Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Saturated fat and cardiovascular disease wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
History of invasive and interventional cardiology wikipedia , lookup
Cardiovascular disease wikipedia , lookup
Heart failure wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Electrocardiography wikipedia , lookup
Rheumatic fever wikipedia , lookup
Cardiothoracic surgery wikipedia , lookup
Aortic stenosis wikipedia , lookup
Hypertrophic cardiomyopathy wikipedia , lookup
Mitral insufficiency wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Myocardial infarction wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
Lutembacher's syndrome wikipedia , lookup
Coronary artery disease wikipedia , lookup
Atrial septal defect wikipedia , lookup
Congenital heart defect wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
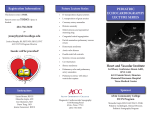
Congenital Heart Disease and Cardiac Imaging Modalities Riya Chacko, MD May 2008 Overview Classification of congenital heart disease Brief overview of common simple adult congenital heart diseases: ASD, VSD, PDA, and coarctation Transthoracic echocardiography Fetal echocardiography Transesophageal echocardiography 3D echocardiography Cardiac CT Cardiac MRI Relevance Congenital heart disease is the most common major birth defect affecting 6-8/1000 live births (Gardiner) Accounts for 40% of perinatal deaths from congenital anomalies, 20% of deaths in 1st month of life, and majority of congenital defect deaths in childhood (Randall) With improved surgical and medical therapies, now more adults live with congenital heart disease. In 1950s, 20% of congenital heart disease patients lived to adulthood and now 80%. (Crean) Adult population in US with congenital heart disease now 1 million (Russell) Table 1. Survival Rate from Year of Birth (1940-2000) by Complexity of Congenital Heart Disease Russell, I. A. et al. Anesth Analg 2006;102:694-723 Copyright restrictions apply. Classification of Congenital Heart Diseases Simple or complex Simple includes ASD, VSD, or singular valvular abnormalities (Ebstein’s anomaly) Complex includes those with multiple defects, AV canal defects, or “single” ventricle physiology. Cyanotic or non-cyanotic Non-cyanotic: ASD, VSD, sinus venosus defect, patent ductus arteriosus, aortic stenosis, pulmonary stenosis, aortic coarctation Cyanotic: Tetralogy of Fallot, Ebstein’s anomaly, transposition of the great arteries, Eisenmenger’s syndrome, truncus arteriosus, tricuspid atresia, total anomalous pulmonary venous return “5 Ts and 2 Es” The heart is formed and septations occur at 50 embryonic days. Atrial Septal Defects One third of all congenital defects detected in the adult are ASDs. 2-3 times more likely to occur in women 3 varieties: Ostium primum Ostium secundum Sinus venosus Ostium Primum 15% of all ASDs Occurs in the lower part of the atrial septum Associated with a left axis deviation on EKG Also associated with cleft in anterior mitral valve leaflet Ostium Secundum Defect in fossa ovalis Represents 75% of all ASDs Associated with mitral valve prolapse Sinus Venosus Defect Located in the upper atrial septum Represents 10% of all ASD defects Associated with anomalous pulmonary venous drainage into the right atrium or venae cavae Patent Ductus Arteriosus PDA 10% of congenital heart disease Rarely closes spontaneously after infancy May become aneurysmal or calcified leading to rupture 1/3 of patients die of heart failure, pulmonary hypertension or endarteritis by age 40. 2/3 die by age 60. Aortic Coarctation Usually distal to left subclavian at site of ligamentum arteriosum. 2-5 times more common in men Associated with Turner’s syndrome, bicuspid aortic valve, ventricular septal defect, patent ductus arteriosus, mitral stenosis or regurgitation, or aneurysms of the circle of Willis Imaging Protocols for Congenital Heart Disease Position of the cardiac apex and aortic arch• Levocardia Left-sided cardiac apex• Dextrocardia Right-sided cardiac apex• Mesocardia Midline/indistinct cardiac apex Aortic arch Left or right aortic arch, branches Defining Atria and Ventricles Left atrium– by finger-like appendage Right atrium – larger, wider appendage Usually concordance with abdominal situs 7080% (IVC on right, RA on right) Right ventricle – triangular with 3 components (inlet, trabeculated, outlet). Moderator band, septal attachments of TV Left ventricle – elliptical, fine trabeculae, no septal attachment of MV (inlet, tension apparatus, and outlet zone for AV valve) Situs of the atrium Situs solitus Normal atrial arrangement Situs inversus Reverse atrial arrangement (LA–RV, RA–LV) Situs ambiguous Often LA isomerism (usual with abnormal venous drainage from azygous/hemi-azygous veins) Atrioventricular (AV) arrangement AV concordance RA–RV, LA–LV AV discordance RA–LV, LA–RV Double inlet RA and LA to LV or RV Absent Right or left AV valve atresia Ventriculoarterial (VA) arrangement VA concordance RV–PA, LV–aorta VA discordance RV–aorta, LV–PA Double outlet RV or LV giving off both PA and aorta Solitary or common arterial trunk Truncus or A–P window Ventricular morphology Normal Single ventricle physiology Rudimentary Other defects ASD VSD AVSD Common in Trisomy 21 (Down's syndrome) Valvular defects, atresia, abnormal number of cusps Shunts Blalock–Taussig or Glenn shunts• Venous drainage Anomalous systemic or pulmonary venous connections Vascular rings Nicol ED. Clin Rad 2007;62(6 Coronary anatomy Normal configuration Rotation discordance Aberrant origin Single coronary artery Malignant course Abnormal morphology Normal or congenital heart Rotation common in AV and VA i.e., RCA off left coronary sinus Beware left main coronary artery atresia i.e., between RVOT and aorta i.e., Kawasaki's disease Echocardiography Preferred method for initial assessment of congenital heart disease Also the preferred imaging modality in babies Limitations – Chest wall deformities, median sternotomies, relation to extracardiac structures and post-surgical assessment Poor assessment of RV size and function Fetal Echocardiography Two forms: basic and extended “Four chamber view” the most basic Color-flow and spectral Doppler imaging M-mode available Sensitivity from 60-100% Limited by body habitus and fetal age (11 to 14 weeks transvaginal ultrasound). 16 weeks by abdominal. Reported specificity up to 100% in babies without congenital heart disease Transabdominal view of the 4 chambers of the heart at 13 weeks' gestation. Transvaginal view of atrioventricular septal defect at 13 weeks' gestation in a fetus with trisomy 21 (case 2). (A) A full examination of the fetal heart may be obtained by five transverse sections through the abdomen and chest of the fetus. The first section shows abdominal situs (B) with the aorta (Ao) to the left of the spine and the inferior caval vein (IVC) anterior and to the right. The normal fetal stomach (St) and heart lie on the left side. The second section (C) illustrates the four chambers of the heart with the left atrium (LA) in front of the spine and the right ventricle (RV) just below the sternum. The third cut (D) shows the aorta arising centrally in the heart from the left ventricle (LV) and the fourth the pulmonary trunk (PV) arising from the anteriorly placed right ventricle and crossing to the fetal left over the ascending aorta (E). The fifth section shows the anteriorly positioned ductal arch (D) and the transverse aortic arch (Ao) to be of equal size traversing back to the fetal spine (F). A normal variant "three vessel" view is shown with a right sided aortic arch and persistent left superior caval vein (LSVC). The trachea (T) can be seen lying between the aortic (Ao) and ductal (D) arches (G). Gardiner. Transvaginal 3-vessel view of the great arteries at 13 weeks' gestation. PA, Main pulmonary artery; Ao, aorta; SVC, superior vena cava; BPA, right branch pulmonary artery. McAuliffe F. In 1992, only 8% of infants with congenital heart disease undergoing cardiac surgery had a prenatal diagnosis. With fetal echo, this number rose to 57% in 2002.(Mohan) In one study assessing use of early fetal echo (prior to 14 weeks gestation) in a high-risk population, sensitivity of 70% and specificity of 98% This resulted in 79% of patients terminating their pregnancy prior to their 18-20 week follow up. Transesophageal Echocardiography Good for evaluation of venous return, atria, AV valves, and the left ventricular outflow tract Mid-esophageal (ME) four-chamber and bicaval views good for atrial septum by 2D ME 4-chamber and transgastric mid-short axis to assess for VSDs Also essential in intra-operative repair Limited for evaluation of the right ventricular outflow tract and pulmonary arteries Preferred method in the following cases: ASD, secundum Mitral valve regurgitation Ebstein’s anomaly Fontan – assessing for right atrial thrombus, obstruction Coronary sinus defect Inferior sinus venosus defect Superior sinus venosus defect AV septal defect 3D Echocardiography In a small, non-randomized comparison of 3D echo evaluation of congenital abnormalities as compared to anatomical specimens, Vogel et al. found a close association. The key difference is in thickness of supporting structures (overestimated on 3D echo). Salustri et al reported additional information gathered by 3D versus 2D echo on 36% of patients screened with known congenital heart disease. Advantage of being able to view en face both sides of a septal defect versus 2D echo --Live 3D imaging examples of how 3D imaging is better than 2D imaging for evaluating structures such as septal defects Houck, R. C. et al. Am. J. Roentgenol. 2006;187:1092-1106 Copyright © 2006 by the American Roentgen Ray Society --Live 3D imaging examples of how 3D imaging is better than 2D imaging for evaluating structures such as septal defects Houck, R. C. et al. Am. J. Roentgenol. 2006;187:1092-1106 Copyright © 2006 by the American Roentgen Ray Society Cardiac CT 10% of MDCT patients at Royal Brompton Hospital in London have congenital heart disease. Multi-detector CT scans (MDCT) are able to identify those with congenital heart disease and anomalous coronary arteries. In a retrospective review of 85 patients with congenital heart disease at Ohio State University, authors Cook and Raman was found that 19% had detectable anomalous coronary anatomy by MDCT both 16 and 64 slice. Normal coronary arteries Figure 6 Anomalous LCA arising from a common RCA origin and coursing anterior to the RVOT (arrow). Note the vestigial left anterior descending artery (LAD) (arrowhead). Manghat, N E et al. Heart 2005;91:1515-1522 Copyright ©2005 BMJ Publishing Group Ltd. Pacemaker leads extending through ASD to left atrium and terminating in left ventricle. Kawasaki’s disease Ebstein’s Anomaly with distal displacement of the right AV valves compared to the left AV valves Patent ductus arteriosus Angiography with pigtail catheter (A). (B) MRA. (C) CT after stent showing contained aortic rupture. (D) CT showing resolution of pseudoaneurysm. (E) MRA showing drop out with stent. Transposition of the great vessels Not as useful due to poorer image quality if the patient has frequent beat-to-beat variation or atrial fibrillation. Flow data is not available and thus information on physiologic effects of valvular abnormalities. Inadequate assessment of RV function Regional wall motion as compared to TTE may be inferior due to lower temporal resolution. Radiation exposure should be considered as compared to cardiac MR or TTE especially if repeat examinations are required throughout a lifetime. Cardiac CT Advantages over cardiac MRI include: Shorter breath-hold sequences that may not be tolerated in a congenital heart disease population Better tolerability for those with pacemakers/ICDs or those with claustrophobia More robust coronary artery imaging especially when involvement of fistulous communication Rapid image acquisition time Cardiac MRI 1st described to assess congenital heart disease in 1984. Also utilizes contrast-enhanced MR angiography (CE-MRA) Allows better visualization of mediastinal vessels (small central pulmonary arteries) and better to assess the left pulmonary artery than echo. Best to visualize proximal and mid pulmonary arterial stenosis but not distal to the hila. (A and B) ALCAPA syndrome (anomalous left coronary artery from PA). (C) Large RCA with fistulous connection. CT at bottom (E) shows anomalous LCX draining into coronary sinus Crean. Heart 2007. Pulmonary vein stenosis seen on MRI Favored to evaluate coarctation in children. Accurately measures pulmonary blood flow and assesses the aorta. Ultrasound better to assess valvular pathology but MR better to assess systemic and venous malformations. Because of wider field of view, better to assess larger cardiac chambers (ie Ebstein’s anomaly) May also be used to estimate left-to-right shunts by measuring flow to calculate Qp:Qs Probably most effective to assess post-surgically as well Allows better assessment of RV size and function (critical in cases such as Tetralogy of Fallot post-surgery). With delayed enhancement technique, it is useful to assess prognosis in congenital heart disease as well. Disadvantage compared to cardiac catheterization: inability to measure pressures and obtain O2 saturations Examination time is long (up to 90 minutes) which is difficult in a pediatric population. Faster heart rates in infant population make MRI less helpful and accurate. Images are obscured by metallic stents in those with stent-corrected coarctation Components of a congenital CMR exam Axial steady state free precession (SSFP) cine sequence from aortic arch to diaphragm 10 mm thick, no gap Short axis oblique SSFP from ventricular apex to atrioventricular (AV) groove, 8 mm thick, no gap Fast cine phase contrast through ascending aorta, main and left and right pulmonary arteries Three dimensional contrast enhanced magnetic resonance angiography (CE-MRA): coronal plane, sternum to spine, slice thickness 2–2.5 mm, arterial and venous phase Additional thin slices (SSFP or black blood) and cine phase contrast studies (for example, for flow through shunts, collaterals, anomalous veins or arteries, etc) as directed by monitoring physician Multiplanar reformations, maximum intensity projections and volume rendered image preparation (ideally by reporting physician) Creon A. Summary Classification of congenital heart disease Overview of common adult congenital heart diseases: ASD, VSD, PDA, and coarctation Transthoracic echocardiography Fetal echocardiography Transesophageal echocardiography 3D echocardiography Cardiac CT Cardiac MRI Regardless of imaging modality, one requires the expertise of an experienced specialist… References Bedard E et al. Adult congenital heart disease: a 2008 review. Brit Med Bull 2008;85:151-180. Brickner ME et al. Congenital Heart Disease in Adults:First of Two Parts. NEJM Jan 27, 2000;342(4):256-263. Cook SC, Raman SV. Unique application of multislice computed tomography in adults with congenital heart disease. Inter J of Card 2007;119(1):101-106. Creon A. Cardiovascular MR and CT in Congenital Heart Disease. Heart 2007;93:1637-1647. Fellows KE et al. Evaluation of Congenital Heart Disease with MR Imaging: Current and Coming Attractions. AJR 159:925-931. Gardiner HM. Fetal echocardiography:20 years of progress. Heart. 2001 Dec;86 Suppl 2:II12-22. Higgins CB, Caputo GR. Role of MR Imaging in Acquired and Congenital Cardiovascular Disease. AJR 1993;161:13-22. Houck RC et al. Live 3D echocardiography: a replacement for traditional 2D echocardiography? AJR Am J Roentgenol. 2006 Oct;187(4):1092-106 McAuliffe FM et al. Am J Obstet Gynecol. 2005 Sep;193(3 Pt 2):1253-9. Mohan UR et al. Am J Cardiol. 2005 Jul 1;96(1):134-6. Nicol ED et al. Assessment of adult congenital heart disease with multi-detector computed tomography – beyond coronary lumenography. Clin Rad 2007;62(6):518-527. Randall P et al. Accuracy of fetal echocardiography in the routine detection of congenital heart disease among unselected and low risk populations: a systematic review. BJOG 2005;112:24-30. Russell IA et al. Congenital heart disease in the adult: a review with internet-accessible transesophageal echocardiographic images. Anesth Analg. 2006 Mar;102(3):694-723. Sahn DJ, Vick III GW. Review of new techniques in echocardiography and magnetic resonance imaging as applied to patients with congenital heart disease. Heart 2001;86(Suppl II):ii41-ii53. Vogel M et al. Comparison of three dimensional echocardiographic findings with anatomical specimens of various congenitally malformed hearts. Heart 1995;73:566-570. Zipes DP et al. Braunwald’s Heart Disease. 7th edition. Elsevier 2005.1489-1547.