Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Specialty drugs in the United States wikipedia , lookup
Discovery and development of tubulin inhibitors wikipedia , lookup
Discovery and development of proton pump inhibitors wikipedia , lookup
Polysubstance dependence wikipedia , lookup
Compounding wikipedia , lookup
Plateau principle wikipedia , lookup
Orphan drug wikipedia , lookup
Psychopharmacology wikipedia , lookup
Drug design wikipedia , lookup
Drug discovery wikipedia , lookup
Pharmacogenomics wikipedia , lookup
Neuropsychopharmacology wikipedia , lookup
Pharmacognosy wikipedia , lookup
Pharmaceutical industry wikipedia , lookup
Neuropharmacology wikipedia , lookup
Prescription costs wikipedia , lookup
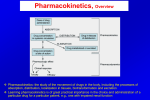
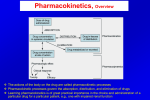
Pharmacology PHL 211 Eighth Lecture By Abdelkader Ashour, Ph.D. Phone: 4677212 Email: [email protected] Pharmacokinetics, Overview Pharmacokinetics: the study of the movement of drugs in the body, including the processes of absorption, distribution, localization in tissues, biotransformation and excretion Learning pharmacokinetics is of great practical importance in the choice and administration of a particular drug for a particular patient, e.g., one with impaired renal function Pharmacokinetics, Introduction Drugs need to achieve an adequate concentration in their target tissues The two fundamental processes that determine the concentration of a drug at any moment and in any region of the body are: – translocation of drug molecules – chemical transformation by drug metabolism and other processes involved in drug elimination These are critically important for choosing appropriate routes of administration Translocation of drug molecules: drug molecules move around the body in two ways: bulk flow transfer (i.e. in the bloodstream) The chemical nature of a drug makes no difference to its transfer by bulk flow diffusional transfer (i.e. molecule by molecule, over short distances) Diffusional transfer (transmembrane movement of the drugs): ability to cross hydrophobic diffusion barriers is strongly influenced by lipid solubility. delivering drug molecules to and from the non-aqueous barriers is influenced by water solubility The Movement of Drug Molecules Across Cell Barriers Cell membranes form the barriers between aqueous compartments in the body. The most universal function of cell membrane is to act as a selective barrier to the passage of molecules, allowing some molecules to cross while excluding others. The cell membrane consists of a bimolecular lipid sheet (hydrophobic) interspersed with protein molecules (hydrophilic), and contains minute aqueous pores which allow passage of small hydrophilic substances. The Movement of Drug Molecules Across Cell Barriers Gaps between endothelial cells are packed with a loose matrix of proteins that act as filters, retaining large molecules and letting smaller ones through. Aqueous Diffusion: It occurs within the larger aqueous compartments of the body (interstitial space, cytosol, etc) and across epithelial membrane tight junctions and the endothelial lining of blood vessels through aqueous pores It is important also in the transfer of gases such as carbon dioxide In other organs, especially in the CNS (blood brain barrier, BBB) and the placenta (placental barrier), There are tight junctions between the cells the endothelium is enclosed in an impermeable layer of periendothelial cells (pericytes) These features prevent potentially harmful molecules from leaking from the blood into these organs and have major pharmacokinetic consequences for drug distribution The Movement of Drug Molecules Across Cell Barriers Passage of drugs across cell membranes 1) Passive transfer: a. Simple diffusion: The vast majority of drugs gain access to the body through this mechanism. Drugs must be first in aqueous solution to gain access to the lipid membrane Drugs pass along concentration gradient No energy or carrier is required It is not inhibited by metabolic inhibitors It is not saturable It depends on: concentration gradient lipid solubility degree of ionization, thickness of membrane molecular size Concentration gradient is maintained by removal of the drug from other side of the membrane Lipid solubility is measured by lipid/water partition coefficient (ratio of drug concentration in lipid phase and water phase when shaken in one immiscible lipid/water system). Ionized drugs generally have low lipid/water coefficient The Movement of Drug Molecules Across Cell Barriers, Lipid solubility: weak acids and weak bases/Clinical Significance In drug poisoning, renal elimination of drugs can be enhanced by changing urinary pH to increase drug ionization and inhibits tubular reabsorption. Alkalinization of urine by NaHCO3 increases excretion of acidic drugs e.g. aspirin. Acidification of urine by vitamin C or NH4Cl increases excretion of weak base drugs e.g. amphetamine. The Movement of Drug Molecules Across Cell Barriers, contd. b. Filtration: In capillaries, pores have large size and so nearly all free drugs in plasma can be filtered. It depends on hydrostatic and osmotic pressure, so it is limited by blood flow but not by lipid solubility and it is not saturable 2) Specialized transport: - Substances that are too large or poorly lipid soluble as amino acids and glucose are carried by specialized carriers - a. Facilitated diffusion: is similar to simple diffusion but requires a carrier and it is saturable - A carrier molecule is a transmembrane protein which binds one or more molecules or ions, changes conformation and releases them on the other side of the membrane - Carrier molecules facilitate entry and exit of physiologically important molecules, such as sugars, amino acids, neurotransmitters and metals The Movement of Drug Molecules Across Cell Barriers, contd. b. Active transport: where drugs pass against concentration gradient, so it requires: energy, carrier (thus it is saturable) Example: many drugs, especially weak acids (e.g., penicillin, uric acid) and weak bases (e.g., histamine), are actively secreted into the renal tubule, and thus more rapidly excreted Mechanism Direction Energy required Carrier Saturable Passive diffusion Along gradient No No No Facilitated diffusion Along gradient No Yes Yes Active transport Against gradient Yes Yes Yes The Movement of Drug Molecules Across Cell Barriers, contd. c. Pinocytosis: It involves Invagination of part of the cell membrane and the trapping of a small vesicle containing extracellular constituents within the cell The vesicle contents can then be released within the cell, or extruded from its other side Examples: Pinocytosis of vitamin B12 (complexed with intrinsic factor). It is important for the transport of some macromolecules (e.g. insulin, which crosses the blood–brain barrier by this process) Plasma level curve Cmax = maximal drug level obtained with the dose. tmax = time at which Cmax occurs. Lag time = time from administration to appearance in blood. Onset of activity = time from administration to blood level reaching minimal effective concentration (MEC). Duration of action = time plasma concentration remains greater than MEC. Time to peak = time from administration to Cmax. Routes of Administration A route of a drug administration is the path by which a drug is brought into contact with the body The pharmacokinetic properties of a drug are critically influenced by the route of administration Drug must be transported from the site of entry to the target tissue Classification: I. Enteral (any form of administration that involves any part of the GIT): desired effect is systemic (non-local). Drug is given via the digestive tract II. Parenteral: desired effect is systemic. Drug is given by injection III. Topical: desired effect is local. Drug is applied directly where its action is desired I. Enteral: I. by mouth (orally): many drugs such as tablets, capsules, liquids Widely used, convenient Some capsules and tablets contain sustained-release drugs, which dissolve over an extended period of time. Administration of oral drugs is relatively easy for patients who are alert and can swallow (can not be used in unconscious patients). Certain drugs are given by the sublingual (placed under the tongue) route. These drugs must not be swallowed or chewed and must be dissolved completely before the patient eats or drinks. Nitroglycerin is commonly given sublingually. II. by gastric feeding tube: many drugs and for enteral nutrition III. Rectally: various drugs in suppository or enema form The effect of digestive enzymes is avoided Useful for unconscious patients and in vomiting cases Routes of Administration, Classification II. Parenteral: The most common routes of parenteral drug administration are the intravenous (IV), intramuscular (IM), the subcutaneous (SC) and intradermal routes. Rapid response obtained Useful in emergencies, vomiting and unconsciousness The drug should be in a sterile dosage form III. Topical: epicutaneous (application onto the skin), e.g. allergy testing, antifungal creams inhalational, e.g. asthma medications enema, e.g. contrast media for imaging of the bowel eye drops (onto the conjunctiva), e.g. antibiotics for conjunctivitis ear drops - such as antibiotics and corticosteroids for otitis externa intranasal route (into the nose), e.g. decongestant nasal sprays vaginal, e.g. vaginal antifungal creams 1- Absorption It is the process of entry of drug from site of administration into systemic circulation. Factors influencing absorption A- Factors related to drug a) Physicochemical properties: 1-Degree of ionization: highly ionized drugs are poorly absorbed. 2-Degree of solubility: High lipid/water partition coefficient increases absorption. 3-Chemical nature: inorganic iron is better absorbed than organic iron. 4-Valency: ferrous salts are more absorbed than ferric, -so vitamin C increases absorption of iron. b) Pharmaceutical form of drug: Absorption of solutions is better than suspensions or tablets. 1- Absorption B- Factors related to the patient: 1-Route of administration: absorption is faster from i.v. > inhaled > i.m. > oral > dermal administration seconds minutes hours 2-Area and vascularity of absorbing surface: absorption is directly proportional to both area and vascularity. Thus absorption of the drug across the intestine is more efficient than across the stomach, as intestine has more blood flow and much bigger surface area than those of the stomach 3-State of absorbing surface: e.g. atrophic gastritis and mal-absorption syndrome decrease rate of absorption of drugs. 4-Rate of general circulation: e.g., in shock, peripheral circulation is reduced and I.V. route is used. 5-Specific factors and presence of other drugs: e.g. intrinsic factor of the stomach is essential for vitamin B12 absorption from lower ileum and adrenaline induces vasoconstriction so delay absorption of local anesthetics. Bioavailability It is the percentage of drug that reaches systemic circulation in an unchanged form and becomes available for biological effect following administration by any route. It is 100% after IV administration. It is calculated by comparison of the area under the plasma concentration time curve (AUC) after IV dose of a drug with that observed when the same dose is given by another route e.g. oral. Area under the curve (AUC) oral x 100 Oral bioavailability = Area under the curve (AUC) I.V. Oral bioavailability depends on amount absorbed and amount metabolized before reaching systemic circulation (first pass metabolism) 2-Distribution Distribution: Movement of drug from the central compartment (blood) to peripheral compartments (tissues) where the drug is present. Distribution of a drug from systemic circulation to tissues is dependent on lipid solubility , ionization, molecular size , binding to plasma proteins , rate of blood flow and special barriers The body compartments include extracellular (plasma, interstitial) and intracellular which are separated by capillary wall and cell membrane The major compartments are: —plasma (5% of body weight) —interstitial fluid (16%) —intracellular fluid (35%) —transcellular fluid (2%) —fat (20%) 2-Distribution Selective distribution: Some drugs have special affinity for specific tissue. e.g. calcium in bones, iodide in thyroid gland and tetracycline in bone and teeth. Volume of Distribution: The volume of distribution (Vd) , also known as apparent volume of distribution, is a pharmacological term used to quantify the distribution of a medication between plasma and the rest of the body after oral or parenteral dosing. Vd, is defined as the volume of fluid required to contain the total amount, Q, of drug in the body at the same concentration as that present in the plasma, Cp. Vd is not a real volume, small volume indicates extensive plasma protein binding, but large volume indicates extensive tissue binding Vd is increased by increased tissue binding, decreased plasma binding and increased lipid solubility Drugs in vascular space Drugs are present in blood in: 1. Free form: active, diffusible, available for biotransformation and excretion. 2. Bound form (mainly to albumin): inert, non-diffusible, not available for metabolism and excretion. It acts as a reservoir for drug. Binding to plasma proteins is reversible Significance of binding to plasma proteins: * Two drugs may have affinity for plasma protein binding sites, thus compete with each other leading to drug interactions * An example: Phenylbutazone and salicylates can displace warfarin (oral anticoagulant) and oral hypoglycemics from plasma proteins * Drugs highly bound to plasma proteins are in general expected to persist in body longer than those less bound and are expected to have lower therapeutic activity, less efficient distribution and less available for dialysis in poisoning 3-Biotransformation (Metabolism) The conversion of a substance from one form to another by the actions of organisms or enzymes. Phases of biotransformation: Phase I (non-synthetic) reactions: introduction or unmasking of functional group by oxidation, reduction or hydrolysis. These reactions may result in : 1. 2. 3. 4. Drug inactivation (most of drugs) Conversion of inactive drug into active metabolite (cortisone→ cortisol) Conversion of active drug into active metabolite (phenacetin→ paracetamol) Conversion to toxic metabolite (methanol → formaldehyde) Phase II (Synthetic) reactions: Functional group or metabolite formed by phase I is masked by conjugation with natural endogenous constituent as glucuronic acid, glutathione, sulphate, acetic acid, glycine or methyl group. These reactions usually result in drug inactivation with few exceptions e.g. morphine-6conjugate is active Most of drugs pass through phase I only or phase II only or phase I then phase II. Some drugs as isoniazid passes first through phase II then phase I (acetylated then hydrolyzed to isonicotinic acid). 3-Biotransformation (Metabolism) Sites of biotransformation and types of enzymes 1. Microsomal enzymes: they are present in smooth endoplasmic reticulum of cells especially liver Microsomal enzymes catalyze: -Glucuronide conjugation -Oxidation by microsomal cytochrome P450 enzymes (CYP450) -Hydroxylation -Dealkylation -Reduction -Hydrolysis They are affected by drugs and age 2. Non-microsomal enzymes: present in liver, kidney, plasma, skin and GIT…etc They catalyze: -Conjugations rather than glucuronic acid -Oxidation by soluble enzymes in cytosol or mitochondria of cells e.g. MAO (monoamine oxidase) and alcohol dehydrogenase -Reduction -Hydrolysis Their activity is stable throughout life. 3-Biotransformation (Metabolism) Factors affecting drug metabolism 1-Drugs: They can stimulate (induce) or inhibit microsomal metabolizing enzymes. * Enzyme induction: Some drugs increase the synthesis or decrease degradation of enzymes. Examples: testosterone, phenobarbitone, phenytoin, carbamazepine, rifampicin, some glucocorticoids, tobacco smoking, ethyl alcohol (chronic) Importance of enzyme induction: a) It decreases effect of other drugs b) Tolerance is sometimes explained by a drug inducing its own metabolism, e.g. ethyl alcohol, phenobarbitone c) It is a mechanism of adaptation to environmental pollutants (pollutants induce their own metabolism reducing their toxic effects) * Enzyme inhibition (drugs that inhibit drug metabolism): it occurs faster than enzyme induction and causes serious drug interactions. Examples: oestrogen, progesterone, cimetidine, chloramphenicol, erythromycin, sodium valproate, cotrimoxazole, ketoconazole and ciprofloxacin 2.Genetic variation: The most important factor is genetically determined polymorphisms. Example: Isoniazid is metabolized in the liver via acetylation. There are two forms (slow and fast) of the enzyme responsible for acetylation (N-acetyl transferase), thus some patients metabolize the drug quicker than others 3-Biotransformation (Metabolism) 3. Nutritional state: Conjugating agents are sensitive to body nutrient level. For example, low protein diet can decrease glycine. 4. Dosage: High dose can saturate metabolic enzyme leading to drug accumulation. 5. Age: Drug metabolism is reduced in extremes of age (old patients and infants). 6. Gender: testosterone induces CYP450, whereas estrogen inhibits it. 7. Disease state: -Liver disease decreases the ability to metabolize drugs. -In cases of heart failure and shock, reduced hepatic flow will increase the effect of rapidly metabolized drugs whose hepatic clearance is blood flow dependent e.g. lidocaine, morphine, propranolol, verapamil…. -Kidney disease reduces the excretion of drugs. 8. Route of administration: 1st pass effect occurs for drugs administered orally 4- Excretion of drugs It is the process by which a drug or metabolite is eliminated from the body Routes of excretion 1- Renal Excretion: It is the result of three processes: Passive glomerular filtration, active tubular secretion in proximal tubules and passive tubular re-absorption. Factors affecting renal excretion: 1-Glomerular filtration rate. Only free unbound water soluble drugs with low molecular weight are filtered. 2-Change in urinary pH affects excretion of weak acid and base drugs. Thus: *Alkalinization of urine by NaHCO3 increases excretion of acidic drugs e.g. aspirin *Acidification of urine by NH4CL or vitamin C increases excretion of base drugs e.g. amphetamine 3-Active tubular secretion e.g., probenecid, penicillin, …... 4- Excretion of drugs 2-Gastrointestinal Tract: a. Salivary glands: e.g., iodides, rifampicin b. Stomach: e.g., morphine c. Large intestine: e.g., tetracycline, streptomycin d. Liver through bile, e.g.: -Ampicillin and rifampicin are excreted in active form so can be used in biliary infection and ampicillin in typhoid carriers 3-Sweat: e.g., rifampicin, vitamin B1. 4-Lungs: e.g., gases and volatile anesthetics. 5-Milk: basic drugs are trapped and excreted in acidic milk, e.g., morphine, amphetamine Also many other drugs e.g. chloramphenicol, oral anticoagulants and phenolphthalein can be excreted in milk