Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
NK1 receptor antagonist wikipedia , lookup
Pharmaceutical industry wikipedia , lookup
Cell encapsulation wikipedia , lookup
Discovery and development of neuraminidase inhibitors wikipedia , lookup
Prescription costs wikipedia , lookup
Discovery and development of angiotensin receptor blockers wikipedia , lookup
Pharmacognosy wikipedia , lookup
Hyaluronic acid wikipedia , lookup
Theralizumab wikipedia , lookup
Drug interaction wikipedia , lookup
Psychopharmacology wikipedia , lookup
Neuropharmacology wikipedia , lookup
Neuropsychopharmacology wikipedia , lookup
Discovery and development of proton pump inhibitors wikipedia , lookup
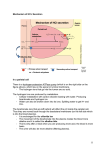
14-4-2014 Pharmacology-sheet 14 Rawan Al-Majali Gastrointestinal Pharmacology This lecture is about the pharmacological treatment of GI problems, including peptic ulcers, constipation, diarrhea, infections, and autoimmune diseases. Peptic ulcers: It is a defect in the continuity of the lining covering the stomach or intestines, and it has varying degrees depending on the depth of this defect, whether it’s only in the superficial layer or it’s coming down for two or more layers until it can cause sometimes bleeding or perforation. Causes: There are different causes or risk factors for the formation of peptic ulcer. The most common cause is infection by H. Pylori. Some peptic ulcers are linked to heavy usage of nonsteroidal anti-inflammatory drugs. NSAID (aspirin and ibuprofen) inhibit the cyclooxygenase pathway. Prostaglandins are produced from the cyclooxygenase pathway, and they are known for their effect of acid secretion inhibition. So when we use a drug that inhibits prostaglandin synthesis, we don’t have this inhibitory effect, and we have more acid secretion. That’s why these drugs -prostaglandin synthesis inhibitors- exaggerate peptic ulcer. And sometimes the problem may be caused by an endogenous disturbance other than exogenous factors (from within the stomach) like tumors, such as gastrinoma. This tumor secretes gastrin in an abnormal amounts, which stimulates acid secretion. Another cause is Zillonger Ellison syndrome where we have gastrin-secreting tumors, and increased acid secretion. Other causes are linked to: smoking, stress, spices, and alcohol consumption. Physiology of the stomach: To protect the organ from the corrosive effects of the acid, a layer of mucous coats the lining of our stomach, and as you know the stomach muscles are proteins, and we have the acids and the enzymes that digest proteins in the stomach so we need to protect the wall of the stomach from these inside molecules that can attack it. When the protective mucous layer breaks down, stomach acid can seep into the lining of your stomach and cause an ulcer. Page 1 of 8 14-4-2014 Pharmacology-sheet 14 Rawan Al-Majali Usually to treat peptic ulcer we use a combination of drugs, one or two of these drugs are usually antibiotics or anti-bacterial if the cause was due to an infection, and usually we give two drugs because bacteria can escape the effect of one drug, so if we give two drugs that work on two different mechanisms you still can kill the bacteria that have developed a mutation or resistance to the first drug. Physiology of acid secretion: There are four important cells in the mucosal layer; parietal cells, G-cells, Enterochromaffin cells (ECL), and chief cells. Acid is secreted from the parietal cells, G-cells secrete gastrin, ECL cells (enterochromaffin like cells) secrete histamine, and Chief cells secrete pepsin; an enzyme that digests the proteins. Regarding the structure or the architecture of the mucus layer, there are caniculi or folds that increase the surface area of the lining (irregular surfaces), and within these bigger folds we have smaller ones, at a microscopic level. Within these small indentations we find the parietal cells. We also have mucous secreting cells. Gastric secretions are under nervous and hormonal control, but how do parietal cells exactly secrete acid? For the parietal cell to secrete acid and transfer the hydrogen ions out of the cell, to the lumen, we need a pump; it is a proton pump, called H+/K+ ATPase pump. So basically a hydrogen ion is going to get pumped into the lumen of the stomach and in exchange for potassium, in other words; potassium comes in and hydrogen or proton goes out. In order for this pump to work we need ATP, that’s why it is called H+/K+ ATPase pump (active pump). You know that the secretory end product of parietal cells is HCl, and by far our pump has provided us with the first component which is H+, but what about the chlorine? When a proton goes out from the parietal cell and gets inside the lumen, alongside Cl diffuses passively to the lumen, and it will combine with H+ to form HCl. Once the parietal cell is exposed to a stimulus, there will be translocation of this pump into the caniculi for it to function and to connect between the two mediums; the lumen the the parietal cell. Usually we need to add phosphate groups to certain signaling mediators for this translocation to happen, so we need to activate certain phosphokinases. What run this whole process are three different pathways: -M3 receptor, this is a muscarenic receptor, so it is activated by acetylcholine or the vagal nerve. (Neural) Page 2 of 8 14-4-2014 Pharmacology-sheet 14 Rawan Al-Majali - H2 receptor, histamine 2 receptor. (hormonal: Paracrine) - G-receptor for gastrin or cholycystokinin, it is a peptide secreted from the GIT. (hormonal: Endocrine) Activation of any of these pathways causes an increase in acid secretion. And this is the basis of drug action that works for peptic ulcer. So if I use histamine antagonist, I prevent the secretion of acid, and if I use muscarinic antagonist I decrease the secretion of acid. The muscarinic receptors M3 are found on parietal cells, and ECL cells. So these get activated by acetylcholine binding, released from the vagus nerve, and it’s going to stimulate acid secretion. When M3 on parietal cells get activated, proton pump will be translocated to the membrane and the acid will be secreted. Activation of M3 on ECL cells triggers ECL to release histamine, and histamine binds to H2 receptor on parietal cells and stimulate acid secretion. If G-receptors on g-cells is activated, then gastrin is released, and it will bind to g-receptors on parietal cells and increase acid secretion. Another type of cells found in the stomach, are the D-cells, these secrete somatostatin. Somatostatin is a regulator of gastrin release; it inhibits gastrin release. The vagus nerve has an inhibitory action on these cells; inhibiting the inhibitory effect on gastrin, thus we have more gastrin secretion. Histamine release is controlled by two factors; vagal stimulation (acetylcholine binding to M3) and the G-receptors on ECL cells. So one important drug for peptic ulcer is H2 antagonist, or histamine antagonist, and this is a very common and old drug, and also we can use muscarinic antagonist but there are a lot of side effects associated with muscarinic antagonism. Gastrin receptor antagonist is not available clinically or commercially yet. Another way to decrease the peptic ulcer or the release of HCl is a direct inhibition of this pump. So we have drugs called PPI, they are the most sold drugs. We also have certain pumps, they are called active pumps, that actively secrete or diffuse chloride from inside the cell into the lumen, so we have two ways of chloride secretion, either passive diffusion, and if the concentration gradient is not enough we have these pumps that take chloride out. Vagal nerve stimulation affects: gastrin, histamine, and directly the proton pump. Page 3 of 8 14-4-2014 Pharmacology-sheet 14 Rawan Al-Majali Pharmacology: Generally, to treat peptic ulcer we aim for: 1. Reducing gastric acid secretion. 2. Neutralizing acid in the lumen. 3. Protecting the mucousa from acid destruction. 4. Prescribing antibiotics to eradicate H. Pylori. Reducing acid secretions: First group of drugs to talk about are the proton pump inhibitors: we have different names, all end with “zol”; omeprazol, lansoprazol, rabeprazol, and esomeprazol. There are different chemical modifications seen in these drugs, rendering them more active or having longer duration of action. Usually we use a drug with a long duration of action, so the patient doesn’t have to take it more than once. Esomeprazole is a very common drug in the market, its commercial name is “nexium” and it’s taken only twice a day, so it is very convenient for the patient. Proton pump inhibitors are the most widely used drugs throughout the world. If compared to the histamine antagonists, they are more expensive. (histamine antagonists cost around 3 JDS, while esomeprazol 20 or 30) Due to the fact that they’re taken orally, these drugs are usually present in a microcapsulation formulation; they are put in a small capsule within the pill, it protects them from acidity of the stomach, so it is easily absorbed into the parietal cells where we need it without losing its action. Inside the parietal cells, the drug undergoes protonation, so the drug enters from the blood into the parietal cells and then it gets protonated (highly charged) so it is difficult now to go out again, and consequently it stays where needed, and kept closer to its target of action (the proton pump). PPI causes irreversible inhibition and once it binds the pump, it does not get off the pump at all. And for parietal cells to get over the action of this drug, they need at least 3-4 days to be able to synthesize more pumps and resume acid secretion. Page 4 of 8 14-4-2014 Pharmacology-sheet 14 Rawan Al-Majali Full inhibition is happening with 2:1 ratio of the drug, that means 2 omeprazole molecules for example need to bind to one pump, for it to fully inhibit the pump. If we have one binding to one, we have somewhat of inhibition but we still have acid secretion, and this has to do more with the dose or concentration you give to the patient. Side effects: They have very minor side effects, can cause headache, diarrhea, nausea, and some people reported that PPI cause some dizziness but few people say it’s a psychological effect; in a medical trial, they gave some people placebo, and some people omeprazole, and they noticed that the ones who took omeprazole and said they have dizziness are similar to the number of people who took placebo and reported that they have dizziness, so it’s not a very serious or considerable side effect. One problem of taking the proton pump inhibitor is that it can inhibit certain proton pump inhibitors in the bone that are associated with osteoblastic activity, so long term use is going to decrease the bone formation and increase the susceptibility for fractures, because it can affect the balance or the building of the bone, and the calcium uptake. H2 receptor antagonists: Competitive inhibitors (bind to the receptor irreversibly, and affect the concentration of histamine around needed to induce its effect), they have a little bit more selectivity for H2 over H1. H1 receptors are more present in the bronchial muscles, so more related to asthma treatment. The first generation of anti-histamine and second generation do not differ in the selectivity to the receptor, both of them antagonize histamine-2 receptor. The difference is that the second generation can’t cross the blood brain barrier, so we don’t have sedation effect. They are present in different body fluids, because they’re well absorbed. The first prototype: Cimetidine, an old drug (in relation to finding a drug after knowing its target not by serendipity). Cimetidine has many side effects, so they developed newer drugs, but they all antagonize the H2 receptor. Ranitidine and nizatidine, are also used for Zollinger Ellison syndrome, and GERD (gastroesopheal reflux disease). Side effects: Cimetidine and a lot of its analogs (Ranitidine and Famotidine) inhibit cytochrome P450, so they interact with many drugs that are substrates for cytochrome P450. Page 5 of 8 14-4-2014 Pharmacology-sheet 14 Rawan Al-Majali Another important side effect is anti-androgen activity, so they decrease male characteristics in males. Also loss of libido and impotence; inability to perform sexual functions in the males. Increased plasma estradiol in males (increased female characteristics). Increased secretion of prolactin. That’s why we don’t use this drug that much nowadays. Neutralize acids in the lumen: Bases are used for that purpose, such as: aluminium anti-acids, magnesium anti-acids, calcium antiacids, and sodium anti-acids. Each of them has special side effect . Aluminium anti-acids cause chelation in many drugs and prevent their absorption, and can also cause diarrhea. Magnesium anti-acids have laxative action and these drugs are used to treat constipation because they cause diarrhea. Examples: magnesium hydroxide or hypochloride. Calcium anti-acids are the most commonly used, but they cause acid rebound; a reversed response after initial neutralization of the acid in the stomach; withdrawal causes the stomach to secrete even more acid as a reflex mechanism. And this is more prominent in calcium anti-acids, and also the sodium anti-acids. Sodium is important in different parts of the body, so when we take sodium anti-acids we aggravate certain diseases like congestive heart failure. Sodium anti-acids will diminish the effect of diuretics in hypertensive patients, and we’ll have a very short duration of action. Protect the mucosa from acid destruction: These drugs protect the mucosa from acid secretion, they form a surfactant layer. prostaglandins inhibit acid secretion, but they also increase mucous secretion, so they can be put under either groups (cytoprotective drugs -mucosal protection- or neutralizing drugs) this group includes: 1) bismuth compounds. 2) Sucralfate (Carafate). 3) Prostaglandins. Page 6 of 8 14-4-2014 Pharmacology-sheet 14 Rawan Al-Majali Bismuth compounds: -Pepto bismol (bismuth sulfate) has an anti-acid effect. It is bismuth subsalicylate or bismuth subcitrate. Pepto bismol is the commercial name. It mainly has a cyto-protective potential (increases cell protection) against the infection of H. Pylori, and they don’t know exactly how it works, but it can form a surfactant-like layer. Side effects: darkening of the stool and darkening of the tongue. -Sacralfate: it’s a complex molecule, contains sucrose and aluminum hydroxide, so this also forms a layer of highly charged negative ions that covers the lining of the stomach, and protects it from the acid secretion. So it’s also a cyto-protective drug. It adheres to the base of ulcer crater. Because it binds to the positively charged protein (since it’s negatively charged). And used for the maintenance therapy of ulcers when the patient gets better, because it’s not a very harsh drug. Does not work directly to inhibit acid secretion. Prostaglandins analogs: There are receptors for prostaglandins in parietal cells and they inhibit the acid secretion. Also, we have receptors in the mucous cells and they increase mucous secretion and promote mucous protection through stimulation of proliferation and repair of mucous cells. In parietal cells, prostaglandin inhibits an enzyme called adenocyclase to inhibit acid secretion. One example is the misoprostol, this is a prostaglandin analog. Side effects are diarrhea and abdominal cramping. It is contraindicated in pregnancy, especially in the late phases of pregnancy, because it can cause premature labor. It can be used to induce labor, but there are other drugs better for that, like oxytocin. It is approved for prevention of ulcers from NSAID. Nonsteroidal anti-inflammatory drugs inhibit the production of prostaglandin, so it is suitable to use prostaglandin analogs for ulcers caused by the use of non steroidal. Many of the patients are going to feel pain, a lot of this pain is not gonna be relieved by panadol or paracetmol, so you might think to prescribe something stronger for them which is ibuprofen, or voltrex, but all of these drugs increase the acid secretion by inhibiting prostaglandin, so they are contraindicated. They should take this drug in full stomach. Page 7 of 8 14-4-2014 Pharmacology-sheet 14 Rawan Al-Majali Antibiotics: Helicobacter produces large amounts of the enzyme urease, that breaks down urea, and the breakdown products (ammonia and carbon dioxide) are toxic to the epithelial cells, that’s why they are harmful to the lining of the stomach. It also produces cytotoxin A (VacA) and this also affects the phospholipid layer of the cells lining the stomach, and on top of that, the inflammatory response also stimulates the G-cells to produce gastrin, which also increases the acid secretion. The antibiotics that can be used: Clarithromycin, Amoxicillin, Metronidazole (anti-protozoal), and Tetracycline. Each of them is from a different group of antibiotics. Treatment protocols of ulcers: We have triple therapy or quadruple therapy, and the patient has two choices: 1. PPI+ clarithromycin + amoxicillin or metronidazole. 2. PPI or H2 Receptor antagonist + bismuth + metronidazole + tetracycline. In either choices the treatment includes two antibiotics. Muscarinic antagonist: Atropine and pirenzepine. Note: the doctor stopped here and you have to read the rest of the slides (constipation and diarrhea). Best wishes Page 8 of 8