Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Fecal incontinence wikipedia , lookup
Fatty acid metabolism wikipedia , lookup
Cholangiocarcinoma wikipedia , lookup
Hepatic encephalopathy wikipedia , lookup
Liver transplantation wikipedia , lookup
Liver cancer wikipedia , lookup
Intestine transplantation wikipedia , lookup
Surgical management of fecal incontinence wikipedia , lookup
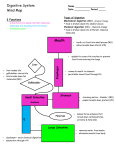
The Digestive System Chapter 25 Function of the Digestive System To break down food into a “usable” (absorbable) form To supply our cells with the nutrients they need for energy, growth & repair Organs of the Digestive System Gastrointestinal tract (GIT) – continuous passageway which contains the food from the time it enters the body, until it leaves; organs include: mouth (oral cavity), pharynx, esophagus, stomach, small intestine, large intestine, rectum, anus Accessory organs - participate in digestive processes; organs include: teeth, tongue, salivary glands, liver, gall bladder, pancreas Processes of Digestion 1. Ingestion 2. Movement along GIT Voluntary – e.g. swallowing Involuntary – e.g. peristalsis 3. Secretion – release of water, enzymes, acids, buffers, mucous, etc. into GIT for physical (mechanical) & chemical digestive processes Processes of Digestion 4. Digestion Mechanical processing – physical breakdown of food; e.g. mastication, emulsification, mixing waves, segmentation Chemical digestion – chemical breakdown of food; disassembling of organic molecules into their component parts; requires enzymes carbohydrates disaccharides monosaccharides proteins amino acids lipids fatty acids & monoglycerides Processes of Digestion 5. Absorption – movement of nutrients from GIT into blood capillaries (monosaccharides, amino acids, H2O, vitamins, minerals) or lymphatic capillaries (fatty acids) 6. Excretion (Defecation) – removal of waste products from GIT Histology of the GIT 4 layers of tissue surround the lumen of the GIT epithelium – stratified squamous or simple Mucosa columnar lamina propria – loose CT muscuaris mucosa – smooth muscle Submucosa CT with BV’s, nerves & lymphatics Muscularis externa Skeletal muscle at beginning & end of GIT, smooth muscle (inner circular; outer longitudinal layer) from lower esophagus to rectum Serosa (a.k.a. viseral peritoneum) Peritoneum & Mesenteries The abdominal cavity is lined with parietal peritoneum & many of the organs within are covered with visceral peritoneum Folds of peritoneum called “mesenteries” attach some organs to others greater omentum lesser omentum mesentery proper mesocolon Mouth (oral cavity) Regions include the vestibule & oral cavity proper Roof comprised of hard & soft palate; floor primarily comprised of tongue Mucosa of stratified squamous epithelium (non-keratinized) Joins to the oropharynx at the fauces Tongue – stratified sqamous epith. over skeletal muscle intrinsic & extrinsic muscles papillae filiform fungiform circumvallate taste buds Salivary glands – secrete saliva – made of H2O, salts & “salivary amylase” Parotid duct Parotid gland Sublingual gland Submandibular duct Submandibular gland Teeth – involved in “mastication” 2 sets of teeth – deciduous & permanent 4 types of teeth – incisors, cuspids (canines), bicuspids (premolars), molars Parts of a tooth – crown – dentin surrounded by enamel, has hollowed pulp cavity filled with CT pulp neck – at gingival border root – within mandible & maxilla, has hollowed root canal with BVs & nerves, root canal opens at apical foramen Pharynx Common passageway for air & food oropharynx & laryngopharynx lined with stratified squamous epithelium (nasopharynx lined with PSCC) uvula & epiglottis protect airway when swallowing (“deglutition”) nasopharynx uvula oropharynx epiglottis laryngopharynx Esophagus muscular tube running from pharynx, posterior to trachea, down thoracic cavity, through “esophageal hiatus” of diaphragm, to lower esophageal (a.k.a. cardiac) sphincter at junction of stomach functions in “deglutition” through action of peristalsis mucosa is stratified squamous epithelium variations in muscularis externa – begins as skeletal muscle at upper 1/3, mixed skeletal & smooth muscle in middle, smooth muscle by lower 1/3 Stomach - Gross Anatomy Lower esophageal (cardiac) sphincter Pyloric sphincter Stomach - Histology Rugae – folds of mucosa & submucosa to allow for expansion of stomach Mucosa of simple columnar epithelium with mucous cells Gastric pit leading to gastric glands Stomach – Histology (cont) - Secrete mucus to protect epithelial cells from enzymes & acid - Secrete HCl (for protein digestion) & intrinsic factor (for B12 absorption) - Secrete pepsinogen which (peptic cells) gets converted to “pepsin” when mixed with HCl; for protein digestion Entero(G-cells) - Secrete gastrin to regulate stomach emptying Stomach Modifications in stomach include 3 layers of smooth muscle in muscularis externa – outer longitudinal, middle circular, innermost oblique layer Functions of stomach include temporary storage of food mechanical breakdown of food to “chyme” through powerful mixing waves intrinsic factor for vitamin B12 absorption start of chemical digestion of proteins – pepsin proteins HCl polypeptides Small Intestine - Anatomy - connects stomach to large intestine; 15-20’ long; 1” diameter; held together in abdominal cavity by “mesentery proper” - site for completion of chemical digestion & absorption of nutrients - comprised of three regions: Duodenum – 10” in length; receives chyme from stomach, secretions from liver, gallbladder & pancreas Jejunum – 8’ long; most digestion & absorption occurs here Ileum – 12’ long; connects to cecum of large intestine at iliocecal valve (sphincter) Small Intestine Modifications in mucosa & submucosa of intestinal wall designed to increase functional surface area: Plicae circulares (circular folds) – large transverse ridges; most abundant in jejunum Villi – small finger-like projections of mucosal folds across surface of intestine Plicae circulares Small Intestine Villi Villi lined with “absorptive cells” - mucosal epithelium of simple columnar epithelium with microvilli “brush border” . These cells also produce enzymes (disaccharidases & peptidases) for final digestion of carbs and proteins Submucosa of each villus contains a capillary network & a “lacteal” (lymphatic capillary) for absorption of nutrients Small Intestine Intestinal crypts containing stem cells and intestinal glands Villi Between villi are intestinal crypts. Stem cells here can replace old cells found lining villi Intestinal glands within intestinal crypts secrete “intestinal juice” – provides watery medium to keep enzymes & digestive products in solution for help with absorption. Pancreas Stomach Tail Body Head Duodenum Pancreatic duct Retroperitoneal elongated organ lying posterior to stomach, from duodenum to spleen Both endocrine (pancreatic islets of Langerhans – secretes insulin & glucagon) & exocrine gland (pancreatic acini – secretes pancreatic juice (aka pancreatin) through pancreatic duct(s) to duodenum Pancreas Pancreatic juice – mixture of enzymes & buffers (sodium bicarbonate) secreted by acinar cells into pancreatic duct & released into duodenum pancreatic amylase Starch lipase Lipids maltose fatty acids + monoglycerol proteases (trypsin, chymotrypsin, carboxypeptidase) Proteins & polypeptides nucleases – digest RNA & DNA small peptides tri & dipeptides sodium bicarbonate – neutralizes acidic chyme because enzymes in small intestine need an alkaline pH Liver - Anatomy Largest organ within the body Comprised of 4 lobes: Large right & left lobes divided by falciform ligament; small caudate (by IVC) & quadrate (by gall bladder ) lobes falciform ligament continues at inferior margin as ligamentum teres (round ligament) (remnant of umbilical vein) Lobes of liver functionally divided into microscopic lobules Liver - Histology Lobules comprised of rows of Hepatocytes arranged radially around a central vein Hepatocytes surround blood sinusoids (capillary structures) which are partially lined with phagocytic Kupffer (aka stellate reticuloendothelial) cells hepatocytes central vein sinusoids Liver One function of hepatocytes is to produce bile, which gets secreted into bile canaliculi of lobule Bile canaliculi merge to form bile ducts, which are part of the portal triad seen at each corner of the lobules. Bile ducts merge to eventually create the right & left hepatic ducts Liver & gall bladder Right & left hepatic ducts unite to form common hepatic duct which merges with cystic duct of gall bladder to form common bile duct which joins with pancreatic duct & enters the Right hepatic duct Left hepatic duct duodenum Gall bladder – hollow muscular sac under right lobe of liver; stores & concentrates bile; releases bile through cystic duct Bile released into duodenum functions in emulsification of lipids, absorption of fats (due to presence of bile salts), & excretion of bilirubin Pancreatic & bile ducts Common bile duct Accessory pancreatic duct Stomach Tail Body Head Pancreatic duct Liver - Functions The liver has over 200 functions including (but not limited to): Bile production & excretion Metabolic regulation – storage of glycogen, fatty acids, fat-soluble vitamins & minerals interconversion of nutrients (“gluconeogenesis”) detoxification & removal of drugs, toxins & hormones hematological regulation – phagocytosis of worn-out RBCs, bacteria & other pathogens synthesis of plasma proteins Blood Supply to Liver In order for the liver to perform all of its functions, it receives blood through 2 vessels: Hepatic artery - delivers oxygenated blood into sinusoids of liver Hepatic Portal vein – delivers de-oxygenated, nutrient-rich blood from digestive organs to sinusoids of liver Liver uses O2 & nutrients within blood of sinusoids & then blood drains into central veins of lobule which merge to form the hepatic veins, which drain into the IVC Large Intestine Begins at the ilium & ends at the anus; 5’ long; 3” in diameter Transverse colon 3 regions: cecum - blind pouch; has appendix attached colon – ascending, (hepatic flexure), transverse, (splenic flexure), descending, sigmoid rectum – last 1” known as “anal canal” Hepatic (rt. Colic) flexure Splenic (lt. colic) flexure Ascending colon Descending colon ileum Ileocecal sphincter Rectum Anal canal Cecum Sigmoid colon Vermiform appendix Rectum Anal canal Internal anal sphincter Rectum External anal sphincter Anus Large Intestine main functions – H2O re-absorption; absorption of some vitamins & minerals; formation & temporary storage of fecal material no chemical (enzymatic) digestion but some bacterial Simple columnar epithelium in mucosa, except at anal canal (strat. Squam.) No plicae circularis or villi Modifications in muscularis externa & serosa : haustra taeniae coli longitudinal muscle layer forms bands called “taeniae coli” which create puckers known as “haustra” serosa forms “epiploic appendages” epiploic appendages THE END (literally!)