Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Heart failure wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Mitral insufficiency wikipedia , lookup
Coronary artery disease wikipedia , lookup
Antihypertensive drug wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
Myocardial infarction wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Cardiac surgery wikipedia , lookup
Lutembacher's syndrome wikipedia , lookup
Atrial septal defect wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
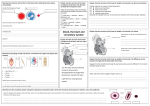
Module 5 Pediatric Cardiac Disorders Fetal Circulation Main Blood Flow Placenta Umbilical Vein Liver Ductus Venosus Inferior Vena Cava Vena Cava Right Atrium Foramen Ovale Left Atrium Left Ventricle Aorta Body Fetal Circulation Secondary Route: Right Atrium Right Ventricle Pulmonary Artery Ductus Arteriosus (so does not go to lungs) Aorta Body Fetal Circulation Third route of blood flow Right Atrium Right Ventricle Pulmonary Artery Lungs (needs to perfuse the lungs and upper body with oxygen) Left Atrium Left Ventricle Aorta Body Transition from Fetal Circulation to Pulmonary circulation The umbilical arteries and vein and the ductus venosus become non-functional Decreased pulmonary vascular resistance and increased pulmonary blood flow Increase in pressure of the left atrium, decrease pressure in right atrium, causing closure of foramen ovale. Pulmonary resistance is less than systematic resistance so there is left-to-right shunting resulting in closure of the ductus arteriosus. Congestive Heart Failure Congestive heart failure The inability of the myocardium to circulate enough oxygenated blood to meet the demands of the body. When the heart fails, cardiac output is diminished. Heart rate, preload, contractitility, and afterload are affected. Peripheral tissue is not adequately perfused. Congestion in lungs and periphery develops. Etiology and Pathophysiology Congenital defects – allow blood to flow from the left side of the heart to the right so that extra blood is pumped to the pulmonary system rather than through the aorta when the ventricle contracts. Obstructive congenital defects – restricts the flow of blood so the heart hypertrophies to work harder to force blood through the narrowed structures. The hypertrophied muscle becomes ineffective. Other defects which weaken the heart muscle. Compensatory Mechanisms Stimulation of the sympathetic nervous system which releases norepinephrine from the adrenals. This stimulates blood vessels to constrict and an increase in the heart rate. Tachycardia increases venous return to the heart which stretches the myocardial fibers and increases preload. Only successful for short period of time. Increased renin and ADH secretion caused by decrease renal perfusion. Resultant increase in Na and H2O retention to increase fluid to the heart and leading to edema Signs and Symptoms 1. 2. 3. 4. 5. 6. 7. Tires easily during feeding Periorbital edema, weight gain Rales and rhonchi Dyspnea, orthopnea, tachypnea Diaphoretic / sweating Tachycardia Failure to gain weight Treatment of Congestive Heart Failure Medication Therapy Digitalis – increases contractility and decreases heart rate. ACE-inhibitors - arterial vasodilator / afterload reducing agent Diuretics - enhance renal secretion of sodium and water by reducing circulating blood volume and decreasing preload. Beta Blocker - increases contractility Treatment of Congestive Heart Failure Diet – low sodium, small frequent feedings (be sure you can pick the right foods for a low NA diet. Nursing care: Measure intake and output – weighing diapers Observe for changes in peripheral edema and circulation If ascites present – take serial abdominal measurements to monitor changes. Skin care Turning schedule Congenital Cardiac Anomalies Defects that increase pulmonary blood flow Patent Ductus Arterious Atrial septal defects Ventricle septal defects Atrial Septal Defect 1. Oxygenated blood is shunted from left to right side of the heart via defect 2. A larger volume of blood than normal must be handled by the right side of the heart hypertrophy 3. Extra blood then passes through the pulmonary artery into the lungs, causing higher pressure than normal in the blood vessels in the lungs congestive heart failure Treatment Medical Management Cardiac Catheterizaton Medications – digoxin Amplatzer septal occluder Open-heart Surgery Cardiac Catheterization Pre-care: History and Physical Lab work – EKG, ECHO cardiogram, CBC NPO Preprocedural teaching Post Care: Monitor vital signs Monitor extremity distal to the catheter instertion, Keep leg immobilized Vital signs Check for bleeding at insertion site Measure I&O Treatment Device Closure – Amplatzer septal occluder During cardiac catheterization the occluder is placed in the Defect Ventricle Septal Defect 1. Oxygenated blood is shunted from left to right side of the heart via defect 2. A larger volume of blood than normal must be handled by the right side of the heart hypertrophy 3. Extra blood then passes through the pulmonary artery into the lungs, causing higher pressure than normal in the blood vessels in the lungs congestive heart failure Treatment Surgical repair with a patch inserted Patent Ductus Arteriosus 1. Blood shunts from aorta (left) to the pulmonary artery (right) 2. Returns to the lungs causing increase pressure in the lung 3. Congestive heart failure Treatment for PDA Medical Mangement Medication Indomethacin - inhibits prostaglandin's which help keep the ductus arteriosus open Surgery Ligate the ductus arteriosus Treatment for PDA Cardiac Catheterization Insert coil – tiny fibers occlude the ductus arteriosus when a thrombus forms in the mass of fabric and wire Defects with decrease blood flow and mixed defects Pulmonic stenosis Tetralogy of fallot Transposition of the great arteries Truncus arteriosus Pulmonic Stenosis Narrowing of entrance that decreases blood flow Treatment: Medications – Prostaglandins to keep the PDA open Cardiac Catheterization Baloon Valvuloplasty Surgery Valvotomy Tetralogy of Fallot Four defects are: 1. 2. 3. 4. Signs and Symptoms 1. Failure to thrive 2. Squatting 3. Lack of energy 4. Infections 5. Polycythemia 6. Clubbing of fingers 7. Cerebral absess 8. Cardiomegaly Treatment Surgical interventions Blalock – Taussig or Potts procedure – increases blood flow to the lungs. Open heart surgery Transposition of Great Vessels Aorta arises from the right ventricle, and the pulmonary artery arises from the left ventricle - which is not compatible with survival unless there is a large defect present in ventricular or atrial septum. artery aorta Truncus arteriosus A single arterial trunk arises from both ventricles that supplies the systemic, pulmonary, and coronary circulations. A vsd and a single, defective, valve also exist. Entire systemic circulation supplied from common trunk. Defects obstructing Systemic blood flow • • Aortic stenosis Coarctation of the Aorta Coarctation of the Aorta 1. Narrowing of Aorta causing obstruction of left ventricular blood flow 2. Left ventricular hypertrophy Signs and Symptoms 1. B/P in upper extremities 2. B/P in lower extremities 3. Radial pulses full/bounding and femoral or popliteal pulses weak or absent 4. Leg pains, fatigue 5. Nose bleeds Treatment Goals of management are to improve ventricular function and restore blood flow to the lower body. Medical management with Medication A continuous intravenous medication, prostaglandin (PGE-1), is used to open the ductus arteriosus (and maintain it in an open state) allowing blood flow to areas beyond the coarctation. Baloon Valvoplasty Surgery for Coarctation of Aorta 1. Resect narrow area 2. Anastomosis Ask Yourself ? Laboratory analysis on a child with Tetralogy of Fallot indicates a high RBC count. The polycythemia is a compensatory mechanism for: a. Tissue oxygen need b. Low iron level C. Low blood pressure d. Cardiomegaly Acquired Cardiac Diseases RHEUMATIC FEVER A systemic inflammatory (collagen) disease of connective tissue that usually follows a group A beta-hemolytic streptococcus infection. This disorder causes changes in the entire heart (especially the valves), joints, brain, and skin tissues. Rheumatic Fever Assessment Jones Criteria Major Minor Treatment Antibiotic Therapy Aspirin Subacute Bacterial Endocarditis / Ineffective Endocarditis: Microorganisms grow on the endocardium, forming vegetations, deposits of fibrin, and platelet thrombi. The lesion may invade adjacent tissues such as aortic and mitral valves. Subacute Bacterial Endocarditis / Ineffective Endocarditis: Assessment Diagnosis – blood cultures Treatment Antibiotics Patient teaching – take antibiotics prior to surgery, dental work, etc. Kawasaki Disease Multisystem vasculitis – inflammation of blood vessels in the body especially the coronary arteries with antigen-antibody complexes. Kawasaki Disease Signs and Symptoms / Treatment Three Phases of clinical manifestations: Acute Subacute Convalesant Treatment Aspirin Gamma Globulin Nursing Care Kawasaki Disease Which phase of Kawasaki is this child exhibiting? Inflamed, Cracked, Peeling Lips Strawberry tongue