoff level for a positive response (23 pg/mL, which is the upper 95% confidence interval of the geometric mean for the control subjects). B, Recognition frequencies of single peptides in patients and control subjects. The peptides were constructed as follows: P1, aa 1-22; P2, aa 14–36; P3, aa 27–49; P4, aa 40–62; P5, aa 53–75; P6, aa 66–88; P7, aa 77–99; P8, aa 90–112; P9, aa 102–124; and P10, aa 116–138. T Cell Recognition of Chlamydia CT521 • JID 2006:194 (1 November) • 1263 Figure 6. Conserved epitope recognition pattern over time. Peripheral-blood mononuclear cells from 2 patients were stimulated with recombinant (r) CT521 and 10 CT521 synthetic peptides at different time points (0 indicates before treatment, and 1 and 10 indicate 1 and 10 months after treatment). to P5 was abrogated by depletion of the CD4+ cell population, whereas depletion of the CD8+ cell population had no effect (data not shown). DISCUSSION Studies aimed at the identificatio of chlamydia proteins relevant for human immunity to C. trachomatis infection are of high priority in the development of a vaccine against the disease. In the present study, we investigated the specificit of human T cell responses to C. trachomatis serovar D proteins by a method in which complex protein mixtures separated by SDS-PAGE are electroeluted into fractions, each of which contains a few protein bands in a physiological buffer [29]. This approach has several advantages over the T cell immunoblotting technique used in previous studies, in which the proteins bands are excised from the nitrocellulose membranes, converted into particles, and added to cell cultures [25, 27, 36]. First, the exact protein concentration can be determined in each molecularweight fraction, meaning that all fractions can be tested at the same protein concentration and that the T cell stimulatory activity of the different molecular-weight regions can be compared directly. Second, each protein fraction can be subjected to protein chemical analyses, such as protein identificatio by mass fingerprintin and MS sequencing of selected peptides. In the present study, we conducted a detailed analysis of one 1264 • JID 2006:194 (1 November) • Olsen et al. protein fraction, F7, and this led to the identificatio of CT521 as an antigen that is frequently recognized by patients with C. trachomatis infection. CT521 has not previously been reported as a target of the human immune response during urogenital C. trachomatis infection. Of the samples from the C. trachomatis patients enrolled in the present study, 83% displayed a T cell response to CT521, compared with 25% of the control samples. Ideally, the responses of patients should be compared with those of nonexposed negative control subjects. Unfortunately, it is difficul to fin suitable control samples, because many individuals may have experienced a subclinical Chlamydia infection or may have had an infection with Chlamydia pneumonia, which is known to induce cross-reactivity against at least some antigens [27]. This could explain the positive response to CT521 observed in at least some of the control samples. On the basis of sequence similarity, CT521 has been identifie as the ribosomal L16 protein, a structural component of the large ribosomal subunit [32], and CT521 has been detected in both phases of the chlamydial life cycle [37]. The observation that a ribosomal protein is frequently recognized during C. trachomatis infection is in agreement with the finding of previous studies, in which ribosomal proteins from a variety of microorganisms have been characterized as major antigens. Moreover, a number of ribosomal proteins have been dem- onstrated to induce at least partial protection in animal models of the respective diseases [38–40]. Because ribosomal proteins are expected to be predominantly located in the bacterial cytoplasm, CT521 may be accessible to antigen-presenting cells and, thus, presented to CD4+ T cells after it is released by infected epithelial cells. Alternatively, it might be speculated that CT521 could access the host cell cytosol (through the type III secretion system) and thereby act as an antigen for CD8+ T cells. Irrespective of how and when CT521 is presented to the human immune system during the chlamydial life cycle, bacterial proteins that are predominantly associated with the cytoplasm have been found to be immunodominant during the course of a natural C. trachomatis infection, as exemplifie by hsp60 [41]. CT521 appears to elicit a predominantly Th1 immune response that is characterized by high levels of IFN-g and undetectable levels of IL-4. However, in contrast to other known C. trachomatis T cell antigens, such as MOMP, OMP2, and hsp60 [42–45], CT521 appears to be targeted exclusively to the cell-mediated-immunity arm of the immune response. None of the patients with C. trachomatis infection in the present study had a detectable level of serum IgG antibodies against CT521. Epitope-mapping experiments revealed several distinct epitopes in CT521, with the P5 epitope (aa 53–75) being recognized by PBMCs from 68% (23/34) of the patients. Several CD4+ T cell epitopes have previously been mapped in C. trachomatis antigens, such as MOMP [22, 23], OMP2 [27], hsp60 [24], and Hc1 [25]. However, in contrast to the present study, in which we used polyclonal T cell populations, these previous studies used T cell clones from a few patients. To our knowledge, this is therefore the firs report of a single epitope being recognized by 63% of patients with C. trachomatis infection responding to a C. trachomatis lysate. Interestingly, the epitope recognition pattern remained constant in patients for up to 10 months after the primary samples had been tested, which contrasts with observations for certain viral diseases in which the epitope recognition pattern changes over time [46]. Although the possible role played by CT521-specifi T cell responses remains to be investigated, a reasonable precondition for even considering an antigen to confer protection is its frequent recognition by a heterogeneous human population, thereby demonstrating both in vivo expression and presentation by the human major histocompatibility complex. Administered in an optimized delivery system and devoid of other less relevant or even detrimental immune responses raised during natural infection, this component may, therefore, provide a potential starting point for a novel subunit vaccine. Furthermore, the CT521 protein is an attractive vaccine candidate because it is abundantly expressed during bacterial growth and is highly conserved between different Chlamydia serovariants. In conclusion, we have identifie a novel C. trachomatis an- tigen, CT521, that is frequently recognized in patients with urogenital C. trachomatis infection. Ongoing studies in animal models will determine the protective value of the protein. Acknowledgments We thank Vita Skov, Lisbeth Schack Abrahamsen, Annette Hansen, and Inger Christiansen, for excellent technical assistance. References 1. World Health Organization (WHO). Global prevalence and incidence of selected curable sexually transmitted infections: overview and estimates. Geneva, Switzerland: WHO, 2001. 2. Pearlman MD, Mcneeley SG. A review of the microbiology, immunology, and clinical implications of Chlamydia trachomatis infections. Obstet Gynecol Surv 1992; 47:448–61. 3. Peipert JF. Clinical practice: genital chlamydial infections. N Engl J Med 2003; 349:2424–30. 4. Brunham RC. Human immunity to Chlamydiae. In: Stephens RN, ed. Chlamydia intracellular biology, pathogenesis, and immunity. Washington, DC: American Society for Microbiology Press, 1999:211–38. 5. Kelly KA. Cellular immunity and Chlamydia genital infection: induction, recruitment, and effector mechanisms. Int Rev Immunol 2003; 22:3–41. 6. Reddy BS, Rastogi S, Das B, Salhan S, Verma S, Mittal A. Cytokine expression pattern in the genital tract of Chlamydia trachomatis positive infertile women—implication for T-cell responses. Clin Exp Immunol 2004; 137:552–8. 7. Arno JN, Ricker VA, Batteiger BE, Katz BP, Caine VA, Jones RB. Interferon-gamma in endocervical secretions of women infected with Chlamydia trachomatis. J Infect Dis 1990; 162:1385–9. 8. Wang C, Tang J, Crowley-Nowick PA, Wilson CM, Kaslow RA, Geisler WM. Interleukin (IL)-2 and IL-12 responses to Chlamydia trachomatis infection in adolescents. Clin Exp Immunol 2005; 142:548–54. 9. Cohen CR, Koochesfahani KM, Meier AS, et al. Immunoepidemiologic profil of Chlamydia trachomatis infection: importance of heat-shock protein 60 and interferon-g. J Infect Dis 2005; 192:591–9. 10. Wang C, Tang J, Geisler WM, Crowley-Nowick PA, Wilson CM, Kaslow RA. Human leukocyte antigen and cytokine gene variants as predictors of recurrent Chlamydia trachomatis infection in high-risk adolescents. J Infect Dis 2005; 191:1084–92. 11. Hawkins RA, Rank RG, Kelly KA. A Chlamydia trachomatis-specifi Th2 clone does not provide protection against a genital infection and displays reduced traffickin to the infected genital mucosa. Infect Immun 2002; 70:5132–9. 12. Igietseme JU, Ramsey KH, Magee DM, Williams DM, Kincy TJ, Rank RG. Resolution of murine chlamydial genital infection by the adoptive transfer of a biovar-specific Th1 lymphocyte clone. Reg Immunol 1993; 5:317–24. 13. Johansson M, Schon K, Ward M, Lycke N. Genital tract infection with Chlamydia trachomatis fails to induce protective immunity in gamma interferon receptor-deficien mice despite a strong local immunoglobulin A response. Infect Immun 1997; 65:1032–44. 14. Morrison RP, Caldwell HD. Immunity to murine chlamydial genital infection. Infect Immun 2002; 70:2741–51. 15. Morrison RP, Feilzer K, Tumas DB. Gene knockout mice establish a primary protective role for major histocompatibility complex class IIrestricted responses in Chlamydia trachomatis genital tract infection. Infect Immun 1995; 63:4661–8. 16. Perry LL, Feilzer K, Caldwell HD. Immunity to Chlamydia trachomatis is mediated by T helper 1 cells through IFN-gamma-dependent and -independent pathways. J Immunol 1997; 158:3344–52. 17. Beatty WL, Byrne GI, Morrison RP. Morphologic and antigenic char- T Cell Recognition of Chlamydia CT521 • JID 2006:194 (1 November) • 1265 18. 19. 20. 21. 22. 23. 24. 25. 26. 27. 28. 29. 30. 31. 32. acterization of interferon gamma-mediated persistent Chlamydia trachomatis infection in vitro. Proc Natl Acad Sci USA 1993; 90:3998– 4002. Morrison RP. Differential sensitivities of Chlamydia trachomatis strains to inhibitory effects of gamma interferon. Infect Immun 2000; 68: 6038–40. Perry LL, Su H, Feilzer K, et al. Differential sensitivity of distinct Chlamydia trachomatis isolates to IFN-gamma-mediated inhibition. J Immunol 1999; 162:3541–8. Kim SK, Angevine M, Demick K, et al. Induction of HLA class Irestricted CD8+ CTLs specifi for the major outer membrane protein of Chlamydia trachomatis in human genital tract infections. J Immunol 1999; 162:6855–66. Kim SK, Devine L, Angevine M, Demars R, Kavathas PB. Direct detection and magnetic isolation of Chlamydia trachomatis major outer membrane protein-specifi CD8+ CTLs with HLA class I tetramers. J Immunol 2000; 165:7285–92. Ortiz L, Angevine M, Kim SK, Watkins D, Demars R. T-cell epitopes in variable segments of Chlamydia trachomatis major outer membrane protein elicit serovar-specifi immune responses in infected humans. Infect Immun 2000; 68:1719–23. Ortiz L, Demick KP, Petersen JW, et al. Chlamydia trachomatis major outer membrane protein (MOMP) epitopes that activate HLA class IIrestricted T cells from infected humans. J Immunol 1996; 157:4554–67. Deane KH, Jecock RM, Pearce JH, Gaston JS. Identificatio and characterization of a DR4-restricted T cell epitope within chlamydia heat shock protein 60. Clin Exp Immunol 1997; 109:439–45. Gaston JS, Deane KH, Jecock RM, Pearce JH. Identificatio of 2 Chlamydia trachomatis antigens recognized by synovial flui T cells from patients with Chlamydia induced reactive arthritis. J Rheumatol 1996; 23:130–6. Gervassi AL, Grabstein KH, Probst P, Hess B, Alderson MR, Fling SP. Human CD8+ T cells recognize the 60-kDa cysteine-rich outer membrane protein from Chlamydia trachomatis. J Immunol 2004; 173: 6905–13. Goodall JC, Beacock-Sharp H, Deane KH, Gaston JS. Recognition of the 60 kilodalton cysteine-rich outer membrane protein OMP2 by CD4+ T cells from humans infected with Chlamydia trachomatis. Clin Exp Immunol 2001; 126:488–93. Goodall JC, Yeo G, Huang M, Raggiaschi R, Gaston JS. Identificatio of Chlamydia trachomatis antigens recognized by human CD4+ T lymphocytes by screening an expression library. Eur J Immunol 2001; 31: 1513–22. Andersen P, Heron I. Specificit of a protective memory immune response against Mycobacterium tuberculosis. Infect Immun 1993; 61: 844–51. Blum H, Beier H, Gross HJ. Improved silver staining of plant proteins, RNA and DNA in polyacrylamide gels. Electrophoresis 1987; 8:93–9. Shevchenko A, Wilm M, Vorm O, Mann M. Mass spectrometric sequencing of proteins silver-stained polyacrylamide gels. Anal Chem 1996; 68:850–8. Stephens RS, Kalman S, Lammel C, et al. Genome sequence of an ob- 1266 • JID 2006:194 (1 November) • Olsen et al. 33. 34. 35. 36. 37. 38. 39. 40. 41. 42. 43. 44. 45. 46. ligate intracellular pathogen of humans: Chlamydia trachomatis. Science 1998; 282:754–9. Franken KL, Hiemstra HS, Van Meijgaarden KE, et al. Purificatio of his-tagged proteins by immobilized chelate affinit chromatography: the benefit from the use of organic solvent. Protein Expr Purif 2000;18: 95–9. Theisen M, Vuust J, Gottschau A, Jepsen S, Hogh B. Antigenicity and immunogenicity of recombinant glutamate-rich protein of Plasmodium falciparum expressed in Escherichia coli. Clin Diagn Lab Immunol 1995; 2:30–4. Theisen M, Soe S, Jessing Sg, et al. Identificatio of a major B-cell epitope of the Plasmodium falciparum glutamate-rich protein (GLURP), targeted by human antibodies mediating parasite killing. Vaccine 2000; 19:204–12. Hassell AB, Reynolds DJ, Deacon M, Gaston JS, Pearce JH. Identifi cation of T-cell stimulatory antigens of Chlamydia trachomatis using synovial fluid-derive T-cell clones. Immunology 1993; 79:513–9. Skipp P, Robinson J, O’connor CD, Clarke IN. Shotgun proteomic analysis of Chlamydia trachomatis. Proteomics 2005; 5:1558–73. Baloglu S, Boyle SM, Vemulapalli R, Sriranganathan N, Schurig GG, Toth TE. Immune responses of mice to vaccinia virus recombinants expressing either Listeria monocytogenes partial listeriolysin or Brucella abortus ribosomal L7/L12 protein. Vet Microbiol 2005; 109:11–7. Iborra S, Soto M, Carrion J, et al. The Leishmania infantum acidic ribosomal protein P0 administered as a DNA vaccine confers protective immunity to Leishmania major infection in BALB/c mice. Infect Immun 2003; 71:6562–72. Jomaa M, Kyd JM, Cripps AW. Mucosal immunisation with novel Streptococcus pneumoniae protein antigens enhances bacterial clearance in an acute mouse lung infection model. FEMS Immunol Med Microbiol 2005; 44:59–67. Kinnunen A, Paavonen J, Surcel HM. Heat shock protein 60 specifi T-cell response in chlamydial infections. Scand J Immunol 2001; 54: 76–81. Clad A, Petersen EE, Dettlaff S. Antibodies to Chlamydia trachomatis heat shock protein 60 (cHSP60) and Chlamydia trachomatis major outer membrane protein (MOMP) in women with different tubal status. Clin Lab 2003; 49:269–71. Schuppe HC, Pichlmeier U, Schenk BI, Bottcher M. Antibodies to Chlamydia trachomatis heat shock protein (cHSP60) and major outer membrane protein (MOMP) in men with impaired fertility. Clin Lab 2003; 49:273–5. Sziller I, Witkin SS, Ziegert M, Csapo Z, Ujhazy A, Papp Z. Serological responses of patients with ectopic pregnancy to epitopes of the Chlamydia trachomatis 60 kDa heat shock protein. Hum Reprod 1998; 13: 1088–93. Wagar EA, Schachter J, Bavoil P, Stephens RS. Differential human serologic response to two 60,000 molecular weight Chlamydia trachomatis antigens. J Infect Dis 1990; 162:922–7. Van Der Most RG, Murali-Krishna K, Lanier JG, et al. Changing immunodominance patterns in antiviral CD8 T-cell responses after loss of epitope presentation or chronic antigenic stimulation. Virology 2003; 315:93–102.