Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
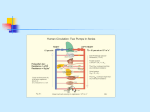
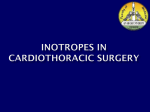
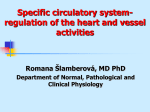
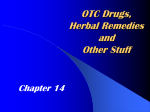
Inotropes and fluids Dr Cath Spoors Consultant, Anaesthesia and Burns Intensive Care Broomfield Hospital, Chelmsford • • • • • • Fluids and fluid challenges Why use drugs to affect the CVS? Definitions Receptors Drugs Practice points, pearls and pitfalls Fluids • Primarily affect preload • Optimising preload will have a positive inotropic effect • Blood also affects oxygen carrying capacity • Blood products will affect coagulation • Hypovolaemia may be absolute or relative Preload Spotting hypovolaemia Spotting hypovolaemia Spotting hypovolaemia Fluid overload Fluid challenge Fluid challenge • Step change in intravascular volume / venous return • Choose your parameter – – – – CVP SVV FTc SV • 250ml is reasonable (consider less if prone to cardiac failure/overload). Consider a straight-leg raise • Record pre-challenge, immediately after, then after 10-15 min • The aim is a sustained improvement • Transient usually indicates room for further fluid • No improvement – either patient is “full” or the hypovolaemia is very severe. • Consider other pathologies (e.g. tamponade, PE) Inotropes Why use drugs to affect the CVS? • Improve the flow – The amount of blood delivered • Improve pressure – To allow delivery of oxygen and substrates • Improve distribution – To defend vital organs Why use drugs to affect the CVS? • Improve the flow – The amount of blood delivered • Improve pressure – To allow delivery of oxygen and substrates • Improve distribution – To defend vital organs Optimise the circulation without over-stressing it • • • • • • Inotrope Chronotrope Lusitrope Vasopressor Agonist Antagonist • • • • • • Inotrope – increases force of contraction Chronotrope Lusitrope Vasopressor Agonist Antagonist • • • • • • Inotrope – increases force of contraction Chronotrope – increases heart rate Lusitrope Vasopressor Agonist Antagonist • • • • • • Inotrope – increases force of contraction Chronotrope – increases heart rate Lusitrope – increases rate of cardiac relaxation Vasopressor Agonist Antagonist • • • • • • Inotrope – increases force of contraction Chronotrope – increases heart rate Lusitrope – increases rate of cardiac relaxation Vasopressor – constricts blood vessels Agonist Antagonist • • • • • • Inotrope – increases force of contraction Chronotrope – increases heart rate Lusitrope – increases rate of cardiac relaxation Vasopressor – constricts blood vessels Agonist – activates a receptor Anatgonist • • • • • • Inotrope – increases force of contraction Chronotrope – increases heart rate Lusitrope – increases rate of cardiac relaxation Vasopressor – constricts blood vessels Agonist – activates a receptor Antagonist – opposes a receptor “Squeeze harder!” - Inotrope “Send the air to the bag!” - Vasopressor “Pump faster!” - Chronotrope “Let go in between!” - Lusitrope Receptor Site Effect α1 adrenergic Vascular smooth muscle Liver Vasoconstriction Glycogenolysis; potassium release α2 adrenergic CNS: pre-synaptic Inhibit noradrenaline release: negative feedback loop causing sedation, vasodilatation, muscle relaxation β1 adrenergic Myocardium Increased heart rate and contractility β2 adrenergic Vascular smooth muscle Vasodilatation (peripheral and renal circulation) Dopaminergic D1 – renal, coronary, mesenteric D2 – nerve endings Vasodilatation Effects are dose-dependent V1 (vascular) Vascular smooth muscle Cardiac myocytes Platelets Efferent glomerular arterioles Vasoconstriction - coronary and cerebral sparing Other sites of drug action • Direct intracellular (phosphodiesterase inhibitors, levosimendan, calcium) • Guanylate cyclase (methylene blue – blocks nitric oxide-induced vasodilatation) • Inhibition of inflammation (steroids) Decisions, decisions... – – – – – – – – – – – – – – Noradrenaline Adrenaline Dopamine Dobutamine Dopexamine Milrinone Enoximone Levosimendan Metaraminol Vasopressin Terlipressin Methylene blue Corticosteroid Calcium Noradrenaline • Endogenous catecholamine • Secreted as a hormone from the adrenal medulla • Released from sympathetic nerve endings -spills over into circulation during mass sympathetic stimulation • Acts on α1 adrenergic and β1 adrenergic receptors • Vasoconstriction – increased SVRI and re-distribution of blood flow to heart, brain, and skeletal muscle • Inotropy; theoretically chronotropy but offset by reflex bradycardia due to α1 effect • Increased mean arterial pressure (MAP) • Increased myocardial oxygen demand • May distribute blood flow away from skin, splanchnic circulation, and renal circulation – e.g. if used before correction of hypovolaemia Metaraminol • • • • • Predominantly acts at α1 receptors Vasoconstrictor action Reflex bradycardia can be marked Can be given in small IV boluses Often used in anaesthesia to counteract vasodilatation (e.g. from spinal or epidural) • Can be used as a bridge to a noradrenaline infusion Adrenaline • • • • • • • • • • • • Endogenous catecholamine Main hormone secreted from adrenal medulla Sympathetic neurotransmitter Acts non-selectively on all adrenergic receptors Chronotropic and inotropic Vasoconstriction – re-distribution of blood flow to heart, brain, and skeletal muscle Used during CPR Bronchodilator (used in status asthmaticus) Drug of choice in anaphylaxis Increases myocardial oxygen demand May cause lactic acidosis May cause hyperglycaemia Dopamine • • • • Endogenous catecholamine Precursor of noradrenaline and adrenaline Acts at dopaminergic, β1 and α1 receptors Actions are dose-dependent: low doses (0.53mcg/kg/min) cause coronary, renal, mesenteric, and cerebral vasodilatation via D1 and D2 receptors; intermediate doses (3-10mcg/kg/min cause β1mediated inotropy, chronotropy, and some increase in SVR; and high doses (>10mcg/kg/min) cause α1 effects i.e. vasoconstriction • “Renal” dose controversial • Inhibits peristalsis – may cause ileus Dobutamine • • • • Synthetic catecholamine Strong β-agonist (β1 and β2) – “inodilator” Potent inotrope β2 effects cause vasodilatation but α1 effect predominate at higher doses • Significant increase in oxygen consumption (dobutamine stress test) • Can cause ventricular arrhythmias • Tolerance can be an issue Comparative receptor actions of catecholamines Dopexamine • Synthetic catecholamine • β2 agonist. Also active at D1 and D2 receptors; and inhibits neuronal catecholamine uptake • Vasodilation which can be profound • Mild positive inotropy/chronotropy • Reduces afterload via generalised vasodilatation but can cause hypotension Phosphodiesterase inhibitors • Milrinone/enoximone • Increase calcium availability within the myocyte and therefore the force of contraction • Also enhance calcium return to sarcoplasmic reticulum, enhancing cardiac relaxation (lusitropy) • Cause vasodilatation due to effects in vascular smooth muscle • Heart rate minimally affected • Do not significantly increase myocardial oxygen consumption • Useful in acute right ventricular failure due to dilatory effects on pulmonary arteries (reduces right ventricular afterload) • Can cause significant hypotension in hypovolaemic patients • Vasopressors may be required in addition Levosimendan • Calcium sensitiser – enhances the molecular mechanics of muscle contraction • Binds to cardiac troponin C • Positive inotropy without increasing myocardial oxygen consumption • Vasodilatory in pulmonary circulation – offloads the right ventricle • Does not increase intracellular calcium – less arrhythmogenic than PDEIs Vasopressin • Acts on peripheral vasopressin receptors • Effects are preserved during hypoxia and severe acidosis • Greatest effects in gut, muscle, and skin • May be dilatory to pulmonary, coronary, and cerebral circulation (but high doses may cause cardiac ischaemia) • Increases free water resorption in kidney (can cause hyponatraemia) • Increases cortisol secretion by stimulating ACTH release from pituitary Methylene Blue • Inhibits guanylyl cyclase, preventing nitric oxide-induced vasodilatation • May improve outcomes in vasoplegic syndrome after cardiopulmonary bypass • Effects in other pathologies not well-studied – use is empirical generally • Interferes with sats probe! Weaning inotropes • The inotropes will wean when the patient gets better – not the other way around • Wean the most harmful ones first (adrenaline) • Wean when MAP exceeds target by around 5mmHg • There is no shame in not being able to wean • Weaning inotropes seems more difficult at night • Keep assessing fluid balance: inotropes are NOT a contraindication to diuretics if the patient is fluid overloaded • Don’t use pain or distress as inotropes!