Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Metalloprotease inhibitor wikipedia , lookup
Discovery and development of ACE inhibitors wikipedia , lookup
Discovery and development of tubulin inhibitors wikipedia , lookup
Drug design wikipedia , lookup
Discovery and development of non-nucleoside reverse-transcriptase inhibitors wikipedia , lookup
Discovery and development of proton pump inhibitors wikipedia , lookup
Discovery and development of neuraminidase inhibitors wikipedia , lookup
Discovery and development of integrase inhibitors wikipedia , lookup
Pharmaceutical industry wikipedia , lookup
Psychopharmacology wikipedia , lookup
Pharmacognosy wikipedia , lookup
Drug discovery wikipedia , lookup
Theralizumab wikipedia , lookup
Prescription costs wikipedia , lookup
Pharmacogenomics wikipedia , lookup
Prescription drug prices in the United States wikipedia , lookup
Pharmacokinetics wikipedia , lookup
Drug interaction wikipedia , lookup
Neuropharmacology wikipedia , lookup
Neuropsychopharmacology wikipedia , lookup
Discovery and development of cephalosporins wikipedia , lookup
Reading assignments:
Katzung’s Basic & Clinical Pharmacology,
13th Edi ,Ch-43 ,p769-787;
LEARNING OBJECTIVES
A. Inhibitors of cell wall synthesis (ICWS)
•
Understand the structure and function of the bacterial
cell wall
•
Know the multiple sites of inhibition by antibacterial
agents
•
1. Penicillins
•
•
•
•
•
•
•
Structure-function relationships-- the beta-lactam ring
Role of penicillin binding proteins (PBP) and murein hydrolases
Chemotherapeutic spectrum of penicillins
Mechanisms of resistance — beta-lactamases
Cross-resistance
Acid- and beta-lactamase-resistant penicillins
Adverse reactions — hypersensitivity
2. Cephalosporins
• Similarities to and differences from penicillins
• Changes in pharmacokinetics and chemotherapeutic
spectrum of first-, second-, third-, and fourth-generation
cephalosporins
3. Other beta-lactams
• a. Aztreonam
b. Carbapenems
c. Beta-lactamse Inhibitors
4. Other ICWS
• a. Vancomycin
b. Bacitracin
c. Isoniazid (only for M. tuberculosis)
• d. Fosfomycin
• Know sites of inhibition of cell wall synthesis
• Know clinical use
Penicillin has common ending with “cillin”
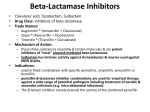
Inhibitors of Cell Wall Synthesis
(ICWS)
• Cell wall is unique target
in pathogen
• Essential for pathogen
• β-Lactam antibiotics
and vancomycin block
enzymatic steps outside
of the cell or in the
periplasmic space
• Other ICWS act at
intracellular sites
1 = fosfomycin; 2 = cycloserine; 3 = bacitracin; 4 = vancomycin; 5 = β-lactams
Bacterial cell wall synthesis inhibitors
2
1
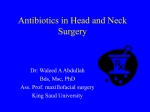
Mechanism of Action of b-lactams- by inhibition
of transpeptidase and preventing the
remodeling of the peptidoglycan layer
3
Gm-ve
Gm+ve
Mechanism of action of vancomycin by
inhibition of peptidoglycan layer biosynthesis
• Name the antibiotics which interfere with the
formation peptide side chains between adjacent
strands of PG by inhibiting B-Lactam binding
proteins(also called PBP)?
---1,2,3,4
• Name the antibiotic/s which substitute d-alanine
for d-lactate in the synthesis of PG precursors?
• Name the antibiotic/s that block the transport of
PG precursors across cell membrane?
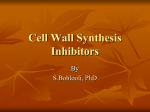
Beta-lactam Antibiotics
Anti-staphylcoccal penicillins
Biliary secretion
Antipseudomnal penicillins
Ampicillin or
Amoxicillin rash
• Find out B-Lactam ring
• Show the site of action of penicillinase (B-lactamase)
• How structural change makes a drug penicillinase
resistant ?
• What are the possible drawbacks associated with
penicillinase resistant strains?
Penicillins
•
Very selective toxicity (extremely high
chemotherapeutic index)
•
Bactericidal in growing, proliferating cells
•
Primarily used for gram positive microbes
X
Mechanism of Action
1)
Covalent binding to transpeptidases/penicillin binding proteins
(PBPs),all are enzymes-
2)
Inhibition of transpeptidation reaction (Cross-linking of cell
wall)
3)
Activation of murein hydrolases (autolysins)
Penicillin Pharmacokinetics
Start with ‘KEY INFORMATION’ as
-all Penicillins are water soluble (memorize the exceptions like Ampicillin,oxacillin
& Nafcillin)
-figure out what key pharmacokinetic attributes a drug should have depending
upon its solubility
Absorption
•
Oral-- Many penicillins are acid-sensitive, yet some are still given orally
•
Other penicillins are acid-stable (phenoxypenicillin V [PEN-V] , oxacillin, amoxicillin,
carbenicillin indanyl)
•
Parenteral--IV, IM
2 long-acting parenteral forms-
Benzathine Pen. G is hydrolyzed slowly over a period of several weeks and
provides low plasma concentrations . Given in every 2-4 weeks in Prophylaxis of
Rheumatic fever
Procaine Pen. G (usually combined with small dose of local anaesthetic) is
hydrolyzed more rapidly and produces significant plasma concentrations for about 24
hrs.
Distribution: Penicillins are widely
distributed to organs and tissues except
the CNS.
When the meninges are inflammed, penicillins readily
penetrate the CSF and may be given intravenously
for the treatment of meningitis.
Elimination: Most penicillins are eliminated
primarily by active renal tubular
secretion , except ampicillin & Nafcillin
Renal tubular excretion is inhibited by
Probenecid.
• A 72 yrs. Old female with HT & congestive heart disease
was adequately treated with multiple drugs for her
condition. She has been recently prescribed an antibiotic
for her lower respiratory tract infection.Following 4th day
of antibiotic therapy she developed severe pain, swelling
& tenderness in her left great toe.Her physician is
suspecting this condition linked with the prescribed
antibiotic. Which of the following antibiotic was
prescribed?
Classification*,Spectrum and Indications of
Penicillins
•
Classified according to their antimicrobial spectrum of activity + Sensitivity to BLactamase .
1.Narrow-spectrum Penicillinase/B-lactamase sensitive- Pen- G & Pen-V
Spectrum: Strepto,Pneumo,Meningo, T.Pallidum
2.Very Narrow spectrum Penicillinase/B-lactamase resistant
Dicloxacillin,Nafcillin,Methicillin
Spectrum: Effective ONLY against B-Lactamase producing Staph EXCEPT MRSA.
3.Extended-spectrum Penicillinase/B-lactamase sensitive3a.Aminopenicillin- Amoxicillin, Ampicillin
Spectrum:
-Gram +ve: Streptococci (BUT not Staph)
-Gram –ive: E. coli, H. influenzae, and Proteus, Listeria monocytogenes
(Ampicillin),Borrelia Burgdorferi (Amoxycillin), H.Pylori (Amoxycillin) species.
3b.Antipseudomonal- Piperacillin,Ticarcillin, Azlocillin, Carbenicillin
Spectrum: Gm –VE rods inclusing pseudomonas aeruginosa
‘5’
‘5’
Sexually Transmitted Diseases
-Vignettes
• Painless sore on penis/around • Painless sore on penis/vagina,
dysuria , urethral discharge of
vagina with inguinal bubo, h/o
yellow pus , gram stain of
unprotected sexual contact,
exudate reveals gram negative
dark-field exam positive
diplococci with PMNs…..DOC
…………………………..DOC?
& other drugs?
• Frequent, painful, or burning
urination in men and women
as well as vaginal discharge
with characteristic fishy odor,
genital soreness, redness, or
itching in women….DOC &
other drugs?
• Painful, watery skin blisters on
or around the genitals or anus
+/- around lips….DOC & other
drugs?
Sample Vignette: A critically ill patient with systemic
infection was brought to ER. He has some clinico-pathomicrobiology data….make a diagnosis & then treat the
patient with empiric therapy.
•
Various Gram positive
or gram negative cocci
or bacilli (aerobes /
anaerobes) or fungi or
virus causing meningitis
,encephalitis,septicemia
,pneumonia,endocarditi
s,osteomyelitis or other
serious types of
systemic infections.
•
A 55 yr old man presents with shaking
chills, fever, myalgia and tachypnea with
wheezing since last few hours. He has
chronic obstructive pulmonary disease and
a history of anaphylactic reactions to
penicillin G. Evaluation of renal function
show normal .Blood cultures are positive
for gram positive cocci in grape like
clusters. Which of the following would be
the
treatment
for has
this been
patient?
A 56best
yr old
male who
on immunosuppressant therapy following kidney
transplant was brought to ED with a feeling
of malaise ,chills and high grade fever .The
drug of choice for empiric treatment of this
patient would be
Extended Spectrum Penicillins (both) shows synergism with
-Beta Lactamase Inhibitors
-Aminoglycosides
1.Amoxicillin-clavulanate
(Augmentin)
2.Ampicillin-sulbactam
(Unsayn)
3.Piperacillin-tazobactam
(Zosyn)
4.Ticarcillin-clavulanate
(Timentin)
1.Ampicillin-Gentamycin
(Ampiclox)
2.Amoxycillin-Gentamycin
(Amclox)
Amoxycillin + Clavalunic acid
Piperacillin + Tazobactam
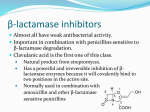
Beta-Lactamase Inhibitors
Clavulanate ,Sulbactam & Tazobactam
All are inhibitors of class II to class VI -lactamases. βlactamases (e.g. gonococci, strept, E.coli, H.
influenzae can be inhibited); not effective against
inducible chromosomal enzymes (e.g. Pseudomonas,
Enterobacter)
When used alone, they do not show any antibacterial
activity. Must be used in combination with Penicillins
(extended spectrum).
In combination, a -lactamase inhibitor acts as a suicide
inhibitor of -lactamase enzymes by serving as a
surrogate substrate for these enzymes.
• Drug X (B-Lactamase Inhibitor) when
combined with Drug Y(Extended spectrum
Penicillin),efficacy of drug Y was increased
. What is the cause for this?
Adverse Effects of Penicillins
Allergies
– Can cause All 4 types of H/S
Ampicillin & amoxicillin rash
– About 10% incidence, 90% for mononucleosis patients
– Self-limiting, often does not recur
– Probably not an immunological mechanism
Hypersensitivity Reaction
–
–
–
–
–
–
–
–
Major penicillin adverse effect
About 5-8% claim allergies to penicillins (I –IV)
Cross-reactivity with all beta-lactams; except aztreonam
Not dependent on therapeutic dose
Rapid onset
Can occur without prior known exposure
Some success with skin test screening
Hapten= major antigenic determinant = Benzylpencililloic acid
– Neutropenia(Nafcillin),Intestitial nephritis(Methicillin,Nafcillin).
Differentiating feature between renal failure
caused by Nafcillin (Interstitial nephritis) & other
nephrotoxic drugs would be Eosinophilia ,thus
would also include some allergic manifestations
-Amphotericin B
-Aminoglycosides
-Vancomycin
(when combined
with AG)
-Cephalosporins
(lower gen.,when
combined with
other nephrotoxic
drugs)
Adverse Effects of Penicillins
Seizures induced by high dose penicillins (particularly in
renal failure)
-Toxic effects from Na+ or K+ overload not due to drug but
due to its additive salts in their preparation in patients
with cardiovascular or renal disease.
-Jarisch Herxheimer Reaction in treatment of
Syphillis→lysis of spirochetes→release of endotoxin in
blood→fever ,chills ,headache,myalgia & exacerbation of
syphilitic lesions.
GI upset due to change in bacterial flora (mainly with broad
spectrum ones)
Resistance to Penicillins
1.
No cell wall, no activation of murein hydrolases, metabolically
inactive
2.
Change in Porin structure-only in gm-ves .Drug access denied
3.
Inaccessible PBPs (MRSA) to one group of B lactam confers
resistance against all B lactam group containing drugs→Hence
to be treated with no B lactam ICWS (ex. Vancomycin) or some
other drugs.
4.
β-Lactamase production (MOST COMMON MECH.)
– Major mechanism of resistance
– Plasmid-mediated
– Use β-lactamase-resistant penicillins (Nafcillin, oxacillin,
dicloxacillin)
– Co-administer β-lactamase inhibitor (Clavulanic acid,
Sulbactam, Tazobactam)
•
Only used with extended spectrum penicillins
Problems Associated with
Penicillin Use/Overuse
•
Sensitization
– Leads to allergies
•
Selection for resistant strains
(90% of Staph are resistant)
•
Superinfections by resistant strains (Esp.
proteus, pseudomonas, serratia, fungi)
2. Cephalosporins
1st
generation
2nd
generation
3rd
generation
4th
generation
CEFADROXIL
CEPHALOTIN
CEPHALEXIN
CEFAZOLIN
CEPHAPIRIN
CEPHRADINE
CEFOXITIN
CEFACLOR
CEFAMANDOL
E
CEFUROXIME
LORCARBEF
CEFONICID
CEFOTETAN
CEFTRIAXONE
CEFTAZIMIDE
MOXALACTAM
CEFOTAXIME
CEFPODOXIM CEFEPIME
E
CEFTIZOXIME
CEFOPERAZO
NE
5th
generation
CEFTAROLINE
(MRSA)
Cephalosporins
• Structure , MOA & MOR similar to penicillins
• Broader spectrum of activity
• Poor oral absorption for many cephalosporins
• More toxic than penicillins-- particularly renal
• Some cross-reactivity with penicillin-sensitive patients
• More expensive than penicillins
• Cephalosporins often are secondary ICWS-if a penicillin
will work, then use it
Cephalosporins
• Cephalosporins traditionally classed as 1st, 2nd, 3rd, and 4th
generation
• Chronology of development and use
• Much variation within generation, but generally:
– Greater gram negative activity
– Some with less gram positive activity (in 2nd and 3rd generation)
– Cephalosporinase-resistant (especially 4th generation-cefepime)
– Less toxic to patient
– Better distribution (especially to CNS)
Try to figure out pharmacokinetic &
pharmacodynamic characteristics of
various generations of cephalosporin by
using 2 physico-chemical information of
a drug ,as size & lipid solubility
Cephalosporins: Uses 1
• First-generation [cefazolin (parenteral); cephalexin (oral)]
– Cephalothin, the prototype first-generation cephalosporin,
is no longer available in the United States.
– Cefazolin (long t1/2) has good activity against grampositive bacteria (not MRSA)and modest activity against
gram-negative bacteria (E.Coli,Klebsiella pneumoniae and
some proteus species).
• Cellulitis (staphylococcus, streptococcus)
• Drug of choice for surgical prophylaxis except abdominal >>>
than use cefoxitin
None enters CNS
Cephalosporins: Uses 2
• Second-generation (cefaclor (oral), cefoxitin,
cefotetan, cefuroxime, cefamandole)
– Increased activity against gram-negative bacteria (E.
coli, Klebsiella, Proteus, Haemophilus influenzae,
Moraxella catarrhalis)
– Cefoxitin & Cefotetan has additional activity against
anaerobes (Drug of choice for surgical prophylaxis in
abdominal surgery.)
• Pelvic inflammatory disease, diverticulitis.
• Pneumonia, bronchitis (H. influenzae)
None enters CNS except Cefuroxime
Cephalosporins: Uses 3
• Third-generation (ceftriaxone, cefotaxime, ceftazidime,
cefoperazone, ceftizoxime, cefexime (oral))
– Decreased activity against gram-positive bacteria but increased
activity against gram-negative bacteria (Enterobacter, Serratia)
– Activity against Pseudomonas aeruginosa in a subset of drugs
(ceftazidime, cefoperazone)
– Meningitis (Neisseria gonorrhoeae)
– Community-acquired pneumonia, Lyme disease,osteomyelitis
(ceftazidime)
– Gonorrhea: ceftriaxone (parenteral) or cefixime (oral) are drugs
of choice
– Many third-generation cephalosporins that penetrate into the CNS (ax drugs) are useful in empirical treatment of meningitis →goes well
with guess organism for newborn, child, adult but not geriatric cases.
A 2-month-old boy/immunocompromised geriatric person is
brought to the ER with fever irritability and vomiting.
Lumbar puncture reveals CSF pleocytosis and you proceed
with empirical ceftriaxone therapy . You must also
administer ampicillin to cover for which bacteria particularly
in this scenario considering your patient’s age?
Cephalosporins: Uses 3
• Fourth-generation (cefepime)
– Extensive gram-positive and gram-negative activity
and increased resistance to -lactamases
– Use: Could be used to treat wide range of Gm+ve or
Gm-ve ,beta lactamase producing or non producing
organism
BUT
practically we use those in those reserve for
situations which are very life threatening or caused by
organisms that are resistant to primary line of
antibiotics e.g. such as neutropenic fever
– Enters CNS
Be appropriate for a task
• Cephalosporins are LAME on the following bugs
L- Listeria (Penicillins used)
A- Atypical Bacteria (No Cell wall i.e Chlamydia,
Mycoplasma best treated with
Macrolides/Tetracycline
M- MRSA
FQ/Vancomycin/Linezolide/Pristinamycin/Tigecill
ine)
E- Enterococcus {treated with (Penicillin +
Aminoglycoside combination) OR vancomycin)
Adverse Effects of Cephalosporins
• Local irritation from injection
• GI distress from oral dose– nausea and vomiting, diarrhea
• Renal toxicity (exception cefoperazone & ceftriaxone
→Billiary excretion) tubular necrosis, interstitial nephritis;
may be enhanced by aminoglycosides; usually don’t see
this with products available today unless used with other
nephrotoxic drugs.
• Cefuroxime,Cefotetan & cefoperazone–
– Disulfiram effect (due to ‘methylthiotetrazole’ induced
inhibition of aldehyde dehydrogenase)
– Bleeding
– Platelet disorders
Adverse Effects of Cephalosporins
• Hypersensitivity-6 - 16% cross-reactivity with penicillins
• Superinfections-- Especially with 2nd and 3rd
• generation due to low gram positive activity
3. Other beta-lactams
AZTREONAM
IMIPENEM/CILASTATIN
MEROPENEM
ERTAPENEM
CLAVULANIC ACID
TAZOBACTAM
SULBACTAM
Other β-Lactams
synergistic with aminoglycosides
Monobactams-- Aztreonam
– β-Lactamase resistant
– Only gram negative activity [gram (-) rods –
Klebsiella spp, Pseudomonas spp, Serratia spp ];
virtually no gram positive or anaerobic activity
– For pencillin allergic pts (No cross-reactivity to
penicillin allergies) and those with renal
insufficiency who cannot tolerate aminoglycosides
– Toxicity: vertigo, usually non-toxic; occasional
GI upset
Other β-Lactams
Carbapenems-- Imipenem
– Broad spectrum-- Gram positive and negative rods, and
anaerobes; DOC for Enterobacter;
– β-Lactamase resistant
– Inactivated by renal dihydropeptidase I,
– Co-administer Cilastatin
– IV only
– Pseudomonas develops resistance rapidly, use with
aminoglycosides
– Cross-sensitivity in patients with penicillin allergies
– Toxicity: CNS toxicity in high doses/plasma levels confusion,
encephalopathy & seizures .Seizure in 1 out of 2 patient treated
with this drug
– Meropenem & Ertapenem
• dipeptidase-resistant carbapenem: don’t need cilastatin, has ↓
risk of seizures
4. Other cell wall synthesis inhibitors
(Non –beta Lactam cell wall synthesis inhibitors)
VANCOMYCIN
BACITRACIN
CYCLOSERINE
FOSFOMYCIN
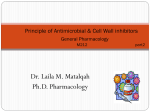
Vancomycin
Mechanism of Action: Inhibits late
stage of peptidoglycan synthesis
(transglycosylation) Slowly
bactericidal glycoprotein
Antibacterial Spectrum:
Strictly G+ve spectrum of acitivity:
-Staph aureus ( MRSA, Coagulase –
ve)
-Enterococcus
-Streptococcus (Including Penicillin
non sensitive strepto pneumonae)
-Cl. difficile
Pharmacokinetics:
• No GI absorption Always given iv
except in the t/t of C.difficile colitis
(given orally)
• Minimal CSF concentrations
• Excreted unchanged by kidneys ↓
dose in renal impairment (CR CL)
What are the drug availability to treat
MSSA(Methicillin Sensitive Staph Aureus)
,MRSA (Methicillin Resistant) & VRSA
(Vancomycin Resistant) strains ?
Name few clinical situation where a drug is
given by systemic route for a local/topical
purpose?
USES
1. Clostridium difficile-induced
pseudomembranous colitis
2. Strept endocarditis (alternative
to β-lactams in penicillin-allergic pts)
3. Serious infections with MRSA
(now intermediate resistance)
Adverse Effects:
1. Rapid iv infusion histaminerelease diffuse flushing (red man
syndrome)→Type1 H/S (?) pre t/t
with Antihistaminics helps
2. Ototoxicity, Nephrotoxicity (↑ risk
with concomitant aminoglycoside)
3. Reversible neutropenia
(w/prolonged courses)
‘6’
An unknown antibiotic was erroneously given by fast
infusion.The drug primarily Inhibits late stage of
peptidoglycan synthesis (transglycosylation) &
proven to be effective against wide range of gram
positive cocci & bacilli (no effect against gram
negatives)causing life threatening types of both
nosocomial & community acquired infections .
During administration patient developed severe
itching & erythromatous rashes in the upper trunk.
Patient also developed tinnitus & transient hearing
loss. There was a statutory warning about possible
nephrotoxicity if this drug is combined with other
nephrotoxic drugs in the drug literature . Pull out all
the key information to identify this antibiotic.
You may be punished for other’s
fault
Bacitracin
It inhibits cell wall synthesis
Used only by topical application (very nephrotoxic on systemic
use ) of minor skin and ocular
infections.
-often combined with Polymyxin or
Neomycin in ointments and
creams. ( Triple Antibiotic)
-Active against gram +ive cocci,
including Staphylococci and
Streptococci.
Cycloserine
-Very unstable at acid pH.
-Inhibits many gram +ive and gram
–ive organisms.
Almost exclusively used to treat
tuberculosis caused by strains
of M. tuberculosis resistant to
1st-line agents.*
Adverse Effects
Serious dose-related CNS
toxicity, including sedation,
headache, tremor, vertigo,
confusion, acute psychosis and
convulsions.
Fosfomycin
Fosfomycin, a newer antibiotic, inhibits
a very early stage of bacterial cell
wall synthesis.
Active against both gram +ive and gram –
ive organisms, including E. coli,
Citrobacter species, Klebsiella species,
Proteus species, and Serratia
marcescens.
Fosfomycin is specifically approved by
FDA for the treatment of
uncomplicated UTI due to E. coli or
Enterococcus faecalis in women,
and is administered orally as a single
dose (3 gm).
Fosfomycin appears to be safe during
pregnancy.
Key Characteristics of ICWS
Drugs
Clinical Use
Pharmacokinetics
Adverse Effects
β-Lactams
Penicillins
Simple penicillins
Pen G, oral or parenteral; Pen V,
oral; less acid-labile; benzathine
Pen G, depot
Hypersensitivity
Gram + cocci
Oral; oxacillin and dicloxacillin,
acid-stable; nafcillin and oxacillin,
parenteral
Methicillin not used—
nephrotoxic
Anti-Staphlococcal
S. aureus
Extended spectrum
Gram + and –
β-lactamase sensitive
Cephalosporins
First generation
Pseudomonas,
Proteus
Chemoprophylaxis,
alternative to AntiStaph penicillin
Parenteral only; usually with βlactamase inhibitor
Cephalexin, oral; cefazolin,
parenteral
Second
More gram – , less
gram +
Cefaclor (oral)
Third
More Gram -, less
gram +
Cefpodoxime proxetil oral; better
for CNS
Better distribution (CNS)
Fourth
Gram –
β-lactamase resistant; narrow
spectrum
β-lactamase sensitive; broad
spectrum
Ampicillin (inj) & Amoxicillin (oral)
Anti-Pseudomonal
Comments
β-lactamase sensitive; Combine with
aminoglycoside
Hypersensitivity;
some GI, renal;
platelet inhibition and
disulfiram effect—
cefotetan,
cefoperazone
β-lactamase sensitive
Superinfections; β-lactamase
sensitive
β-lactamase sensitive
Monobactams
Only gram -
Parenteral
No cross-reactivity
with β-lactams
β-lactamase resistant
Carbapenams
Broad spectrum
Parenteral; imipenam inactivated in
kidney
GI effects
β-lactamase resistant
Use with aminoglycoside
Non-β-Lactams
Vancomycin
Fosfomycin
MRSA
IV ; oral for GI tract
‘Red man’ , some
renal and oto-tox
Enhances nephrotox of
aminoglycosides
Gram – UTI
Active uptake by bacteria
(especially Gram -)
Well tolerated
Synergy with β-lactams,
aminoglycosides, fluoroquinolones
B. Agents Which Affect Cell Membranes
POLYMYXIN B
COLISTIMETHATE
GRAMICIDIN
Cell wall synthesis inhibitors
III
III
Penicillins
Cephalosporins
Penicillin G
Penicillin V
Nafcillin
Oxacillin
L
antistaph
III
Other beta-lactams
Other cell wall
synthesis inhibitors
Aztreonam
Imipenem/Cilastatin
Meropenem
Clavulanic Acid
Vancomycin II
Fosfomycin I
Bacitracin
II
Ampicillin
Amoxicillin
Ticarcillin
Piperacillinantipseudo
First generation
Cephalexin O
Cefazolin
Cephradine O
Second
generation
Cefoxitin
Cefaclor O
Cefotetan
Third generation
Ceftriaxone L
Ceftazidime
Cefoperazone L
Cefpodoxime
proxetil O
Fourth generation
Cefepime
A 25-year-old man with a complaint of
dysuria and urethral discharge of yellow pus
had a painless ulcer on his penis. Gram
stain of the urethral exudate revealed gramnegative diplococci with PMN’s. Which of
the following medications is a currently
recommended oral treatment for this
patient?
A.
B.
C.
D.
E.
Azithromycin
Cefexime
Ceftriaxone
Doxycycline
Ofloxacin
Answer: B
Cefexime is an oral medication
for gonococcus
Ofloxacin no longer recommended
because of resistance
Ceftriaxone, a drug of choice, is not
effective orally
Which of the following is a
recommended oral prophylactic drug, for a
62-year-old man with a mitral valve prolapse
who is allergic to penicillins, to take prior to
a dental procedure?
A.
B.
C.
D.
E.
Aztreonam
Cefaclor
Clindamycin
Levofloxacin
Tobramycin
Answer: C
Amoxicillin drug of choice; but
clindamycin or azithromycin are
good alternatives for this situation
in patients allergic to penicillins
PowerPoint Slides
Several of the PowerPoint slides are Copyright © 2002-04,
the American Society for Pharmacology and Experimental
Therapeutics (ASPET). All rights reserved.
Some of slides in this session are from the above mentioned format
and are free for use by members of ASPET.
Some others are from various sources like text book, recommended
books, slides of Dr. S. Akbar (ex. professor, Pharmacology ,MUA).
Core concepts of various USMLE High yield review series like
Kaplan ,BRS etc. are thoroughly explored & integrated whenever
necessary