Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
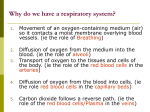
Provide anatomy and physiology advice to clients Gaseous exchange and breathing Lung macro structure • In our last session we looked at the respiratory system histology. In this session we are going to look closely at how oxygen from our lungs enters our blood. But before we come to that lets revise briefly the macro structure of our lungs. Note in this slide that the left lung has a notch it. This allows the heart to snuggle in because the heart’s apex is not in the medial plane. The lobes are separated into segments • From the diagram you can see that in each lobe there are quite distinct branches of the bronchial tree that align to segments. There are 10 segments in the lung and each is served by their own artery and vein. Each segment is separated by connective tissue and this makes it easier to dissect out diseased components. Look at the bronchial tree in this slide. Here each segment has been painted in different colours so that you can see them easily. Mechanics of breathing • When we breathe in, the muscles in our diaphragm contract and move inferiorly (i.e. move downwards). At the same time, the external intercostal muscles lift the rib cage and pull the sternum forward. These two actions expand the volume of the thoracic space by about 500ml and the lung tissue can expand by that amount. So air can rush in to fill the volume. During exercise when deep breathing is required, several other muscles that include the scalenes and the sternocleidomastoid muscles raise the rib cage even further to permit more air to enter. When we breathe out the reverse occurs. Blood vessels • Deoxygenated blood travels from the left ventricle of the heart through the pulmonary artery to the lungs, where it is delivered to a fine network of capillaries. These capillaries surround each alveoli. Remember, that alveoli are composed of squamous epithelial cells held together by threads of smooth muscle. You can visualise this in this slide. We have about 8 million alveoli in our lungs. Lung structure revision • The alveoli walls are very, thin single layers of squamous epithelial cells. These are called Type 1 cells. In amongst these cells are cuboidal cells which are called Type 2 cells. These produce a surfactant which covers the surface of Type 1 cells and this reduces surface tension. This is very important because water molecules tend to stick to each other and gas molecules, like oxygen, would have difficulty moving across the membrane if it was not for the surfactant. Type 3 cells or macrophages can also been seen wandering around looking for bacteria and viruses to devour. Gas Exchange • Oxygen readily diffuses from the lung across the respiratory membrane (composed largely of squamous epithelial cells) into the capillary network. It diffuses across because the pressure of oxygen is less in the capillaries than in the lung. The oxygen readily combines with haemoglobin in the red blood cells. Each red blood cell can carry about 250 oxygen molecules. Carbon dioxide from metabolism diffuses out of the plasma into the lungs, where it is expelled when a person breathes out. Control of respiration • Fortunately, we don’t have to sit and think about our breathing. It just happens most of the time. That is easy to say but the control mechanisms are quite complex and is still the matter of extensive research. • A portion of the brain is known as the inspiratory centre. The neurons there fire regular bursts of impulses that travel along the phrenic and intercostal nerves to excite the diaphragm and the external intercostal muscles. These contract and air rushes into the lungs. When lactic acid builds up from anaerobic exercise or where hypoxia occurs for any reason then the neurons generate a gasping or puffing response. Respiratory rhythm • We all breath on a regular rhythm but the regulation for that rhythm is obscure. It has been proposed that pacemaker neurons control our breathing rate whilst others have proposed that stretch receptors in the lungs feedback to the brain. None of these explain why we breathe slowly when asleep or why our breathing speeds up when we think about something exciting like studying anatomy and physiology. We do know that our breathing rate is related to our emotional state and that the limbic part of the brain has a role to play in this, so perhaps that part of the brain is involved in deep regulation of breathing rhythm. Some clinical conditions • The trachea and bronchus have smooth muscle bands around the tubes and these can contract if histamine is present in the blood. Histamine is present as a response to inflammation such as a cold virus or an allergy; hay fever or asthma. The effect is to tighten up the air ways and this constricts the amount of oxygen that can enter and carbon dioxide that can leave. When people take an antihistamine, they are opening up the airway by reducing the effects of histamine. When asthmatics inhale their reliever puffer are also doing the same thing. Activity • Prepare a presentation aimed at high school students to describe how oxygen from the air makes its way into the lungs.