Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
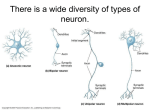
بسم هللا الرحمن الرحيم ﴿و ما أوتيتم من العلم إال قليال﴾ صدق هللا العظيم االسراء اية 58 By Dr. Abdel Aziz M. Hussein Assist Prof of Medical Physiology Objectives • • • • • • • • • • 1. definition of pain 2. types of pain 3. Body reactions or responses to pain 4. perception of pain 5. neural pathways for pain 6. referred and radiating pain 7. modulation of pain perception 8. endogenous analgesia system 9. gate control theory 10. applications of this theory (acupuncture and TENS) Def : •Pain is an unpleasant sensory and emotional experience associated with actual or potential tissue damage according to; International association for the study of pain (IASP). Significance: 1. Pain is a warning signal for tissue damage. It is the prominent symptom of tissue damage 2. Pain has a protective function. It initiates protective reflexes that; •Get rid of the painful stimulus. •Minimize tissue injury or damage. A) According to its mechanism or cause: •Pain is classified into 3 main types; 1. Physiological Pain Also called Nociceptive pain Caused by stimulation of pain receptors by tissues damage e.g. in inflammation 2. Pathological Pain Also called neuropathic pain Caused by damage of nerve pathway 3. Psychogenic Pain In depression and anxiety Difficult to differentiate whether 2ry to or actual cause of pain N.B. Neuropathic pain: according to site of injury is classified into; a. Central → Central pain e.g. thalamic infarct b. Peripheral → e.g. nerve compression, neuralgias. c. Mixed → e.g. post herpetic neuralgia. Character: neuropathic pain is characterized by burning, tingling, numbness, squeezing, itching, constant +/- intermittent shooting, and electric. B) According to its duration: •Both nociceptive and neuropathic pains are classified into 2 types; a) Acute pain: less than 7 weeks b) Chronic pain : more than 7 weeks C) According to the quality or character : •A pain it is classified into 5 types; a) Pricking or Cutting Pain: b) Burning Pain: c) Aching Pain: d) Throbbing Pain: e) Colicky Pain: 1. Pricking pain • Sharp and localized pain. • Of skin origin (mainly) • e.g. in pricking or cutting the skin by sharp object 2. Burning pain • Less well localized, has unpleasant burning nature. • Usually of skin origin • Caused by wide spread irritation of skin 3. Aching pain 4.Throbbing pain 5.Colicky pain • disagreeable pain of dull- aching nature • More diffuse and felt coming from deeper tissues e.g. rheumatic pains • Fluctuation of its intensity with arterial pulsations • localized inflammation in deep tissues e.g. abscess • Comes in cramps, so it has a colicky nature, e.g. intestinal colic and ureteric colic • Spasm of smooth ms in the walls of hollow viscera D) According to site of origin: 3 types; Cutaneous pain • Pain comes from skin and subcutaneous tissues • Usually pricking or burning pain Deep pain • Pain comes from structures deep to the skin e.g. skeletal muscle, joints, and tendons • Usually dull aching or throbbing Visceral pain • Pain comes from internal viscera e.g. stomach • Usually colicky or dull aching 1) Somatic reactions: a) Withdrawal reflex : • It occurs in cutaneous pain • This is a protective reaction which get rid of injurious agent b) Reflex spasm of nearby muscle: • It occurs in deep pain • It immobilize pained parts to decrease pain sensation c) Reflex spasm of overlying muscle: • It occurs in visceral pain • It produce guarding rigidity of abdominal muscle (guarding reaction) 2) Autonomic reactions: • • Mild and moderate cutaneous pain → sympathetic stimulation → ↑ heart rate and ABP (pressor reaction) Sever cutaneous, deep, and visceral pain → parasympathetic stimulation →↓ HR and ABP (depressor reaction) 3) Emotional or psychogenic reactions: • In the form anxiety, fear, crying, and depression • These reactions vary: a. From person to person on exposure to similar pain stimuli. b. In the same person according to his emotional state: -Worry about the cause of pain augment the feeling of pain. -Strong emotional excitement & sever physical exertion may block the feeling of pain. -Thus, seriously wounded soldiers in a battlefield suffer little or no pain till the battle is over. 4) Cutaneous hyperalgesia: •It is 2 types; PRIMARY Site: Duration Characteristics: Mechanism: In the red area SECONDARY In healthy skin area around red area It develops within 30 to 60 It duration is much shorter than minutes and lasts for several that of 1ry hyperalgesia hours or days after injury. When non-noxious stimuli When a noxious stimulus is such as touch or mild applied, the pain felt is more warming are applied they severe than usual. cause pain. It is due to lowered Convergence -Facilitation threshold of pain receptors in theory: the red area due to local -No lowering of the pain threshold axon reflex -The pain impulses from the area of 1ry hyperalgesia facilitates (↑ed excitability) those from the area of 2ry hyperalgesia. Area of injury Area of redness Healthy skin Antidromic impulse Secreting substance P Area of injury Area of redness Healthy skin Convergence facilitation Pain sensation Painful stimulus 22 1)Types: •They are morphologically similar but functionally they are specific a) Morphological types: are specific free nerve endings b) Functional types: classified according to their adequate stimulus into:1) Mechanical Pain Rs: • Respond to strong mechanical forces, such as cutting, or pricking 2) Thermosensitive pain Rs: • Respond to excessive changes in temp. (above 45°C and below 10°C). 3) Chemical Pain Rs: respond to noxious chemical stimuli. 4) Polymodal Pain Rs: • Respond to a combination of mechanical, thermal, and chemical noxious stimuli 2)Distribution: • Pain Rs are found in most tissue of the body. a) Abundant in the skin and some internal tissue such as the periosteum, arterial wall, joint surfaces, and the dura of the tentorium cerebelli. b) Few in deep tissues and all viscera. So, for pain to occur, painful stimulus must by intense and widespread. The deep & visceral pain is poorly localized. c) Brain itself and the parenchymal tissues of the liver, kidneys, and lungs have no pain receptors “pain insensitive structures” N.B.: Serious diseases in these organs don’t produce pain till they extend to a pain sensitive structure like arterial wall or serous covering. 3) Mechanism of stimulation: Chemical stimuli Mechanical stimuli Thermal stimuli Strong acids or Alkalies Cutting or pricking temp. > 45 C and < 10 C Tissue damage 1st class K ions, Histamine, Serotonin, and Bradykinin Directly stimulate Pain Receptors Release of Pain Producing Compounds (PPS) 2nd class PGE2, leukotriens and Substance P Sensitize the pain Rs by lowering its threshold to stimuli Tissue Damage Direct stimulators Sensitizers 4) Adaptation: • Pain Rs do not adapt to continuing noxious stimuli • This serves a protective function to keep the individual trying to remove the damaging stimulus or to get away from it. Pathway: Neospinothalamic tract A) 1st order neuron : • A delta afferent fibers • End in lamina I of dorsal horn of spinal cord B) 2nd order neuron : • Axons of neurons lamina I of dorsal horn of spinal cord cross the opposite side in front of central canal and ascend as neospinothalamic in spinal cord and as spinal leminiscus in brain stem • End in posteroventral nucleus of thalamus (PVNT) Pathway: C) 3rd order neuron : • Axons of neurons of PVNT ascend in sensory radiations • End in primary somatic sensory area (area 3,1,2) Note: • The chemical transmitter released at the central end of A delta fibers that carry fast pain is glutamate PVNT Sensory Radiations Spinal Leminiscus Lamina I A delta Receptors Free nerve endings Lateral spinothalamic tract Pathway: Paleospinothalamic tract A) 1st order neuron : • C afferent fibers • End in lamina II and III (called substantia Gelatinosa of Rolandi SGR) of dorsal horn of spinal cord B) 2nd order neuron : • Axons of neurons SGR of dorsal horn of spinal cord cross the opposite side in front of central canal and ascend in spinal cord and as; 1. Spinoreticular tract end in RF of MO and Pons 2. Spinotectal tract end in PAG areas of midbrain 3. Paleospinothalamic tract end in non specific thalamic nuclei (intralaminar and midline) Pathway: C) 3rd order neuron : • Axons of neurons from RF and NSTN of thalamus ascend in sensory radiations • Terminate diffusely in all areas of the cerebral cortex Note: • The chemical transmitter released at the central end of c fibers that carry fast pain is substance P All cortical areas Non-specific nuclei of thalamus Periaqueductal gray area (PAG) in midbrain Reticular formation In MO and Pons SGR Laminae II, III Receptors Free nerve endings Afferent C fibers Paleospinothalamic tracts Comparisons Between Slow and Fast Pain Source Stimulus Quality Onset Duration Localization Afferent Tract Centre Chemical trans. Acute (Fast) Chronic (Slow) Skin only Skin, deep tissues, and viscera All types Mechanical and thermal Pricking Within 0.1 sec after stimulation Short (one second) Well –localized A-delta Neospinothalamic tract Cerebral cortex Glutamate Burning One or more seconds after stimulation Long (few minutes) Diffuse C Paleospinothalamic tract Thalamus Substance P Def: • • Referred pain is pain felt away from the site of its origin Radiating pain is pain appear to migrate away from the its original site • Referred pain is a part of radiating pain N.B. • Visceral pain usually referred, deep pain may be referred but cutaneous pain never referred Site of referral is determined by dermatomal rule: •The pain from a viscera is referred to a somatic structure (skin or deep structure) which were developed in the same embryonic segment and supplied by the same dorsal root ganglia. •Abnormal sites are due to migration of viscera. Mechanism : Convergence Projection Theory: • • • • Afferents pain fibers from skin area and diseased viscera converge on the same 2nd order neuron and finally stimulate the same cortical neuron The cortex project (feel) pain as it is coming from the skin because the sensory cortex is accustomed to receive pain from the skin Skin is the commonest site of pain Convergence may occurs also at the level of thalamus or sensory cortex • There is endogenous analgesic system as proved by: 1. Stress analgesia e.g. soldiers wounded by the heat of the battle may feel no pain until the battle is over. 2. The pain felt from an injured area is reduced when the skin around the injured area is rubbed or stroked. 3. Morphine injected in minute doses in experimental animals in the third ventricle of the brain produce marked analgesia. • This Pain Control System can modulate pain sensation (mainly inhibitory) by release of endogenous opiate like (opioid) peptides such as encephalins, endorphins • It cause both presynaptic and postsynaptic control of nociception in the dorsal horn via enkephalin release which inhibits release of substance P, transmitter at pain nerve endings 1) Def, • System which control pain transmission in CNS or inhibit pain transmission i.e. endogenous analgesia system 2) Sites: 1.Periventricular area of hypothalamus 2.Periaqueductal area (PAG) around aqueduct of sylivus in midbrain and Pons 3. Nucleus raphe magnus (NRM) AND Nucleus reticularis paragigantocellularis (NRPG) in lower Pons and upper medulla 4. Pain inhibitory complex (PIC): interneuron in dorsal horn of spinal cord 3) Neurochemistry: • This system act through the release of endogenous opioid peptides which act on opiate receptors. Opioid peptides: • They include 3 groups; enkephalins, endorphins and dynorphins. Opiate Receptors: • 3 types of opiate receptors : delta (δ), kappa (κ), and muta (μ). Enkephalins bind with the delta (δ) receptors Endorphins bind with the muta (μ) receptors Dynorphins bind with the kappa (κ) receptors. •These receptors can be blocked by naloxone, which is a morphine antagonist Activation of the Pain Control System Clinical (Experimental) Natural (physiological) 1- Electrical stimulation of certain regions of pain control system Exposure to severe stress, particularly when associated with strong emotional excitement. 2- Local application of opiates (such as morphine) at particular regions in the nervous system. Stress induced analgesia (pharmacological analgesia) Periventricular nucleus of hypothalamus Endorphins ++ Periaqueductal gray area Encephalin ++ Stress Nucleus raphe magnus Serotonin ++ Ascending pathway Encephalins -Substance P Posterior horn of spinal cord 1st order neuron of pain • The sites of synapses along the pain pathway are considered as gates through which pain transmission can be; Facilitated (if the gate is open) or Blocked (if the gate is closed). Sites: The main pain gates are: 1- Spinal gate: at the SGR. 2- Brain stem gate: at the nuclei of reticular formation. 3- Thalamic gate: At neurons of PVLNT & intalaminar thalamic nuclei. 3 2 1 At spinal gate pain transmission is blocked by; 1. Descending inhibitory impulses through the pain control system activating enkephalin-secreting interneuron 2. Stimulation of the large diameter nerve fibers (A delta and A beta) terminating peripherally in mechanoreceptors, such as tactile receptors or proprioceptors (A beta), and pricking pain fibers (A delta). • • This may explain why simple maneuvers such as rubbing the skin (thus exciting tactile and pressure receptors), near a painful area is often effective in relieving certain types of pain → A beta Also block of pain by acupuncture (A delta fibers) Interneuron Rubbing of the skin A beta fibers Pain C fiber Painful stimuli Interneuron Acupuncture A delta fibers Pain C fiber Painful stimuli • This theory provides basis for various methods of pain relief 1. Massaging a painful area 2. Applying irritable substances to a painful area (counter-irritation) 3. Transcutaneous Electrical Nerve Stimulation (TENS) 4. Acupuncture ? •Acupuncture has been practiced in China for more than 4000 years as a method for pain relief. Mechanism: 1- Needles in appropriate body regions are thought to excite certain sensory neural pathways which feed into the brain stem centers (such as the PAG) involved in the pain control system, with release of endogenous opioid peptides. 2- Simultaneous suppression of pain transmission at the spinal pain-gate by acupuncture Def., •TENS is any stimulating device which delivers electrical currents across the intact surface of the skin Mechanism: •TENS causes relieve of pain by activate large diameter ‘touch’ fibres (Aβ) without activating smaller diameter nociceptive fibres (Aδ and C) this causes; 1- Excitation of certain sensory neural pathways which activate PAG area involved in the pain control system, with release of endogenous opioid peptides. 2- Simultaneous suppression of pain transmission at the spinal pain-gate by acupuncture TENS Physical conditions Conditions that open the Gate Extent of injury Extra activity Conditions that closes the Gate medications Counter stimulation, e.g. massage, heat Emotional conditions Depression, tension Anxiety, worry Relaxation Positive emotion Mental conditions Focusing on pain Distraction Involvement in life activity THANKS