Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Management of acute coronary syndrome wikipedia , lookup
Cardiac surgery wikipedia , lookup
Coronary artery disease wikipedia , lookup
Jatene procedure wikipedia , lookup
Myocardial infarction wikipedia , lookup
Antihypertensive drug wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
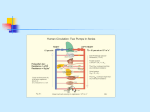
Specific circulatory systemregulation of the heart and vessel activities Romana Šlamberová, MD PhD Department of Normal, Pathological and Clinical Physiology Introduction Slides from the lecture. Respecting the copyrights it was not possible to publish pictures showed at the lecture at our website. © 2006, Romana Slamberova, MD PhD Distribution of blood circulation Total volume of blood in all vessels (intravascular volume): man: 5.4 l (77 ml / kg) woman: 4.5 l (65 ml / kg) Distribution: Heart 7% Pulmonary circulation 9% Systemic circulation 84% from that veins 75% large arteries 15% small arteries 3% capilaries: 7% Resistance of blood circulation Total peripheral resistance: of all paralel restistance in the body Actual resistance is given based on the lumen of vessels and viscosity of blood Percentage portion of resistance in different types of vessels: large arteries 19% small arteries 47% capillaries 27% veins 7% Resistance depends not only on type of vessel, but also on the actual situation of blood need in organs Regulation of blood circulation Mechanisms of regulation: Local Humoral (chemical) – O2, CO2, H+ Nervous Enzymatic and hormonal General Fast = short-term (regulate blood pressure) Slow = long-term (regulate blood volume) – several days Local chemical regulatory mechanisms The most obvious in the heart and the brain Goal: autonomic regulation of resistance by organ based on its metabolic needs Principal: accumulation of products of metabolism (CO2, H+, lactacid ) or consumption of substances necessary for proper function (O2) directly affects smooth muscles of vessels and induce vasodilatation Local nervous regulatory mechanisms The most obvious in the skin and mucous Goal: central regulation of blood distribution Principal: Autonomic nervous system Sympaticus Vasoconstriction – activation of α receptors in vesselsnoradrenalin (glands, GIT, skin, mucous, kidneys, other inner organs) Vasodilatation – activation of β receptors in vessels – adrenalin (heart, brain, skeletal muscles) Parasympaticus - Acetylcholin Vasoconstriction – heart Vasodilatation – salivatory glands, GIT, external genitals Local enzymatic and hormonal regulatory mechanisms Kinin ↑ = vasodilatation Cells of GIT glands contain kallikrein – changes kininogen to kinin → kallidin → bradykinin (vasodilatation) Kinins are any of various structurally related polypeptides, such as bradykinin and kallikrein, that act locally to induce vasodilation and contraction of smooth muscle. A role in inflammation, blood pressure control, coagulation and pain. Hormones of adrenal medula: adrenalin (vasodilatation), noradrenalin (vasoconstriction) General fast (short-term) regulatory mechanisms (1) Nervous autonomic reflexes Baroreflex glomus caroticum, glomus aorticum Afferentation: IX and X spinal nerve Centre: medulla oblongata, nucleus tractus solitarii Efferentation: X spinal nerve, sympatetic fibres Effector: heart (atriums), vessels Effect: After acute increase of blood pressure – activation of receptors – decrease of blood pressure (vasodilatation, decrease of effect of sympaticus) General fast (short-term) regulatory mechanisms (2) Receptors in the heart Reflex of atrial receptors – mechano- and volumoreceptors – activated by increased blood flow through the heart A receptors – sensitive to ↑ of wall tension after systole of atriums B receptors – sensitive to ↑ of wall tension after systole of ventricles Ventricular receptors – mechano- and chemical receptors activated in pathological cases Hypoxia of myocardium → decrease of heart rate (Bezold-Jarisch reflex) → protection of myocardium of larger damage General fast (short-term) regulatory mechanisms (3) Humoral mechanisms Adrenalin – β receptors → vasodilatation → ↓ peripheral resistance → blood from skin and GIT to skeletal muscles, heart and brain → ↑ minute heart volume Noradrenalin – α receptors → vasoconstriction → ↑ blood pressure Renin-angiotensin – activated by ↓ pressure in vas afferens General slow (long-term) regulatory mechanisms Regulatory mechanisms of water and electrolytes exchanges Regulation of total blood volume by kidneys Increase of ADH (vasopressin) When ↑ blood pressure → ↑ of filtration pressure in glomeruli → ↑ production of urine → ↓ volume of circulating blood → ↓ blood pressure ↑ ADH → ↑ of the permeability of collecting ductus for the water → water is reabsorbed → ↑ volume of circulating blood → ↑ blood pressure Increase of Aldosterone ↑ aldosterone → ↑ reabsorbtion Na+ and water → ↓ volume of urine → ↑ volume of circulating blood → ↑ blood pressure Intracardial regulatory mechanisms (1) Frank-Starling’s law = initial length of the fibers is determined by the degree of diastolic filling of the heart, and the pressure developed in the ventricle is proportionate to the total tension developed. The developed tension increases as the diastolic volume increases until it reaches a maximum, then tends to decrease. Ganong: Review of Medical Physiology Intracardial regulatory mechanisms (2) Ionotropic effect of heart rhythm ↑ heart frequency → ↑ amount of Ca2+ that goes into heart cells → ↑ Ca2+ available for tubules of sarkoplasmatic reticulum → ↑ Ca2+ that is freed by each contraction → ↑ strength of contraction Extracardial regulatory mechanisms Cardiomotoric centers Inhibition – ncl. Ambiguus (beginning of n. vagus in medulla oblongata) Excitation - Th1-3 beginning of sympathetic fibres Vasomotoric centers In brain stem (medulla oblongata, Pons Varoli) In the hypothalamus (controls activity of vasomotoric centers in brain stem) Brain cortex – control both the hypothalamus and the brain stem Stunning Postischemic stunning - paralyzed myocardium Short-time ischemia of cardiac muscle provokes defects of contraction of cardiac muscle. Reversible dysfunction of contraction. Persists also after reperfusion of ischemic myocardium, cardiac cells were not permanently damaged and coronary flow was totally renewed. There is no necrosis. There is: defect of calcium homoeostasis – antagonistic effect of calcium ameliorates reparation of conctractions after ischemic stress - : reduces transfer of calcium to the cells just during ischemia lower reduction of ATP reducing of volume of lesion reducing of reperfusionallesion. increasing of free oxygene radicals increased transfer of extracellular Ca++ to the cells (always pathology!!) antioxidants reduce (N-Acetylcystein, Oxypurinol) Hibernation Hibernating myocardium some hours persisting defect of contraction function reduced coronary flow living cardiac cells Adaptive response to low flow, hypoxia does not induces cellular death and metabolism and clinical symptom s of ischemia. After revival of coronary flow the function is regenerating. Stunning x Hibernation x Si1ent ischemia Coronary flow normal or almost normal significantly reduced Differential diagnosis To measure contraction function and regional blood flow.