Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
History of invasive and interventional cardiology wikipedia , lookup
Saturated fat and cardiovascular disease wikipedia , lookup
Drug-eluting stent wikipedia , lookup
Antihypertensive drug wikipedia , lookup
Cardiovascular disease wikipedia , lookup
Cardiothoracic surgery wikipedia , lookup
Jatene procedure wikipedia , lookup
Cardiac surgery wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
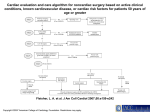
CARDIAC RISK ASSESSMENT FOR NONCARDIAC SURGERY JOHN HAMATY D.O. SOUTH JERSEY HEART GROUP SJHG.ORG INTRODUCTION: CAD ACCOUNTS FOR THE MOST DEATHS IN PTS UNDERGOING NONCARDIAC SURGERY. 5% OF ELDERLY POPULATION IN US UNDERGO NONCARDIAC SURGERY/YR. 30% ARE AT RISK FOR CAD WITH INHOSPITAL COMPLICATIONS IN 1.5 MIL. PTS. PERIOPERATIVE RISK OF EVENTS PATIENTS WITH NO PRIOR HISTORY OF MYOCARDIAL INFARCTION HAVE A LOW RISK OF PERIOPERATIVE MI(0.1%-0.6%) PATIENTS WITH A HISTORY OF PRIOR MI ARE AT A SIGNIFICANTLY HIGHER RISK (2.8%-7%). PERIOPERATIVE RISK OF EVENTS (HISTORY OF PRIOR MI) MI WITHIN 3 MOS.-37% INCREASE IN EVENTS MI WITHIN 3-6MOS.-16% INCREASE IN EVENTS MI GREATER THAN 6 MOS.-4% INCREASE IN EVENTS A STEPWISE APPROACH FOR PERIOPERATIVE RISK ASSESSMENT OF A PATIENT UNDERGOING NONCARDIAC SURGERY URGENCY OF SURGERY ALL PATIENTS UNDERGOING URGENT SURGERY SHOULD BE BETA-BLOCKED TO A HEART RATE OF 50 BEATS/MIN AND A BLOOD PRESSURE THAT IS CONTROLLED. PRIOR REVASCULARIZATION PTS WHO HAVE UNDERGONE COMPLETE REVASCULARIZATION IN THE FORM OF CORONARY ARTERY BYPASS OR PTCA WITHIN 6 MONTHS TO 5 YEARS AND ARE FUNCTIONALLY ACTIVE AND HAVE NO CLINICAL EVIDENCE OF ISCHEMIA DO NOT NEED FURTHER CARDIAC TESTING. PRIOR EVALUATION FOR CAD PTS. THAT HAVE BEEN EVALUATED IN THE PAST TWO YEARS WITH EITHER INVASIVE OR NONINVASIVE TECHNIQUES WITH FAVORALE FINDINGS GENERALLY DO NOT NEED FURTHER EVALUATION. MUST BE FREE OF CARDIAC SYMPTOMS AND OR SIGNS OF ISCHEMIA PRESENCE OF CLINICAL RISK FACTORS HISTORY, PHYSICAL AND ECG ARE GENERALLY SUFFICIENT TO ESTIMATE CARDIAC RISK ASSESSMENT OF CLINICAL RISK FUNCTIONAL CAPACITY PREDICTORS OF INCREASED PERIOPERATIVE CV RISK • • • • MAJOR UNSTABLE ANGINA RECENT MYOCARDIAL INFARCTION(>7 BUT <30 DAYS DECOMPENSATED CHF SYMPTOMATIC ARRHYTHMIAS(RAPID VENTRICULAR RESPONSES.) PREDICTORS OF INCREASED PERIOPERATIVE CV RISK INTERMEDIATE • • • • MILD ANGINA PRIOR MYOCARDIAL INFARCCTION COMPENSATED OR PRIOR CHF DIABETES MELLITUS PREDICTORS OF INCREASED PERIOPERATIVE CV RISK MINOR • ADVANCED AGE • ABNORMAL ECG(LVH, LBBB) • RHYTHM OTHER THAN SINUS(CONTROLLED) • LOW FUNCTIONAL CAPACITY • HISTORY OF CVA • UNCONTROLLED HYPERTENSION SURGERY SPECIFIC CARDIAC RISK HIGH(CARDIAC RISK>5%) • EMERGENT MAJOR OPERATION • AORTIC AND OTHER MAJOR VASCULAR • PERIPHERAL VASCULAR • ANTICIPATED PROLONGED PROCEDURE SURGERY SPECIFIC CARDIAC RISK INTERMEDIAC(CARDIAC RISK<5%) • CAROTID ENDARTERECTOMY • HEAD AND NECK • INTRAPERITONEAL AND INTRATHORACIC • ORTHOPEDIC • PROSTATE SURGERY SPECIFIC CARDIAC RISK LOW(CARDIAC RISK<1%) • • • • ENDOSCOPIC PROCEDURES SUPERFICIAL PROCEDURES CATARACT BREAST FUNCTIONAL CAPACITY FUNCTIONAL CAPACITY EXCELLENT(ACTIVITIES>7METS) • CARRY 24 LBS UP 8 STEPS • CARRY OBJECTS THAT WEIGH 80 LBS. • RECREATION(SKI, BASKETBALL, WALK 5MPH) FUNCTIONAL CAPACITY MODERATE(ACTIVITIES >4 BUT <7 METS) • HAVE SEXUAL INTERCOURSE WITHOUT STOPPING • WALK 4 MPH ON LEVEL GROUND • OUTDOOR WORK(GARDEN, RAKE, WEEK) • RECREATION(DANCE, SWIM) FUNCTIONAL CAPACITY POOR (ACTIVITY <4 METS) • • • • SHOWER/DRESS WITHOUT STOPPING WALK 2.5 MPH ON LEVEL GROUND OUTDOOR WORK(CLEAN WINDOWS) RECREATION(PLAY GOLF, BOWL) FUNCTIONAL CAPACITY IS ONE OF THE MOST USEFUL MEASURES OF PREOPERATIVE RISK Stepwise Approach to Preoperative Cardiac Assessment 1. Need for noncardiac surgery 2. Coronary No Urgent or revascularization Elective within 5 years ? 3. Recent coronary evaluation No Yes Emergency Operating Room Recurrent symptoms or signs ? Yes No Favorable AND no change in symptoms Postoperative risk stratification and risk factor management Yes 4. Clinical predictors Recent coronary angiogram or Unfavorable stress test ? OR change in symptoms Stepwise Approach to Preoperative Cardiac Assessment 4. Clinical predictors 5. Major clinical predictor Unstable coronary syndromes Decompensated congestive heart failure Significant arrhythmia Severe valvular disease 6. Intermediate clinical predictor Mild angina pectoris Prior myocardial infarction Compensated or prior CHF Diabetes mellitus 7. Minor or no clinical predictor Advanced age Abnormal ECG Rhythm other than sinus Low functional capacity History of stroke Uncontrolled systemic hypertension Stepwise Approach to Preoperative Cardiac Assessment Major Clinical Predictor 5. Major clinical predictor Consider delay or cancel noncardiac surgery Consider coronary angiography Medical management and risk factor modification Subsequent care dictated by findings and treatment results Unstable coronary syndromes Decompensated congestive heart failure Significant arrhythmia Severe valvular disease Stepwise Approach to Preoperative Cardiac Assessment Functional capacity Surgical risk Poor (<4 METs) Noninvasive testing Invasive testing 8. Noninvasive testing High risk Low risk 6. Intermediate clinical predictor Moderate or excellent (>4 METs) High surgical risk procedure Intermediate or low surgical risk procedure Low surgical risk procedure Operating room Consider coronary angiography Postoperative risk stratification and risk factor reduction Subsequent care dictated by findings and treatment results Stepwise Approach to Preoperative Cardiac Assessment Functional capacity Surgical risk Poor (<4 METs) High surgical risk procedure Noninvasive testing Invasive testing 8. Noninvasive testing High risk Low risk 7. Minor or no clinical predictor Intermediate or low surgical risk procedure Moderate or excellent (>4 METs) Low surgical risk procedure Operating room Consider coronary angiography Postoperative risk stratification and risk factor reduction Subsequent care dictated by findings and treatment results IN THE ABSENCE OF CONTRAINDICATIONS, BETA BLOCKADE THERAPY SHOULD BE GIVEN TO ALL PATIENTS AT HIGH RISK FOR CORONARY EVENTS(DIABETICS) TREATMENT SHOULD BE GIVEN SEVERAL DAYS OR WEEKS PRIOR TO OR AT DOSES TO ACHIEVE HR 50 AND BP OF 100mm hg.