Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
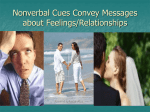
Illness Behavior & Dr - Pt Relationship Illness Behavior • 20% of the patients neglect their illness I am a patient I am weak I need help Causes of Denial of Illness It is not easy for the patient to show his weakness Doctor’s authority Illness Behavior Factors Affecting Illness Behavior Gender Symptom presentation Age Lay beliefs Race Social Class Learned behavior Previous experience Accessibility to health services Trigger factors Locus of control Factors Affecting Illness Behavior Symptoms : • severity of the symptom • Patient ideas & understanding about the symptom • Patient previous experience with this symptom Factors Affecting Illness Behavior Accessibility to Medical services Physical barriers can make health facilities difficult to reach H Factors Affecting Illness Behavior Previous experience with health services ??? Bureaucratic barrier can make health services difficult to obtain H Illness Behavior Learned behavior Somatic complain Somatic fixation Inappropriate reaction (Pt. Family & Dr.) Trigger Factors Another Interpersonal Crisis Trigger Factors Effect of the Problem on Pt. Activity Trigger Factors Pressure from Family or Friends Trigger Factors The setting of arbitrary deadline or putting limit Illness Behavior Final Message & Conclusions Doctors need to understand illness behavior for proper understanding of their patients Doctors need to explore & acknowledge patient’s believes & worries Communication Skills Communication Skills Objectives: To improve your skills in exploring and acknowledgement of patient’s thoughts and feelings. To increase your awareness about your patients’ verbal and nonverbal cues. To help you to develop new communication skills in order to deal with your patients’ cues. Exercise 4 • Write down three words that best describe the way you want to be perceived by your patients: 1)……… 2) ………… 3)………. • Write how can you use your communication skills to convey this message? 1) …………….......... 2) …………….......... 2) …………….......... Awareness of Patients’ verbal and Nonverbal Cues Who is the patient?! Classification of Communication Skills Verbal communications Nonverbal communications Communication Skills Verbal communications • How to formulate questions • Discussion , explanation & Advice • Understanding pt. verbal cues Verbal communications How to formulate questions • Direct Qs (Yes or No) • Suggestive Qs • Why Qs • Many Qs at a time • Indirect Qs (Open-ended Qs) Communication Skills Nonverbal communications 1 - Body language & Facial expression 2 - Appearance 3 - Touch 4 - Paralanguage 5 - Body bubble 6 - Environment Verbal communication for tilling information , but nonverbal communication for negotiation • Verbal communication • 10% of communications • nonverbal communication • 90% of communications Reference: (McCaskey 1979 )Rakel Nonverbal Communication is an universal language Mind & Body Body Language Facial Expression Appearance Body Language Hand to face Expression Body Language Hand Expression Body Language Hand Expression Body Language Body Posture Body Posture Body Language Touch The effect of touch Communications Paralanguage • • • • • Velocity Volume Tone Pause Others Body Language Body Bubble ???? Body Bubble Intimate zone 15 - 46 cm Private zone 46 cm - 1.2 m zone Social 1.2 m - 3.6 m Public zone More then 3.6 Communications Environment Dr. Pt. Couch Communications Environment Communications Environment Discuss the advantage of this style of communications ??? Doctor - Patient Relationship Doctor - Patient Relationship Doctors - Patient Relationship Why doctors need to have a positive relationship with their pt. ??? How dose this relationship start & how it progress ??? What are the skill needed to build a positive relationship ??? Doctors - Patient Relationship Why ??? • For the patient care & satisfaction • For doctor satisfaction • For effective use of resources Doctors - Patient Relationship Doctors - Patient Relationship Patient positive role Doctors - Patient Relationship How ??? • Professional relationship • personal relationship • Intimate relationship To Establish & To Maintain Dr-Pt Relationship • Welcoming the Patient • Showing respect To Establish & To Maintain Dr-Pt Relationship The ability to listen “ Don’t waste my time , just say yes or no” Doctor - Patient Relationship Understanding & Empathy Review of Consultation Models Hospital Model of Consultation Computerized chick lest of history taking A case of 2 weeks headache Complete history, physical Examination & Investigations ?! Psychosocial component of the physical problems . Byrne & Long 1976 Patient Centered Consultation Doctor Centered Consultation Use of pt’s knowledge and experience Use of doctor’s special skills and knowledge Silence Clarification Analyzing Listening Interpretation Probing Reflection Gathering Information The Real Reason for Consultation Failure to explore the real reason of patient problem is the main reason of consultation failure (Byrne & Long 1976) The Expanded Model of Consultation Management of Presenting Problem Modification of Help Seeking Behavior Management of Continuous Problem Opportunistic health Promotion (Stott & Davis 1979) Modification of Help Seeking Behavior • The child as the presenting complain • Frequent attender • Somatic patient Modification of Help Seeking Behavior • Sick Role • Secondary gain Modification of Help Seeking Behavior • Denial • Poor Compliance Modification of Help Seeking Behavior • Hidden agenda • Displacement Pendleton 7 Tasks 1. To define the real reasons for pt attendance 2. To consider other problems 3. To choose with the pt. appropriate action for each problem 4. To achieve a share understanding 5. To involve pt. in the management 6. To use time & resources effectively 7. To establish & maintain Dr.-pt. relationship Patient’s Ideas : Patient’s Concern : Patient’s Expectation Explanation Skills Needed To Explore the Real Reasons for Pt. Attendance • Open ended questions • Confrontation • Indirect questions • Reflection • Use of silence • Probing • Recognition of pt cues • Summarization • Immediate response to pt. cues Pendleton Third Task With the patient to choose an appropriate action for each problem. Why With the patient to choose an appropriate action for each problem • Patient responsibility • Patient compliance Pendleton Fourth Task With the patient to achieve shared understanding of the problem Doctor Patient Knowledge Questions Doubts Theories Experience Knowledge Questions Doubts Theories Experience Pendleton Fourth Task With the patient to reach Shared Understanding of the Problem The patient has the right to know all important details Pendleton Fifth Task To involve patient in the management Pendleton Sixth Task To use time & resources appropriately Pendleton Seventh Task To Establish & Maintain Dr.-Pt. Relationship Final Message & Conclusions • A lot of practice is needed to be able adopt the proper consultation model