Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
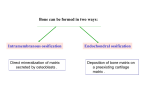
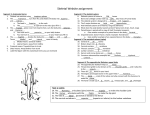
1 Skeletal System Paraxial mesoderm forms from segmented somitomeres in the occipital region. It also derives from somites which formed from somitomeres caudal to the occipital somitomeres. The skeletal system develops from paraxial and lateral plate (somatic) mesoderm and from neural crest. The somites differentiate into two parts: a sclerotome ventromedially and a dermomyotome dorsolaterally. The sclerotome differentiates into loose connective tissue called mesenchyme (embryonic connective tissue). Cells of mesenchyme migrate to become either fibroblasts, chondroblasts, or osteoblasts. Bone that forms the axial skeleton (vertebral column, ribs) develops from the mesenchyme of the sclerotome and the sternum, from mesoderm of the ventral body wall. The bones of the pelvic and shoulder girdle as well as the long bones of the limbs develop from lateral plate or somatic mesoderm. Some bone at the base of the cranial vault is formed from the occipital somites and somitomeres. In some bones, mesenchyme directly differentiates into bone: intramembranous ossification. This occurs, particularly, in flat bones of the skull. Alternatively, most bones in the body are formed when mesenchymal cells give rise hyaline cartilage models which later become ossified: endochondral ossification. Parts of bone at the base of the skull are also formed in this manner. Skull The skull is a composition structure consisting of two major subdivisions, the neurocranium, which surrounds the brain, and the viscerocranium, which surrounds the oral cavity, pharynx, and upper respiratory passages. Both have membranous and cartilagenous parts. Neurocranium Chondrocranium - The cartilagenous part of the neurocranium is the chondrocranium at the base of the skull. In the beginning, it is characterized by several sets of paired cartilages. One group (parachordals, hypophyseal cartilages, and trabeculae cranii) is closely related to midline structures. Caudal to the parachordal cartilages are four occipital sclerotomes. Along with the parachordal cartilages, the occipital sclerotomes (homologues of vertebral sclerotomes) fuse to form the base of the skull. The individual primitive components of the chondrocranium go through several patterns of growth and fusion to form complex bones of the base of the cranium: ethmoid, occipital, sphenoid, and temporal bones. The area about the foramen magnum for the occipital bone plus petrous and mastoid parts of the temporal bone is chondrocranium. Other parts of the occipital and temporal bones employ intramembranous ossification. Membranous neurocranium – Elements of the membranous neurocranium (paired parietal and frontal bones plus the interparietal part of the occipital bone) arise as flat plates of boney spicules from mesenchyme that has been induced by parts of the developing brain. These bones remain separate structures during fetal development and even at birth they are separated by connective tissue. Intersections between sutures where two or more bones meet are occupied by broader areas of connective tissue called fontanelles. Where the two frontal and parietal bones meet is the anterior fontanelle (bregma). Initially, the frontal bones are separated by a suture, the metopic suture, but they ususally fuse and the frontal bone is considered a single bone. At the junction of the parietal bones and occiput is the posterior fontanelle (lambda). 2 Viscerocranium Like the neurocranium, the viscerocranium consists of two divisions: a cartilagenous viscerocranium and a membranous viscerocranium. In contrast to the neurocranium, bones of the viscerocranium originate largely from neural crest-derived mesenchyme. Phylogenetically, the viscerocranium is related to the skeleton of the branchial arches (gill arches). Each branchial arch, or pharyngeal arch in the human, is supported by a cartilagenous rod which gives rise to a number of skeletal elements associated with that arch. The membranous viscerocranium related to the upper and lower jaws and region of the ear arise in association with the first arch. The first arch gives rise to maxillary process which forms the maxilla, zygomatic, and part of the temporal bone. The first arch also forms the mandibular process which contains Meckel's cartilage. Mesenchyme around Meckel's cartilage condenses and ossifies by membranous ossification giving rise to the mandible. Meckel's cartilage disappears except for the sphenomandibular ligament. Additional cartilagenous structures of the viscerocranium are derived from the dorsal tip of the mandibular process (incus and malleus) along with part of the second pharyngeal arch (stapes). Craniofacial defects Some malformations of the skull are secondary to disturbances in development of the brain. In this category are conditions such as acrania and anencephaly. Hydrocephaly can occur when there is brain malformation and concomitant obstruction of cerebrospinal fluid resulting in an enlarged skull. One family of cranial malformations is called craniosynostosis results from premature closure of certain sutures between major membrane bones of the neurocranium. Craniosynostosis is a feature of more than 100 genetic syndromes and is seen in 1/3000 live births. Premature closure of the sagittal suture produces a long, keel-shaped skull referred to as scaphocephaly. Oxycephaly, or turret skull, is the result of premature fusion of the coronal suture. Other terms for premature closer of the coronal suture are acrocephaly or tower skull. A dominant genetic condition, Crouzon's syndrome, has a gross appearance quite similar to that of oxycephaly with additional defects in the face, teeth, ears, and other body parts. Appendicular Skeleton The appendicular skeleton consists of the bones of the limbs and limb girdles. Late in the first month, upper limb promordia begin to bulge from the body wall before the lower. At this stage the limb bud consists of a mass of similar-looking mesodermal cells covered by a layer of ectoderm. The mesenchymal core is derived from the somatic layer of lateral plate mesoderm that will form bones and connective tissue. A unique feature of the limb bud is the presence of a ridge of thickened ectoderm (apical ectodermal ridge [AER]) located along the anteroposterior plane of the limb bud apex. During much of the time when the AER is present, the hand- and foot-forming regions of the developing limb are paddle-shaped with the apical ridge situated along the rim of the paddle. Experiments have shown that the AER interacts with the underlying limb bud mesoderm to promote outgrowth of the developing limb. The AER marks the border between the dorsal and ventral limb bud ectoderm. Different signaling molecules are either present or not present in the mesoderm with respect to mesoderm being ventral or dorsal to the AER. 3 Additionally, the AER acts as an organizing center for the proximodistal axis of the limb by stimulating the proliferation of the underlying mesoderm. Just beneath the AER is a severalhundred-micron-thick region of distal mesoderm called the progress zone. Cells in the progress zone divide actively and are not morphogenetically determined. However, as the limb bud grows out the mesodermal cells that are proximal enough to escape the influence of the AER become differentiated to their ultimate tissue type. That is, cells leaving the progress zone early ultimately form proximal skeletal elements (humerus and femur) and cells leaving later form elements of the forearm or hand in the upper limb. As limb development proceeds, changes become apparent in the AER. Instead of remaining continuous around the entire apex of the limb, the ridge begins to break up, leaving intact segments of thickened ridge epithelium covering the emerging digital rays (cartilagenous models for the digital bones). As the digital primordia continue to grow outward, apoptosis or programmed cell death sculpts the interdigital spaces. If interdigital cell death does not occur, a soft tissue web connects the digits on either side. Development of the upper and lower limbs is similar with the lower lagging by 1 – 2 days. During the seventh week, the limbs rotate in opposite directions. The upper rotate laterally 90o so that the extensor muscles lie on the lateral and posterior surface and thumbs are directed laterally. The lower limbs rotate medially 90o, placing the extensor muscle on the anterior surface and the big toes are directed medially. Limb skeleton – Formation of the skeleton can first be seen as condensation of mesenchymal cells in the central core of the proximal limb bud. Even before undergoing condensation, these cells are determined to form cartilage, and if they are transplanted to other sites or into culture, they still continue to differentiate into cartilage. Differentiation of the cartilagenous skeleton occurs in a proximodistal sequence. The term preaxial is defined as: situated in front of any transverse axis in the body of an animal; anterior; cephalic; esp., in front, or on the anterior, or cephalic (that is, radial or tibial) side of the axis of a limb. In mammals, the postaxial structures of the distal limb segments differentiate before the preaxial structures. The postaxial skeleton of the arm is considered to be the humerus, ulna, and digits 2-5. The preaxial portion of the limb bud becomes progressively reduced during limb outgrowth, contributing only to the radius and possibly the first digital ray. For the lower limb, the tibia and the bones of the great toe are preaxial, fibula and the bones of 3rd, 4th and 5th toes are postaxial (remember the lower extremities rotated medially). Certain limb defects, sometimes called hemimelias, are characterized by deficiencies of preaxial or post axial limb components. One of the characteristic features in differentiation of the limb skeleton is the formation of joints. Joint formation occurs by the transverse splitting of precartilagenous rods rather than by the apposition of two separate skeletal elements. Ossification of the bones of the extremities, endochondral ossification, begins by the end of the embryonic period. Primary ossification centers are present in all long bones of the limb by the 12th week of development. From the primary ossification center in the shaft or diaphysis, endochondral ossification gradually progresses toward the ends of the cartilagenous model. At birth the diaphysis of the bone is usually completely ossified, but the ends, epiphyses, are still cartilagenous. Later, secondary ossification centers appear in the epiphyses. Between the diaphysis and epiphysis is a cartilagenous epiphyseal plate which plays an important role in growth in the length of long bones. 4 Limb defects One of the best known abnormalities of the skeletal system is achondroplasia. This condition is caused by a disturbance of endochondral ossification in the epiphyseal plate of long bones, resulting in dwarfism. Congenital overproduction of growth hormone (GH) will cause gigantism. After the plates cease growing, acromegaly presents in overproduction of GH. Axial Skelton – Vertebral Column and Ribs During the fourth week of development, cells of the sclerotomes shift their position to surround both the spinal cord and the notochord. The conventional view of vertebral development tells us that the sclerotomes split into cranial and caudal halves. Basically, the densely packed caudal half of one sclerotome joins with the loosely packed cranial half to form the centrum or body of a vertebra. However, it is a bit more complex than this description. Cells of the sclerotome disperse around the notochord. Intersegmental arteries enter the areas where the dense and sparse cell populations of the sclerotome adjoin each other. In each sclerotome, the posterior portion has a higher proliferation of cells than its anterior portion. The cellular growth of the densely packed cells of the posterior half of the more cranial somite will proceed into the cells of the anterior half of the somite below it. Ultimately, this aggregation forms single vertebrae. Such an arrangement places the bony vertebrae out of phase with the myotomally derived segmental muscles of the trunk. This allows the contracting segmental muscles to move the vertebral column laterally. A typical vertebra arises from the fusion of several cartilagenous primordia. The centrum, which is derived from the ventromedial portions of the paired somites, surrounds the notochord and serves as a bony floor for the spinal cord. The neural arches, arising from the lateral sclerotomal cells, fuse on either side of the centrum and along with other neural arches, form a protective roof over the spinal cord. Incomplete closure of the bony roof results in a common anomaly called spina bifida occulta. The costal processes form ribs at the level of the thoracic vertebrae. At other vertebral levels, the costal processes become incorporated into the vertebrae proper. Retinoic acid (vitamin A) can cause shifts in cranial or caudal levels in overall segmental organization of the vertebrae if applied at specific developmental periods. If administered early, retinoic acid results in a cranial shift (the last cervical vertebra is transformed into the first thoracic vertebrae). Later administration of retinoic acid causes a caudal shift (thoracic vertebra extend into the first two lumbar vertebrae). Such shifts in level are called homeotic transformations and are representative of a broad family of homeotic mutations. In about 5% of humans, there are minor variations in the number or proportions of vertebrae. The KlippelFeil syndrome (brevicollis) is characterized by a short neck and low hairline due to a reduced number of cervical vertebrae. This variation is likely due to imbalance in homeobox-containing gene products. Among the vertebrae, the axis and atlas have an unusual morphology. The centrum of the atlas is deficient, but that area is replaced with the protruding odontoid process of the axis. The odontoid process consists of three fused centra: (1) a half-segment of a proatlas (not found in humans, (2) the centrum that should have been the atlas's, and (3) the normal centrum of the of the axis. This arrangement permits greater rotation of the heard about the cervical spine. 5 The ribs arise from zones of condensed mesenchymal cells lateral to the centrum. The proximal part of a rib (head, neck, tubercle) arises from the ventromedial sclerotome. By the time ossification of the vertebrae begins, the ribs separate from the vertebrae. Accessory ribs occur in the lower cervical and upper lumbar area with an incidence of about 1%. The sternum arises as a pair of cartilagenous bands at the ventral midline as the body wall consolidates. After the primordial sternal bands come together (like being zippered from top to bottom) they secondarily subdivide into craniocaudal elements. Many of these ultimately fuse to form a common unpaired body of the sternum. The split xiphoid process is readily understood from its embryological development. The clavicle is sometimes considered part of the appendicular skeleton. It is one of the first bones to become ossified. In mice, it has been shown that a certain gene helps develop the clavicle and skull. If it is defective the results are hypoplasia of the clavicle, delayed ossification of membrane bones of the skull, and open anterior and posterior fontanelles. Cleidocranial dysplasia in humans exhibits all of these conditions. Without clavicles, affected individuals can approximate their shoulders to the midline. Between the vertebrae the notochord expands into the condensed mesenchymal primordia of the intervertebral disc. In the adult the notochord persists as the nucleus pulposus. The bulk of the intervertebral disc consists of layers of fibrocartilage that differentiate from the rostral half of the sclerotome in the somite. Questions 1. Which of the following is not a precursor for the formation of either the axial, appendicular or facial bone skeleton? a. paraxial mesoderm b. lateral plate mesoderm c. neural crest d. intermediate mesoderm 2. Long bones are differentiated from which of the following tissues? a. paraxial mesoderm b. lateral plate mesoderm c. neural crest d. intermediate mesoderm 3. Which of the following is part of the neurocranium? a. skull cap b. cervical vertebrae c. bones of the face d. spinal canal 6 4. The _________ bone is not one of the bones formed partially or totally by endochondral ossification? a. temporal b. sphenoid c. frontal d. occipital 5. The viscerocranium could include the __________ bone as part of its composition. a. maxilla b. parietal c. sphenoid d. temporal 6. The viscerocranium largely incorporates _____________ for formation of its parts. a. occipital somites b. cervical somites c. neural crest d. paraxial mesoderm 7. Concerning the 1st pharyngeal arch, which of the following statements is true? a. It forms part of the frontal bone. b. The remnant of Meckel's cartilage is the stylohyoid ligament. c. Meckel's cartilage helps for the maxillae. d. The remains of Meckel's cartilage is the sphenomandibular ligament. x 8. Premature closure of the _________ sutures can produce scaphocephaly. a. lamdoidal b. sagittal c. coronal d. metopic 9. Late in the fourth week when limb buds appear, a crest of thickened tissue forms at their distal parts. Which of the following is true concerning the function of these apical ectodermal ridges? a. The AER form in the lower limb buds before the upper limb buds. b. They allow cells beneath them to proliferate and lengthen the limb bud. c. The AER induce the formation of skeletal cartilage in the mesoderm. d. The progress zones are distal to the AER. 10. The _________ contributes to the formation of the limb skeleton. a. lateral plate mesoderm b. sclerotome c. paraxial mesoderm d. dermomyotome 7 11. Which of the following statements is true? a. Joints of the limbs are formed by forming different pieces of cartilage from proximal to distal. That is, scapula, humoral, ulnar cartilages are separate made. b. The upper limbs rotate 90o laterally and the lower limbs rotate 90o medially. c. Lower limb buds appear before upper limb buds. d. The upper limbs rotate 90o medially and the lower limbs rotate 90o laterally. 12. The _________ are split into cranial and caudal halves, then the vertebrae are formed. a. myotome b. somite c. dermatome d. sclerotome 13. The cells of the ________ half of the structure correctly chosen in question #12 will increase in density and migrate into the _________ half of the next structure below to form the centrum. a. caudal / caudal b. caudal / cranial c. cranial / caudal d. cranial / cranial 14. Incomplete closure of the _________ will result in _____________. a. neural arch / spina bifida occulta b. neural arch / Klippel-Feil syndrome c. centrum / spina bifida occulta d. centrum / cleidocranial dysplasia 15. The ribs develop from mesenchymal cells of their corresponding _________ and the nucleus pulposus is the remains of the __________. a. notochord / vertebrae b. vertebrae / notochord c. sternal segment / notochord d. notochord / sternal segment