Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
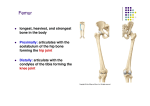
Plates 486-491 in Netter’s -Lower limb specialized for weight bearing, maintaining equilibrium, locomotion -Divided into four parts: -Pelvic girdle (hip) -Thigh region - femur + patella -Leg - tibia + fibula -Foot - tarsals, metatarsals, phalanges PELVIS -Composite hip bone spans the sacrum and the femur -Each hip bone consists of three individual bones that are fused in adulthood - ilium, ischium, pubis -Separated by cartilage usually until puberty ossification into one bone -In adults, acetabulum is only place where the remnants of three bones can be seen -Ilium - largest, forms superior part of hip -Ischium - posterior/inferior part of hip -Pubis - anterior part of hip bone, acetabulum, anterior medial hip (Find posterior, inferior, anterior spine, greater and lesser sciatic notch, etc) FEMUR -At superior end has head, neck, greater and lesser trochanter -Head in acetabulum -Head and neck of femur are an angle of bt 115 and 140 degrees w/shaft -When angle is reduced Coxa Vara -Weight of body passes through pelvic girdle onto femur, puts extreme stress on femur - easy to fracture -When angle is increased Coxa Valga -Mobility is compromised - femur is too close to midline -Normal angle allows for the greatest mobility while placing least amt of stress @ point where neck meets the shaft -Body (shaft) of femur - curved with anterior convexity -Distal end of the femur ends in two large condyles: TIBIA and FIBULA -Tibia is larger of the two - weight bearing bone - articulates w/condyles of femur superiorly, talus inferiorly -Nutrient foramen - largest foramen on any bone in the body - posterior surface of the tibia, upper 1/3rd -Fibula lies posteriolateral to tibia - mainly for muscle attachment -Shaft to two bones connected by interosseous membrane (like radius and ulna) -Distal end of tibia on medial side ends in the medial malleolus -Distal end of fibula on lateral side ends in the lateral malleolus TARSALS -7 tarsal bones: talus (articulates with tibia), calcaneus, cuboid, navicular, 3 cuneiforms -Talus: only bone that articulates with the tibia above -Body, head, neck moving distally -Sits on the anterior 2/3rd of the calcareous -Articulates on lateral side w/fibula -Articulates moving forward (anteriorly) with the navicular -Calcaneus: largest and strongest bone in the foot -Has on its superior medial border a shelf-like structure - sustentaculum tali - supports talus -Lateral surface of calcaneus has oblique ridge - fibular (paroneal) trochlea -Posterior surface has large prominence - tuberosity of calcaneus -Has medial, lateral, anterior tubercle - ONLY the medial tubercle rests on the ground when standing -Navicular: bt talus and cuneiforms -Cuboid: Most lateral bone in distal row -Cuneiforms x3: all three articulate with the navicular posteriorally and metatarsals anteriorly -Lateral, intermediate, mediate METATARSALS -Number 1 to 5 medial to lateral (metacarpals are 1-5 lateral to medial) -Each metatarsal has base proximally articulating with the navicular, body, head distally -Head of each metatarsal articulates with a proximal phalange of the toes -Plantar surface of first metatarsal - two sesamoid bones -14 phalanges: two metatarsals in great toe (hallux), three in every other toe Surface Anatomy -Iliac crest -Posteriorally @ level of L4 and L5 -High point of crest ends anteriorly at the anterior-superior iliac spine -Important in locating pain(?) of appendicitis -Pubic tubercle - anterior about 2.5 cm on either side of median plane -Evaluating inguinal hernias -The condyles of femur, patella are easily palpated -Lateral and medial malleoli are easily palpated -Greater trochanter may be palpated in some individuals -In anatomical position - horizontal line through trochanter passes through heads of the femur, pubic tubercles -Strength of a muscle is directly related to its cross-sectional diameter(???) Fascia of the Lower Limb -Divided into superficial and deep layer -Superficial: lies just deep to the skin - contains fat, nerves, lymphatic vessels, lymph nodes, two important veins: great saphenous (longest vein in body), small saphenous vein -At the knee - superficial fascia loses its fat and blends with the deep fascia -Deep fascia: layer of dense connective tissue bt the superficial fascia and the muscles in the thigh region -Surrounds the leg like an elastic stocking around the muscles -Called the fascia lata in the thigh -Very strong laterally - runs from iliac tubercle to tibia -Called the iliotibial tract - receives the tendon from the tensa fascia lata and tendon from gluteus maximus muscle -Distally, iliotibial tract is attached to the lateral condyle of the tibia -Below the knee where two layers merge, called the crural fascia -Thigh muscles are separated into three groups (anterior, medial, posterior) by three fascial intramuscular septum -Arise from fascia lata - attach to the linea aspera of the femur -Lateral Septum is much stronger than the other two -Crural fascia is continuous with the fascia lata - attached to the tibia - thick proximally and anteriorly, weak distally EXCEPT at the inferior and superior extensor retinaculum (around the ankle) -Leg is divided into compartments by the crural fascia: -Anterior (extensor) compartment -Lateral (fibular, paroneal) compartment -Posterior (flexor) compartment - further divided into superficial and deep region -Movements around the ankle - dorsiflexion, plantar flexion NERVES -Branches of the lumbar sacral plexus -Veins - major: great & small saphenous veins -Veins from the dorsum (dorsum surface of the arch) converge medially to form great saphenous, laterally to form small sapnenous -*Great saphenous vein (longest vein in body) runs from the foot to the groin - enters femoral vein near the femoral triangle through the saphenous openings* -Small saphenous vein ends in the popliteal fossa popliteal vein -Most lymph vessels parallel the saphenous veins -End in superficial inguinal lymph nodes -Lymph vessels associated with small saphenous veins end in popliteal lymph nodes THIGH MUSCLES -Divided into anterior, medial, posterior compartments -Coxa vs. Coxal bone (pelvic girdle) -Anterior compartment muscles: -Iliopsoas - begins as two separate muscles (psoas and iliacus) -Arise in abdomen, distally attach to lesser trochanter -Span the hip joint anteriorly -Hip flexors -Tensa Fascia Lata - strap-like muscle between the fascia lata and anterior superior iliac spine -Runs down to lateral condyle of the tibia -Abducts at the hip, also plays small role in hip flexion -Sartorius - important as a landmark! -Longest muscle in the body -Most superficial muscle in the anterior compartment -Spans two joints (hip and knee) -Parallels much of the femoral artery -Starts at anterior superior iliac spine, runs across superficial surface of thigh to attach distally to superior medial surface of the tibia -Flexes at the hip, laterally rotates at hip, flexes at the knee -Functions as a hip abductor -Quadriceps Femoris - has four parts -All extensors of the leg at the knee joint -All have common insertion (distal attachment) on tibial tuberosity through quadriceps tendon - along the quadriceps tendon distally is the patellar ligament -Rectus Femoris - spans two joints- also has hip action -Runs from anterior inferior iliac spine (pelvic girdle) to the base of the patella to tibial tuberosity -Is also a hip flexor (only one that spans two joints) -Vastus Lateralis - Originates on the greater trochanter -Vastus Medialis - Originates on the intertrochanteric line (bt the greater and lesser trochanter) -Vastus Intermedius - Originates on body of the femur -Tendons of all three vasti merge distally on the tendon of the rectus femoris for form quadriceps tendon attaches to tibial tuberosity -Chondromalacia of the patella (Runner’s Knee) - Presents with soreness and achey feeling deep to the patella -Usually due to erosion of the underside of the patella - due to imbalance in the tension placed on the quadriceps tendon -When patella is fractured - dramatic decrease of efficiency of muscles attaching at knee joint -Patella acts like a fulcrum in a lever system -Without patella, quadriceps must exert 30% more force to perform same action