Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Psychedelic therapy wikipedia , lookup
Toxicodynamics wikipedia , lookup
Pharmacokinetics wikipedia , lookup
NK1 receptor antagonist wikipedia , lookup
Pharmaceutical industry wikipedia , lookup
Effects of long-term benzodiazepine use wikipedia , lookup
Prescription costs wikipedia , lookup
Pharmacogenomics wikipedia , lookup
Pharmacognosy wikipedia , lookup
Drug interaction wikipedia , lookup
Polysubstance dependence wikipedia , lookup
Neuropharmacology wikipedia , lookup
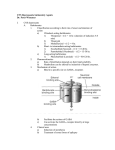
Sedative Hypnotics and anxiolytics Terminology Tranquilizers (anxiolytics): Treat excitment and anxiety Sedative-Hypnotics (sleeping pills): Sedation and sleep Sedative hypnotics are drugs used for the treatment of anxiety and sleep disorders. A sedative A hypnotic drug Sometimes calledproduces drowsiness and anxiolytic, or minor tranquilizer, encourage the reduces anxiety onset and maintenance of and exerts a sleep calming effect Anxiety disorders •Generalized anxiety disorder (GAD)= excessive anxiety lacking any clear reason •Panic disorder (sudden attacks of severe fear accompanied by sweating, tachycardia, chest pains,….) •Phobias (strong fears of snakes, open spaces, flying) •Post-traumatic stress disorder (anxiety triggered by recall of past stressful experiences) •Obsessive compulsive disorder (OCD) e.g. fear Examples drugs: of Sedative-Hypnotic 1- Benzodiazepines 2- Buspirone 3- Zolpidem 4- Barbiturates 5- Ethyl alcohol NB: BZs and barbiturates share very similar properties but BZs have a much safer pharmacological profile All have the same Mechanism of action (acting on GABA) except Buspirone Graded dose-dependent depression of the CNS function is a characteristic of sedative-hypnotics. Individual drugs differ in the relationship between the dose and the degree of CNS depression BENZODIAZEPINES Benzodiazepines (BZs) are the most widely used sedativehypnotic drugs They have replaced barbiturates for most uses, particularly for treatment of anxiety and sleep disorders How Do BZ Work? A model of the GABAA receptor-chloride ion channel The receptor consists of five or more membrane-spanning subunits. GABA interact with alpha or beta subunits triggering chloride channel opening with resultant membrane hyperpolarization. Binding of BZs to gamma subunits potentiates effects of GABA, facilitates the process of channel opening. BZs increases the frequency of channel opening by a given concentration of GABA, but no change in the mean open time Pharmacokinetics: absorption: well absorbed if given orally , Cmax reached in about 1 h strongly bound to plasma proteins distribution: high lipid solubility metabolism: hydroxylation &conjugation with glucuronic acid Pharmacological Actions The main effects of BZs are: 1- Reduction of anxiety and aggression 2Sedation & induction of sleep 3- Reduction of skeletal muscle tone and coordination 4- Anticonvulsant (antiepileptic) effect 5- Anterograde amnesia ., they obliterate memory of events experienced while under their influence Therapeutic uses 1) as anxiolytic Short-term treatment of acute anxiety states 2) for insomnia BZs decrease rapid eye movement (REM) sleep, which is associated with dreaming For short-term courses, as tolerance , dependence, hangover may occur 3) Reduction of muscle tone and coordination Increased muscle tone is a common feature of anxiety states in humans and may contribute to the aches and pains, headache The relaxant effect of BZs may therefore be clinically useful 4) As anticonvulsants Clonazepam has selective anticonvulsant action ( epilepsy) Diazepam i.v. in status epilepticus 5) Muscular disorders strong muscle-relaxing properties In cases of : - muscle spasm - spastic disorders (MS, cerebral palsy) 6) Ttreatment of alcohol withdrawal symptoms By ameliorating the alcohol withdrawal syndrome The commonly used drug is Diazepam 7) as a pre-ansthetic medication for : i) Anxiolytic effects ii) Amnesia (impair short-term memory) 7) To control extreme mania Pharmacokinetics BZS are well absorbed orally, giving a peak plasma concentration in about 1 hour They bind strongly to plasma protein, and their high lipid solubility causes many to accumulate in body fat given by mouth or i.v. (e.g. diazepam in status epilepticus, midazolam in anaesthesia) BZs are all metabolized and excreted in the urine Classificaion of BZs According to duration of action: •Very short (< 6 h): Triazolam , midazolam • Short (12-18): Lorazepam (Ativan) • Medium (24 h): Alprazolam (Xanax), • Long (24-48 h): Diazepam (Valium) The longer acting agents form active metabolites with long half-lives Classificaion of BZs • According to therapeutic uses: HypnoticTemazepam, Nitrazepam Anti-anxiety- Diazepam, Oxazepam For panic attacks; Alprazolam Anticonvulsant- Diazepam, Lorazepam, Advantages Why BZ have replaced barbiturates ?? 1- Less tolerance & physical dependence 2- They cause less disturbance in sleep patterns 3- Barbiturates causes drug interaction because they are enzyme inducers e.g. They increase metabolism of warfarin due to induction of cytochrome P450 thus making it less effective 4- BZ are Safe in overdose while Barbiturates have lower therapeutic index (easily overdosed) They don’t produce marked and fatal CNS depression Symptoms of overdose of BZ are less than of barbiturates 5- BZs produce minimal sedation and motor impairment 6- A Benzodiazepine antagonist is available (Flumazenil) Advanges as Hypnotics REM sleep ( rapid eye movement) is less affected if compared with the same effect of other hypnotics artificial interruption of REM sleep causes irritability and anxiety even if the total amount of sleep is not reduced BZ antagonist “Flumazenil” Mechanism of action Flumazenil acts as a competitive antagonist to the binding of BZs to their receptors Flumazenil is a short-acting drug while, most BZs have longer halflives, therefore, repeated i.v. administration of flumazenil is required to avoid relapse into the sedative state Side Effects •Drowsiness and confusion, amnesia • BZ may paradoxically produce an increase in irritability and aggression in some individuals (particularly if short- acting drugs are given (triazolam) •Hypotension in old patients •Ataxia occurs at high doses and interfere with motor coordination (e.g. driving a car) •BZs enhance the depressant effect Tolerance and dependence •If high doses of BZs are given over a prolonged period, weight gain as well as physical dependence may develop • Abrupt discontinuation of BZs causes withdrawal symptoms, including confusion, anxiety, restlessness ,tremor and dizziness • Short-acting BZs (triazolam) cause more withdrawal effects Contraindications 1.Pregnancy, labour and lactation: During pregnancy Late in pregnancy or around the time of labor and delivery During the period of breast feeding 2. In patients with myasthenia gravis: due to the muscle relaxing effect of BZs 3.Pre-existing CNS depression II. BUSPIRONE Mechanism of action: Buspirone is a 5HT1A receptor agonist with anxiolytic activity but little sedation 5-HT1A receptors are inhibitory receptors that reduce the release of 5-HT and other mediators Advantages of buspirone: 1.Unlike BZs, buspirone has no sedative hypnotic, anticonvulsant, or muscle relaxant properties (anxiolytic only) 3.Buspirone causes less psychomotor impairment than BZs and does not affect driving skills 4. The drug does not potentiate the CNS depressant effects of other sedativehypnotics e.g. ethyl alcohol Disadvantages of buspirone: Its anxiolytic effect takes days or weeks to develop . (useful in chronic anxiety states) Buspirone is ineffective in controlling panic attacks or severe anxiety states Side effects Buspirone has side effects quite different from those of BZs. It does not cause sedation or motor incoordination, nor have withdrawal effects been reported. Main side effects are nausea, dizziness, headache and restlessness Less troublesome than the side effects of BZs IV. BARBITURATES Barbiturates are non-selective CNS depressants. They can produce varying degrees of CNS depression ranging from mild sedation to general anesthesia Barbiturates have been largely replaced by BZs, because of the following: High incidence of tolerance and physical dependence following chronic use Barbiturates have a low therapeutic index (they are dangerous in overdose) Barbiturates are enzyme inducers especially cytochrome P450 system, they increase the rate of metabolic degradation of many other drugs, so liable to cause drug interactions They don’t have an antagonist Mechanism of Action: Barbiturates like BZs, cause activation of GABAA receptor and opening of the Clchannel associated with the receptor The neuronal membrane is hyperpolarized and less likely to fire Actions : At low doses, produce sedation barbiturates At higher doses, they cause hypnosis followed by anesthesia Overdosage may cause respiratory depression and death CNS depression death ★ medullary depression★ Barbiturates anesthesia ★ hypnosis ★ BZDs sedation ★ antianxiety★ Relative concentration Classification •Ultra-short acting: Thiopental Na is an i.v. anesthetic that acts within seconds with short duration of action •Short-acting: Pentobarbital and secobarbital act for 3-8 hours •Long-acting: Phenobarbital (> than 24 h) Therapeutic Uses: 1- Anesthesia: Thiopental Na is used iv to induce anesthesia 2- As sedative-hypnotic agents: Barbiturates have been replaced by BZs 3-Anticonvulsants: Emergency treatment of convulsions in status epilepticus by thiopental as the last approach 4-Phenobarbital is used in long-term management of tonic-clonic seizures and eclampsia 5- To lower serum bilirubin in Neonatal jaundice (kernicterus) Barbiturates such as phenobarbital can increase the conjugation of bilirubin and reduces this risk by inducing the activity of glucuronyl transferase enzyme Side effects 1-CNS effects: drowsiness can interfere with motor & mental performance; hangover. In large doses, barbiturates cause marked depression of CNS (may be fatal) 2- Induction of P450 thus the rate at which they are metabolized increases over the first few days of administration. Also, it leads to increased metabolism of other drugs e.g. estrogen and warfarin ( oral contraceptives and oral anticoagulants) 3-Tolerance and physical dependence with prolonged use III. ZOLPIDEM, Z drugs Mechanism of action: Zolpidem is a non-benzodiazepine hypnotic that binds selectively to a subset of the BZs receptor family and facilitates GABAmediated neuronal inhibition Zolpidem has a rapid onset and a short duration of action (about 4 hours) Its action is antagonized by flumazenil Zopiclone is similar to zolpidem Advantages Disadvantages Rapid onset less daytime sleepiness Less tolerance or dependence with prolonged use It has no effect on psychomotor skills Antagonized by flumazenil Least effect on Short duration of action Nightmares GIT upset Respiratory depression occurs only if large doses of zolpidem are ingested together with other central depressants Hypnotic drugs Benzodiazepines (e.g. Temazepam , nitrazepam) Related drugs working on the BZ receptor (e.g. zolpidem, zopiclone) Sedating antihistamines (e.g. promethazine), which cause drowsiness and are used for occasional insomnia. They can impair performance the day after V. ETHYL ALCOHOL (Ethanol) Ethyl alcohol (ethanol) is the most abused drug in the world. Ethyl alcohol in low to moderate amounts relieves anxiety and causes euphoria Large dose causes hypnosis and respiratory depression which may be fatal Mechanism of action Ethanol enhances GABAmediated synaptic inhibition Ethanol inhibits excitatory NMDA glutamate receptors Treatment of Chronic Alcoholism •Hospitalization, psychotherapy and nutritional therapy may be needed. Drug therapy includes: •BZs (e.g. diazepam) are used to prevent alcohol withdrawal symptoms. They are preferred over barbiturates because of their wide margin of safety. The dose must be tapered slowly over several weeks Disulfiram The drug given by itself to nondrinkers has little effects however, it causes extreme discomfort to patients who drink alcohol (Flushing, throbbing headache, nausea, vomiting, sweating, hypotension and confusion) Mechanism of action Disulfiram acts by inhibiting aldehyde dehydrogenase thus, alcohol is metabolized as usual but acetaldehyde accumulates. Acetaldehyde will form the toxic intermediates; methanol and formaldehyde THANK U