Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Cardiac contractility modulation wikipedia , lookup
Remote ischemic conditioning wikipedia , lookup
Aortic stenosis wikipedia , lookup
Hypertrophic cardiomyopathy wikipedia , lookup
History of invasive and interventional cardiology wikipedia , lookup
Drug-eluting stent wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
Cardiac surgery wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
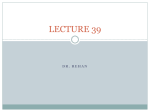
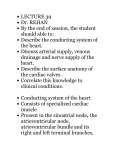
Influence of the Location of Left Anterior Descending Coronary Artery Stenosis on Left Ventricular Function During Exercise KA-HEI LEONG, M.D., AND ROBERT H. JONES, M.D. Downloaded from http://circ.ahajournals.org/ by guest on April 30, 2017 SUMMARY The purpose of this investigation was to determine if a stenosis of a coronary artery located proximally caused greater deterioration of left ventricular function than a stenosis of a similar magnitude located more distally in the artery. Twenty-six patients with isolated left anterior descending coronary artery (LAD) lesions documented by cardiac catheterization were studied by radionuclide angiocardiography (RNA) at rest and during exercise on a bicycle ergometer. Thirteen patients (nine males and four females) had a proximal lesion of the LAD averaging 91 ± 11% of the diameter of the lumen (group 1) and 13 patients (eight males and five females) had a distal lesion averaging 88 12% of the lumen (group 2). The mean age of group 1 was 49 ± 9 years and the mean age of group 2 was 48 9 years. In group 1, the ejection fraction decreased from 63 ± 8% to 55 i11% (p = 0.02), left ventricular end-diastolic volume (EDV) increased from 130 ± 32 ml to 174 ± 34 ml (p = 0.001) and left ventricular end-systolic volume (ESV) increased from 49 ± 16 ml to 80 ± 26 ml (p = 0.001) during exercise. In group 2, the ejection fraction and ESV showed no significant change during exercise. In this group, the left ventricular EDV increased from 117 ± 28 ml to 140 ± 37 ml (p = 0.04) during exercise. The two groups showed no significant hemodynamic differences during the rest studies, but group 1 showed significantly lower ejection fraction and higher EDV and ESV during exercise. These findings indicate that a stenotic lesion located at a more proximal level of the coronary arterial system reduces blood flow in a larger area of myocardium, resulting in a more pronounced ischemic response to exercise than a similar lesion located more distally. mented by coronary arteriography to have significant isolated LAD coronary artery stenosis were studied by RNA at rest and during exercise. Each patient had a baseline evaluation, including history, physical examination, ECG and chest radiograph, as well as hematologic and chemical blood profiles. Patients with episodic substernal chest tightness or pain accentuated by exercise or stress and partially or completely relieved by rest were classified as having typical angina pectoris. Patients with any uncharacteristic aspect of the pain were classified as having atypical angina. No patient had severe impairment of left ventricular function (resting ejection fraction less than 50%), cardiomyopathy, left ventricular aneurysm or congestive heart failure. Right and left cardiac catheterization and coronary arteriography were performed in each patient. Coronary arteriograms were reviewed by three observers, and the magnitude of atherosclerotic narrowing was estimated as the percent of the diameter of the artery. The magnitude of each stenotic lesion was categorized as 0%, 25%, 50%, 75%, 95% or 100% of the vessel diameter.4 The site of each stenosis was diagrammed for later tabulation. For this study, all stenoses of 75% or greater in major coronary arterial branches were defined as hemodynamically significant, and stenoses of less magnitude were considered to represent insignificant disease. This definition has been shown to correlate with ultimate prognosis at this institution." Thirteen patients showed a significant stenosis in the LAD proximal to the first perforating branch, and were designated group 1. Thirteen patients had significant stenosis in the LAD distal to the first septal perforating branch, and were designated group 2. The clinical characteristics of group 1 (table 1) were quite similar to those of group 2 (table 2). Group 1 included nine males and four females, mean age 49 RADIONUCLIDE ANGIOCARDIOGRAPHY (RNA) permits noninvasive measurement of left ventricular function in patients with coronary artery disease, and has been used to document impairment of left ventricular function in patients with coronary artery stenosis." 2 The magnitude of exercise-induced left ventricular dysfunction has been related to the anatomic extent of disease, and patients with stenosis of more than one coronary artery showed more deterioration of left ventricular function during exercise than patients with one-vessel coronary artery stenosis.3 However, a moderate amount of individual variation was observed among patients grouped by the number of stenotic vessels. This individual variation may have been the result of differences in severity of stenosis or amount of collateral perfusion. In addition, stenotic lesions located more proximally in the vessel might induce a greater functional impairment than more distally located lesions. The purpose of this investigation was to assess the functional response in two groups of patients with similar amounts of left anterior descending coronary artery (LAD) stenosis to evaluate the influence of the level of the stenosis on functional impairment during exercise. Methods Twenty-six patients admitted to Duke University Medical Center because of chest pain and docuFrom the Department of Surgery, Duke University Medical Center, Durham, North Carolina. Supported by grant HL-17670-05, SCOR, NIH. Address for correspondence: Robert H. Jones, M.D., P.O. Box 2986, Duke University Medical Center, Durham, North Carolina 27710. Received February 20, 1981; revision accepted April 27, 1981. Circulation 65, No. 1, 1982. 109 CIRCULATION 110 Downloaded from http://circ.ahajournals.org/ by guest on April 30, 2017 years, and group 2 included eight males and five females, mean age 48 years. The mean body surface area was 1.9 ± 0.2 in both groups. A prior myocardial infarction was suggested by history or ECG in seven patients of group 1 and five patients of group 2. No patient had a documented myocardial infarction within 6 months of the time of study. The number and extent of significant stenoses were similar in groups 1 and 2 when expressed as the number with a 75%, 95% or 100% stenosis. Moreover, the average of the significant stenosis was 91 ± 1 1% in group 1 and 88 ± 12% in group 2. A similar number of stenoses considered insignificant was present in both groups. Therefore, the major difference between the two groups of patients was the level of LAD stenosis. Of the 13 patients with a stenosis in the proximal LAD, seven had a stenosis located proximal to the origin of the first anterolateral branch and six distal to the first anterolateral branch but proximal to the first septal perforating branch. Four of these patients had stenoses extending more distally in the LAD, but the stenosis was significant in only one patient. In the 13 patients in group 2, the significant stenosis was located distal to the first septal perforating branch but proximal to the second anterolateral branch in each patient. Three of these 13 patients also had insignificant stenoses in the proximal LAD. An insignificant stenosis was observed in the circumflex or right coronary artery in eight patients in group I and seven patients in group 2. Propranolol was discontinued at least 24 hours before study in all patients who had received it. Rest and exercise RNA were performed for each patient by a previously described technique.6 The patient was seated in an erect position on a bicycle ergometer (Fitron, Lumex, Inc.) with a short, 21-gauge Teflon catheter placed into an external jugular vein. The heart rate was continuously monitored by telemetry of a modified CM-5 lead, and blood pressure was monitored at 1-minute intervals by a sphygmomanometer during rest, exercise and recovery. The RNA was performed from an anterior projection using a Baird Atomic System Seventy-Seven multicrystal computerized gamma camera. Data were acquired at 25-msec intervals for I minute after a LAD STENOSIS PROXIMAl TO FIRST SEPTAL PERFORATOR VENTRICULAR EJECTION FRACT ION (0/ ) 70 bolus injection of 15 mCi of technetium-99m pertechnetate. After acquisition of a resting study, exercise was begun at 200 kpm/min, and the work load was increased by 100-kpm/min increments each minute. A second RNA was obtained during exercise when the patient achieved an end point of chest pain suggestive of angina, ECG ischemic changes or 85% of maximal predicted heart rate for age. Left ventricular ejection fraction (LVEF), enddiastolic volume (EDV) and end-systolic volume (ESV) were calculated by data processing techniques that have been assessed for accuracy and reproducibility.7 Wall motion was subjectively assessed using static and dynamic images of the left ventricle throughout the cardiac cycle. The difference in individual rest and exercise measurements in each group were compared with a paired t test. The hemodynamic measurements between groups were compared by unpaired t tests. A p value less than 0.05 was considered significant. Results The exercise end points achieved were similar in the two patient groups. In the group 1 patients, with proximal LAD stenoses, heart rate increased from 74 ± 14 beats/min to 124 ± 27 beats/min and mean blood pressure increased from 94 ± 11 mm Hg to 108 ± 15 mm Hg during exercise. Four patients achieved their target heart rate and nine developed chest pain or STsegment depression during exercise. In the group 2 patients, with distal LAD stenoses, heart rate increased from 80 ± 15 beats/min to 138 ± 21 beats/min and mean blood pressure from 96 i 15 mm Hg to 113 ± 22 mm Hg during exercise. Six patients achieved their target heart rate and seven developed chest pain or ST-segment depression during exercise. In group 1 patients, LVEF decreased during exercise, from 63 ± 8% to 55 ± 11% (p = 0.02). In group 2, LVEF changed insignificantly, from 66 ± 8% to 65 ± 10% during exercise (fig. 1). Although some individual variation was apparent in group 1, only two subjects had a small increase in LVEF, and a marked decrease was the predominant change. In some patients in group 2, LVEF decreased during exercise, LAD STENOSIS DISTAL TO FIRST SEPTAL PERFORATOR 80 80 LEFT VOL 65, No 1, JANUARY 1982 T 703 60 60 - 50 50 40 40o REST EXERCISE I. .X II P-NS REST EXERCISE FIGURE 1. The 13 patients with a left anterior descending coronary artery (LAD) stenosis proximal to the first septal perforator show a marked decrease of left ventricular ejection fraction (L VEF) during exercise. Thirteen patients with a distal stenosis of the LA D had no change in L VEF during exercise. Although L VEF decreased in some patients in this group, in more than half of the patients it increased during exercise. LOCATION OF LAD STENOSIS/Leong and Jones LAD STENOSIS DISTAL TO FIRST SEPTAL PERFORATOR LAD STENOSIS PROXIMAL TO FIRST SEPTAL PERFORATOR O LEFT VENTRICULAR -, END DIASTOLIC 140 VOLUME (M) 100 OU I- 140 iIi 1 100 60 P0 REST EXERCISE 60 Downloaded from http://circ.ahajournals.org/ by guest on April 30, 2017 LAD STENOSIS PROXIMAL TO FIRST SEPTAL PERFORATOR ,'/ 110 ...I 90 LEFT VENTRICULAR END SYSTOLIC VOLUME (M L) 70 50 K- 30 REST EXERCISE FIGURE 2. The two groups of patients showed an increase of end-diastolic volume (EDV) during exercise. However, the increase of EDV with exercise is more pronounced in patients with a proximal lesion of the left anterior descending coronary artery (LAD) than in patients with a distal lesion. P 0 04 REST but in more than half of this group LVEF increased during exercise. The EDV increased during exercise, from 130 ± 32 ml to 174 ± 34 ml (p = 0.001) in group 1 and from 1 17 + 28 ml to 140 i 37 ml (p = 0.04) in group 2 (fig. 2). The increase in group I was significantly greater than that in group 2 (p = 0.02). During exercise, ESV increased in all patients in group 1, and the group average increase was from 49 i 16 ml to 80 ± 26 ml (p = 0.001) (fig. 3). Patients in group 2 showed an insignificant ESV change, from 41 ± 15 ml to 50 ± 22 ml. Although some patients in group 2 increased ESV, others decreased ESV during exercise. Ten patients in group 1 had normal wall motion at rest, five of whom developed wall motion abnormalities during exercise. The three patients in this group with abnormal wall motion at rest all developed new wall motion abnormalities during exercise. Eleven patients in group 2 had normal wall motion at rest, four of whQm had exercise-induced wall motion abnormalities. Two patients in this group had abnormal wall motion both at rest and during exercise. Hemodynamic measurement during rest and exercise of the two groups are compared in table 3. Resting measurements were not significantly different between the groups. During exercise, patients in group I had a lower LVEF (p = 0.02), greater EDV (p = 0.02) and greater ESV (p = 0.004) than patients in group 2. - III EXERCISE Discussion Normal subjects exercising in the erect position typically increase left ventricular stroke volume more than EDV, resulting in an increase in ejection fraction and a decrease in ESV. Patients with coronary artery disease typically increase EDV more than stroke volume, resulting in a decrease in ejection fraction and increase in ESV during exercise. Patients grouped by the number of major coronary arteries with a significant stenosis show a clear relationship between the magnitude of exercise-induced left ventricular dysfunction and the anatomic extent of disease.3 During exercise, the patient group with stenosis of the left main or all three major coronary arteries shows the greatest average decrease in ejection fraction and has the smallest number of patients who maintain normal left ventricular function. Patients with stenosis of only one major coronary artery show a smaller decrease in ejection fraction during exercise than patients with three stenosed arteries, but left ventricular function remains abnormal compared with groups of normal subjects. However, a large amount of individual variation occurs, and many patients with stenosis of one coronary artery have left ventricular function that appears entirely normal during exercise. The presence and magnitude of exercise-induced left ventricular dysfunction in an individual patient might result from a number of factors, such as age, sex, history of prior myocardial infarction, level of exercise stress achieved, level of exercise conditioning, magnitude of LAD STENOSIS DISTAL TO FIRST SEPTAL PERFORATOR FIGURE 3. The 13 patients with a proximal stenosis of the left anterior descending coronary artery (LAD) all show an increase of end-systolic volume (ESV) during exercise. In patients with a distal LAD stenosis, ESV did not change significantly during exercise. However, some patients in this group could decrease ES V, reflecting enhanced contractility during exercise. 112 CIRCULATION VOL 65, No 1, JANUARY 1982 Downloaded from http://circ.ahajournals.org/ by guest on April 30, 2017 TABLE 1. Clinical, Coronary Arteriogram and Radionuclide Angiographic Data in 13 Patients with Significant Stenosis of Proximal Left Anterior Descending Coronary Artery Coronary arteriography - percent stenosis Proximal LAD Distal LAD Angina Age Previous Proximal Distal to Distal to BSA Proximal to Pt to first AL first AL second AL second AL (years) Sex (M2) Type Class Ml 41 M IV Yes LP 1.81 Typical 100 0 0 0 51 M III No GS 1.85 Typical 100 0 0 0 M JA 32 IV Yes 2.09 Typical 100 0 0 0 No JC 47 M IV 95 1.92 Typical 0 50 50 RM 62 2.16 Typical II Yes M 95 25 50 0 JK 37 No M 2.09 Atypical 75 75 0 0 F No IT 55 1.80 Atypical 75 0 0 25 II JH 54 F 1.62 Typical Yes 0 100 75 0 II M TG 53 2.24 Typical Yes 0 100 0 0 CW M IV 58 1.97 Typical Yes 0 0 100 0 M BE 47 1.88 Typical III Yes 0 95 0 25 61 F HC No 1.55 Atypical 0 75 0 0 ME F 50 1.48 Atypical No 0 75 0 0 Abbreviations: BSA - body surface area; Angina Class = New York Heart Association classification; Proximal LAD -left anterior descending coronary artery proximal to origin of first septal perforating branch; Distal LAD = LAD distal to first septal perforating branch; AL = anterolateral branch of LAD; Circumflex = left circumflex coronary artery; Right = right coronary artery; Ex exercise. intravascular blood volume and magnitude and location of the stenosis in the coronary arteries. The purpose of this investigation was to evaluate the hypothesis that stenosis' located proximally caused a greater amount of exercise-induced left ventricular dysfunction than a stenosis of similar magnitude located more distally in an artery. The most- dissimilar characteristic of the two patient studied appeared to be the level of stenosis within the LAD. Left ventricular function during exercise clearly differed in the two groups, and at lower ejection fraction and higher EDV and ESV during exercise were observed -in -the group with the proximal stenosis. Documentation that the level of a coronary artery stenosis influences the response of the left ventricle to exercise is consistent with the concept that the groups TABLE 2. Clinical, Coronary Arteriogram and Radionuclide Angiographic Data in 13 Patients with Significant Stenosis of Distal Left AnteriorDescending Coronary Artery Coronary arteriography-percent stenosis Proximal LAD Distal LAD Angina Age BSA Previous Proximal Distal to Proximal to Distal to Pt to first AL second AL second AL first AL (years) Sex (m2) Type Class MI MC F 50 1.68 Typical II Yes 50 25 100 0 BK 62 F 1.64 Typical IV No 50 50 100 0 M GB 46 1.73 Atypical No 0 0 100 0 SM M 41 1.97 Typical IV Yes 0 0 100 0 M WD 51 2.00 Atypical No 0 0 0 100 MK 44 F 1.40 Atypical Yes 0 0 100 0 M RW 64 1.89 Typical III No 0 0 95 0 M WB 37 1.94 Atypical No 0 25 75 0 RW 57 F 1.83 Atypical No 0 0 75 0 M II JA 54 2.37 Typical Yes 0 0 75 0 RC 37 F 1.71 Atypical No 0 0 75 0 M RM 34 2.03 Atypical Yes 0 0 75 0 M HY 50 2.05 Typical IV No 0 0 75 0 Abbreviations: BSA = body surface area; Angina Class New York Heart Association classification; Proximal LAD left anterior descending coronary artery proximal to origin of first septal perforating branch; Distal LAD = LAD distal to first septal perforating branch; AL = anterolateral branch of LAD; Circumflex = left circumflex coronary artery; Right right coronary artery; Ex = exercise. 113 LOCATION OF LAD STENOSIS/Leong and Jones TABLE 1. (Continued) Downloaded from http://circ.ahajournals.org/ by guest on April 30, 2017 Circumflex 50 0 0 25 0 0 0 0 50 0 25 0 0 Right 50 50 0 25 25 0 0 25 25 50 0 0 0 Ejection fraction (%) Rest Ex 56 47 72 38 67 67 71 66 65 70 61 53 62 51 56 47 53 51 54 60 67 51 80 74 57 42 Radionuclide angiography End-diastolic End-systolic volume (ml) volume (ml) Rest Ex Rest Ex 152 238 67 126 180 178 50 110 160 212 53 70 96 171 28 58 99 126 35 38 153 189 60 89 137 170 52 83 67 130 30 69 154 175 72 86 153 182 70 73 129 204 43 100 98 120 24 39 114 174 49 101 magnitude of exercise-induced left ventricular dysfunction relates to the quantity of myocardium that becomes ischemic during exercise. The observation that patients with a stenosis proximal to the first perforating septal branch of the LAD have a greater magnitude of exercise-induced left ventricular dysfunction than similar patients with a more distal stenosis suggests other important clinical differences between the two groups. The quantity of myocardial tissue dependent upon a major coronary artery could be expected to decrease progressively as flow progresses more distally in the vessel. Therefore, the larger amount of potentially ischemic myo- Wall motion abnormalities Rest Ex No Yes Yes Yes No No No No No No No Yes No No No Yes Yes Yes Yes Yes No Yes No No No Yes cardium in patients with a proximal LAD stenosis suggests that this group would have a less favorable prognosis than patients with lesions located more distally. Coronary atherosclerosis involving only one major vessel is usually associated with a good prognosis. However, an isolated stenosis of the LAD may be a more serious lesion than a single stenosis of the right or circumflex coronary arteries.10 13 Moreover, the anatomic site of the stenosis of the LAD may also influence prognosis.14 Webster and associates'5 noted that the 6-year mortality rate in patients with a proximal lesion of the- LAD was 29% compared with 21% for a distal LAD lesion. Schuster TABLE 2. (Continued) Ejection fraction(%) Circumflex Right Rest 0 0 50 50 0 0 0 0 0 0 0 0 0 50 0 25 0 25 25 25 0 25 0 0 0 0 68 58 65 53 56 71 70 63 71 64 87 64 69 Ex 52 72 49 62 70 81 76 76 57 67 51 59 67 Radionuclide angiography End-diastolic End-systolic volume (ml) volume (ml) Ex Ex Rest Rest 41 93 127 204 41 132 145 55 122 76 149 43 141 113 103 110 125 113 168 45 130 101 145 128 69 117 156 161 164 69 153 167 66 50 30 33 46 33 61 6 47 31 55 39 13 28 37 69 54 16 63 55 Wall motion abnormalities Rest Ex No Yes No No Yes No No No Yes Yes No No No No No No No Yes No No No No No Yes No No 114 CI RCULATION TABLE 3. Comparison of Hemodynamic Measurements Between the Patients with a Proximal and Patients with a Distal Left Anterior Descending Coronary Artery Stenosis Exercise Rest Hemodynamic variables NS NS Heart rate (beats/min) NS NS Mean blood pressure (mm Hg) Left ventricular ejection 0.02 NS fraction (%) 0.02 NS End-diastolic volume (ml) 0.004 NS End-systolic volume (ml) NS NS Stroke volume (ml) NS NS Cardiac output (1/min) NS NS Cardiac index (1/min) Downloaded from http://circ.ahajournals.org/ by guest on April 30, 2017 and associates"6 also observed that the incidence of fatal acute myocardial infarction in patients with a proximal LAD lesion was 66%, compared with 9% in patients with a distal LAD lesion. Kumpuris and colleagues17 found the magnitude of depressed LVEF ejection fraction after myocardial infarction to be greater in patient groups with an isolated proximal LAD stenosis than in patients with an isolated LAD stenosis located more distally. The patients showed a large amount of individual variation in hemodynamic response to exercise. This variation was not entirely explained by the level or magnitude of stenosis. Other anatomic differences that could alter regional myocardial perfusion, such as the presence of collateral vessels and the relative size of the diseased and undiseased vessels, could not be assessed in this small patient population. Irrespective of the anatomic reason, individual difference in exercise-induced left ventricular dysfunction would be of great clinical importance if the magnitude of abnormality reflected the quantity of potentially ischemic myocardium in individual patients. However, documentation of a more abnormal response in a patient group anticipated from coronary arteriography to have a larger mass of jeopardized myocardium does not confirm this relationship in individual patients. Moreover, no information is available to document whether individual differences in exercise-induced left ventricular dysfunction tend to predict progression of angina, myocardial infarction or death. Evaluation of the prognostic information associated with individual measurements of left ventricular function during exercise is an-important topic for further investigation. VOL 65, No 1, JANUARY 1982 References 1. Rerych SK, Scholz PM, Newman GE, Sabiston DC Jr, Jones RH: Cardiac function at rest and during exercise in normals and in patients with coronary heart disease: evaluation by radionuclide angiocardiography. Ann Surg 187: 449, 1978 2. Newman GE, Rerych SK, Upton MT, Sabiston DC Jr, Jones RH: Comparison of electrocardiographic and left ventricular changes during exercise. Circulation 62: 1204, 1980 3. Jones RH, McEwan P, Newman GE, Port S, Rerych SK, Scholz PM, Upton MT, Peter CA, Austin EH, Leong K, Gibbons RJ, Cobb FR, Coleman RE, Sabiston DC Jr: Accuracy of diagnosis of coronary artery disease by radionuclide measurement of left ventricular function during rest and exercise. Circulation 64: 586, 1981 4. Hartman CW, Kong Y, Margolis JR, Warren SG, Peter RH, Behar VS, Oldham HN Jr: Aortocoronary bypass surgery: correlation of angiographic, symptomatic and functional improvement at one year. Am J Cardiol 37: 352, 1976 5. Harris PJ, Behar VS, Conley MJ, Harrell FE Jr, Lee KL, Peter RH, Kong Y, Rosati RA: The prognostic significance of 50% coronary stenosis in medically treated patients with coronary artery disease. Circulation 62: 240, 1980 6. Jones RH, Douglas JM, Rerych SK, Newman GE, Sabiston DC Jr: Noninvasive radionuclide assessment of cardiac function in patients with peripheral vascular disease. Surgery 85: 59, 1979 7. Scholz PM, Rerych SK, Moran JF, Newman GE, Douglas JM, Sabiston DC Jr, Jones RH: Quantitative radionuclide angiocardiography. Cathet Cardiovasc Diagn 6: 265, 1980 8. Sandler H, Dodge HT: Use of single plane cineangiocardiogram for calculation of left ventricular volume in men. Am Heart J 75: 325, 1968 9. Upton MT, Rerych SK, Newman GE, Bounous EP Jr, Jones RH: The reproducibility of radionuclide angiocardiographic measurements of left ventricular function in normal subjects at rest and during exercise. Circulation 62: 126, 1980 10. Abedin Z, Dack S: Isolated left anterior descending coronary disease: choice of therapy. Am J Cardiol 40: 654, 1977 11. Brymen JF, Butter TH, Walton JA, Willis PW III: A natural history study of the prognosis role of coronary arteriography. Am Heart J 88: 139, 1974 12. Hamby RI, Gupta MP, Young MW: Clinical and hemodynamic aspect of single vessel coronary artery disease. Am Heart J 85: 458, 1973 13. Kouchoukos NT, Oberman A, Russell RO Jr, Jones WB: Surgical versus medical treatment of occlusive disease confined to the left anterior descending coronary artery. Am J Cardiol 35: 836, 1975 14. Bakst A, Lewis BS, Gotsman MS: Isolated obstruction of the left descending coronary artery. S Afr Med J 47: 1534, 1973 15. Webster JS, Moberg CH, Rincon G: Natural history of severe proximal coronary artery disease as documented by coronary cineangiography. Am J Cardiol 33: 195, 1974 16. Schuster EH, Griffith LS, Bulkley BH: Preponderance of acute proximal left anterior descending coronary lesions in fatal myocardial infarction. (abstr) Circulation 60 (suppl II): 11-60, 1979 17. Kumpuris AG, Quinones MA, Kanon D, Miller RR: Isolated stenosis of left anterior descending or right coronary artery: relation between site of stenosis and ventricular dysfunction and therapeutic implications. Am J Cardiol 46: 13, 1980 Influence of the location of left anterior descending coronary artery stenosis on left ventricular function during exercise. K Leong and R H Jones Downloaded from http://circ.ahajournals.org/ by guest on April 30, 2017 Circulation. 1982;65:109-114 doi: 10.1161/01.CIR.65.1.109 Circulation is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Copyright © 1982 American Heart Association, Inc. All rights reserved. Print ISSN: 0009-7322. Online ISSN: 1524-4539 The online version of this article, along with updated information and services, is located on the World Wide Web at: http://circ.ahajournals.org/content/65/1/109.citation Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in Circulation can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for which permission is being requested is located, click Request Permissions in the middle column of the Web page under Services. Further information about this process is available in the Permissions and Rights Question and Answer document. Reprints: Information about reprints can be found online at: http://www.lww.com/reprints Subscriptions: Information about subscribing to Circulation is online at: http://circ.ahajournals.org//subscriptions/