Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Pharmacokinetics wikipedia , lookup
Pharmacognosy wikipedia , lookup
Effect size wikipedia , lookup
Pharmaceutical industry wikipedia , lookup
Clinical trial wikipedia , lookup
Neuropharmacology wikipedia , lookup
Drug interaction wikipedia , lookup
National Institute for Health and Care Excellence wikipedia , lookup
Adherence (medicine) wikipedia , lookup
Prescription costs wikipedia , lookup
Neuropsychopharmacology wikipedia , lookup
Theralizumab wikipedia , lookup
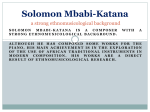
Chapter 8 Quality of Life Assessment 1 News • 乳癌的標靶治療用藥有了新突破!國內台大、 榮總、三總、馬偕、奇美、高醫、彰基等醫學 中心現正著手進行乳癌新藥Lapatinib的臨床 試驗,對於國內每年新增近五百人晚期患者來 說,可說是最後一線希望。 • 只要是HER-2成陽性反應,且屬於轉移性第四 期,嘗試過各種藥物都無效,就可能參加這項 人體試驗。 2 Targeted Clinical Trials • HER2 (the human epidermal growth factor receptor 2) gene in metastatic breast cancer - Herceptin requirement of screening the patients with overexpressed HER2 level (Slamon, 2001). • Estrogen receptor polymorphism - Estrogen Replacement Atherosclerosis trial (ERA, Herrington, et al, 2002): a total of 9 SNPs were identified and interaction between treatment of HRT and some of SNPs in elevation of lipid levels is suggested • Sample size determination: Fijal, et al. (2000) and Maitournam and Simon (2005). 3 Targeted Clinical Trials and EGFR • Iressa (gefitnib) and Tarceva (Erlotinib) are targted at the EGFR pathway. • Efficacy is correlated to race number of gene copies protein expression EGFR mutation Gappuzzo et al. (JNCI, 2005), Tsao, et al (NEJM, 2005) 4 Ethnic Difference Patients surviving (%) —— IRESSA ------ Placebo 1.0 1.0 1.0 0.9 0.9 Asian (n = 342) 0.9 HR = 0.66 (0.48, 0.91), P = .011 0.8 0.8 0.8 RR = 12.0% 0.7 0.7 0.6 0.5 0.5 0.5 0.4 0.4 0.4 0.3 0.3 0.3 0.2 0.2 0.2 0.1 0.1 0.1 0 0 11 22 33 44 55 RR = 6.5% 0.7 0.6 0.6 0.0 0.0 Non-Asian (n = 1350) HR = 0.93 (0.81, 1.08), P = .364 0.0 6 7 8 9 10 11 12 13 14 6 7 8 9 10 11 12 13 14 15 1500 11 22 33 44 55 6 77 88 99 10 10 11 1112 12 13 1314 14 15 15 6 Time, mo 5 From: Tsao, et al (2005, NEJM) 6 From: Tsao, et al (2005, NEJM) 7 Genomic Effect • The increasing evidence that genetic determinants may mediate variability among persons in the response to a drug implies that patient responses to therapeutics may vary among racial and ethnic groups. • After the intake of identical doses of a given agent, some ethnic groups may have clinically significant side effects, whereas others may have no therapeutic response. 8 Genomic Effect • Caraco (2004) points out that some of this diversity in rates of response can be ascribed to differences in the rate of drug metabolism, particularly by the cytochrome P-450 superfamily of enzymes • While ten isoforms of cytochrome P-450 are responsible for the oxidative metabolism of most drugs, the effect of genetic polymorphisms on catalytic activity is most prominent for three isoforms—CYP2C9, CYP2C19, and CYP2D6. 9 Genomic Effect • Among these three, CYP2D6 has been most extensively studied and is involved in the metabolism of about 100 drugs including beta-blockers, antiarrhythmic, antidepressant, neuroleptic, and opioid agents. • Several studies revealed that some patients are classified as having “poor metabolism” of certain drugs due to lack of CYP2D6 activity. 10 Genomic Effect • Patients having some enzyme activity are classified into three subgroups: those with “normal” activity (or extensive metabolism), those with reduced activity (intermediate metabolism), and those with markedly enhanced activity (ultrarapid metabolism). 11 Genomic Effect • The distribution of CYP2D6 phenotypes varies with race. For instance, the frequency of the phenotype associated with poor metabolism is 5 to 10 percent in the Caucasian population but only 1 percent in the Chinese and Japanese populations. 12 Example • Drug A is a fixed combination of two antiplatelet agents with indication for secondary prevention of thromboembolic stroke (200mg dipyridamole/25mg aspirin 1bid) After the standard process of BSE, we decided to request a bridging study due to an ethnic difference in medical practice (much lower dose for one of the components in Taiwan) and higher headache-associated dropout rate in previous Philippine study 13 Example • Headache drop out rate: Phillipino > Caucasian Local Bridging Study Result : first 4 weeks Group Placebo Reduced Dose 2wk Full Dose Full Dose 2wk 4wk Headache 8.7% 6.7% 16.3% drop out rate • Risk Management: Change labeling’s instruction for use 14 Why Are We Interested in the Quality of Life? The United States Food and Drug Administration has stated that efficacy with respect to overall survival and/or improvements in QOL might provide the basis for drug approval “Live longer – feel better” Shaughnessy JA, Wittes RE, Burke G et al. Commentary concerning demonstration of safety and efficacy of investigational anticancer agents in clinical trials. J Clin Oncol 1991; 9:2225-32. 15 Outline for Quality of Life • General background • Data collection considerations 16 Your Quality of Life How are you feeling this afternoon? Mood Happy Miserable 17 What is Quality of Life? WHO: “Health is not only the absence of infirmity and disease, but also a state of physical, mental and social well being Multiple domains include: physical, cognitive, emotional and social functioning, pain, sexual functioning, health perceptions, and symptoms such as nausea and fatigue Fundamental principle: quality of life is assessed by the patient 18 Quality of Life (1) • Definition depends on context Cancer vs. MI vs. hypertension • Some instruments are disease specific • Others are "general health status" instruments – POMS = Profile of Mood – SIP = Sickness Impact Profile • Difficulties with concept – No agreement on definitions – Lack of standardized measures 19 Quality of Life (2) • One definition (Levine & Croog) Two Components - Functioning 1. Social (Major component) - Get along with family & friends | sense of worth(家庭價值) 2. Physical - Perform daily life activities 3. Emotional - Stability and self control 4. Intellectual - Decision making ability - Perceptions 1. Life Satisfaction - Sense of well being(幸福感覺) 2. Health Status - Compared to others 20 Factors Which Influence Quality of Life 1. Intervention 2. Disease Process 3. "Labeling" Need a control group - Diagnosis brings on change 4. Concomitant Care 5. Non-related life events (e.g. death in family) 21 Rationale in Clinical Trials • Quality of life may assess effect of intervention – primary response (treatment less toxic?) – side effects (treatment toxic?) – economic aspects (low risk/cost treatment but benefit high?) 22 How To Assess Quality of Life • Determine your QoL Objective • Choose an instrument – Reliable, valid, responsive, feasible – Global measures, disease-specific measures, symptom checklists • Select your assessment time points and administration format • Develop an analysis plan 23 Data Collection Considerations (1) • Mode – Self-administered • glasses, reading skills, fine-motor skills – Personal interview • training/background of interviewer • sensitivity to gender/ethnicity/age • hearing impairment 24 Data Collection Considerations (2) • Content – instrument validity, sensitivity & specificity – sensitivity of questions – frame of reference for answers (cognitive skills, privacy, cultural background) • Source(s) – participant, family or support network, health care providers 25 Off the Shelf Instruments • Off-the-shelf instruments – Designed to distinguish sickness from wellness – May not be sensitive to particular aspect of a given trial – May not be validated or "normed" in population being tested – May ask ridiculous questions for trial pop. – May take hours to complete – May impact negatively on compliance 26 Off-the-Shelf Instruments (Example-NOTT) • Design – Advanced Chronic Obstructive Pulmonary Disease – 24 vs. 12 hours of O2 – Quality of life 10 outcome (No norms in this pop!) • Quality of Life Results – Patients were sick – Patients got worse – No treatment difference BUT – Mortality ratio was 2/1 (p<.01) 27 More Perspectives • "Tailor Made" Instruments – Can be Quick and simple – Standardized but targeted to disease – Must be Validated for trial population – Select subsets of off-the-shelf instruments 28 More Perspectives • “Home-made" Instruments – Often designed by a graduate student – Often too long – Often not validated or field tested on your patient population 29 Quality of Life Instruments • Can be simple and short • Classic examples for – Cancer – Congestive Heart Failure 30 31 32 33 Quality of Life Analysis • Analytic methods likely to be based on a scoring system • Methods often rank based • Challenging to design/ compute sample size 34 Statistical Consideration • Multi-trait scaling and other construct examination • Reliability (internal consistency and testretest reliability) • Correlation analyses with other instruments • Clinical validity (known group comparisons (sensitivity)) • Responsiveness to change over time 35 Multi-trait Scaling (1) • Multi-trait scaling analysis will be employed to examine whether the individual items in the instrument can be aggregated into hypothesised multi-item scales • Evidence of item convergent validity is defined as correlation of 0.40 or greater between an item and its own scale (corrected for overlap). 36 Multi-trait Scaling (2) • Evidence of item discriminant validity will be based on a comparison of correlation of an item with its own scale and with other scales • Scaling success for any item is defined as an item correlated significantly higher with its own scale (corrected for overlap) than with another scale 37 Reliability • The internal consistency of the multi-item questionnaire scales will be assessed by Cronbach’s alpha coefficient • A magnitude of >0.70 is considered acceptable for group comparisons • The test-retest reliability of scales will be assessed using intraclass correlations between the second and retest assessments in the patients 38 Clinical Validity • Known-group comparison will be used to assess whether the questionnaire scores can discriminate between subgroups of patients of clinical status 39 Responsiveness Over Time • Mixed effects regression model or generalized estimating equations (GEE) will be used to test for the significance of changes in QL scores before and after treatment 40 Sample Size Requirements • The sample size is based on the recommendation of Tabachnik and Fidell that for multivariate analysis techniques to obtain reliable estimates the number of observations should be 10 times the number of variables in the model 41 EORTC QLQ-C30 (version 3) 台灣中文 版 (1) 1. 2. 3. 4. 5. 您從事一些費力的活動,如攜帶重物或手提箱,是 否有困難?完全沒有,有一點,相當多,非常多 您從事長距離步行,是否有困難?完全沒有,有一點, 相當多,非常多 您在戶外從事短距離步行,是否有困難?完全沒有, 有一點,相當多,非常多 您在白天是否需要待在床上或椅子上?完全沒有,有 一點,相當多,非常多 您進食、穿衣、洗澡或上廁所需要別人幫助嗎?完 全沒有,有一點,相當多,非常多 42 EORTC QLQ-C30 (version 3) 台灣中文 版 (2) 在過去一星期內(過去七天內): 6. 您在從事工作或日常生活上是否受到限制?完全沒有, 有一點,相當多,非常多 7. 您在從事嗜好或休閒生活上是否受到限制?完全沒有, 有一點,相當多,非常多 8. 您呼吸會喘嗎?完全沒有,有一點,相當多,非常多 9. 您曾感到頭痛嗎?完全沒有,有一點,相當多,非常多 10. 您需要休息嗎?完全沒有,有一點,相當多,非常多 43 EORTC QLQ-C30 (version 3) 台灣中文 版 (3) 11. 您曾難以入睡嗎?完全沒有,有一點,相當多,非常多 12. 您曾感到虛弱嗎?完全沒有,有一點,相當多,非常多 13. 您曾缺乏食慾嗎?完全沒有,有一點,相當多,非常多 14. 您曾感到噁心嗎?完全沒有,有一點,相當多,非常多 15. 您曾嘔吐嗎?完全沒有,有一點,相當多,非常多 16. 您曾便秘嗎?完全沒有,有一點,相當多,非常多 17. 您曾腹瀉嗎?完全沒有,有一點,相當多,非常多 18. 您疲倦嗎?完全沒有,有一點,相當多,非常多 19. 疼痛干擾您日常生活嗎?完全沒有,有一點,相當多,非 常多 44 EORTC QLQ-C30 (version 3) 台灣中文 版 (4) 20. 您曾否難將注意力集中在一些事情上,如看報紙或看 電視?完全沒有,有一點,相當多,非常多 21. 您覺得緊張嗎?完全沒有,有一點,相當多,非常多 22. 您感到憂慮嗎?完全沒有,有一點,相當多,非常多 23. 您覺得容易發怒嗎?完全沒有,有一點,相當多,非常多 24. 您覺得情緒低落嗎?完全沒有,有一點,相當多,非常多 25. 您曾感到記憶困難嗎?完全沒有,有一點,相當多,非常 多 26. 您的身體狀況或醫療過程是否曾干擾您的家庭生活?完全沒有, 有一點,相當多,非常多 27. 您的身體狀況或醫療過程是否曾干擾您的社交生活?完全沒有, 有一點,相當多,非常多 28. 您的身體狀況或醫療過程是否曾造成您財務上的困難?完全沒有, 有一點,相當多,非常多 45 EORTC QLQ-C30 (version 3) 台灣中文 版 (5) 29. 您如何評定過去一星期內(過去七天內 )您整體的健康?1(非常差)234567( 極好) 30. 您如何評定過去一星期內(過去七天內 )您整體的生活品質?1(非常差)2345 67(極好) 46 FACT-P (第四版) (1) 生理健康狀況 一點也不 有一點 有些 相當 非常 GP1 我精神不好 0 1 2 3 4 GP2 我有反胃噁心的情形 0 1 2 3 4 GP3 因為我的身體狀況,我有困難達到家人的需求 0 1 2 3 4 GP4 我有疼痛 0 1 2 3 4 GP5 我有治療的副作用感到困擾 0 1 2 3 4 GP6 我覺得身體不適 0 1 2 3 4 GP7 我因疾病被迫要臥床休息 0 1 2 3 4 47 FACT-P (第四版) (2) 社會/家庭健全狀況 一點也不 有一點 有些 相當 非常 GS1 我覺得與我的朋友親近 0 1 2 3 4 GS2 我從我家人獲得情緒上的支持 0 1 2 3 4 GS3 我從我朋友獲得支持 0 1 2 3 4 GS4 我家人已接受我的疾病 0 1 2 3 4 GS5 我滿意家人間對我疾病的溝通方式 0 1 2 3 4 GS6 我覺得與我的伴侶 (或我主要支持者) 親近 0 1 2 3 4 0 1 2 3 4 Q1 不管你近期的性生活的程度,請回答下面的問 題。如果你不回答,請在這裡註明 GS7 我對我的性生活感到滿意 48 FACT-P (第四版) (3) 情緒穩定狀況 一點也不 有一點 有些 相當 非常 GE1 我感到悲傷 0 1 2 3 4 GE2 我滿意自己處理疾病的方式 0 1 2 3 4 GE3 我逐漸失去對抗我的疾病的希望 0 1 2 3 4 GE4 我覺得緊張 0 1 2 3 4 GE5 我擔心死亡 0 1 2 3 4 GE6 我擔心我的狀況會惡化 0 1 2 3 4 49 FACT-P (第四版) (4) 功能健全狀況 一點也不 有一點 有些 相當 非常 GF1 我能夠工作 (包括在家的工作) 0 1 2 3 4 GF2 我的工作 (包括在家的工作) 令人滿意 0 1 2 3 4 GF3 我能夠享受生活 0 1 2 3 4 GF4 我已接受我的疾病 0 1 2 3 4 GF5 我睡得好 0 1 2 3 4 GF6 我依然享受我以前常做的有趣的事 0 1 2 3 4 GF7 我滿足我現在的生活品質 0 1 2 3 4 50 FACT-P (第四版) (5) 附加關注事項 一點也不 有一點 有些 相當 非常 C2 我的體重正在減輕當中 0 1 2 3 4 C6 我有好胃口 0 1 2 3 4 P1 身體的疼痛困擾著我 0 1 2 3 4 P2 我感到身體的某些部位有顯著的疼痛 0 1 2 3 4 P3 我的疼痛使我無法去做我想做的事 0 1 2 3 4 P4 我滿意目前的舒適程度 0 1 2 3 4 P5 我能夠覺得像一個男人 0 1 2 3 4 P6 我有排便的困難 0 1 2 3 4 P7 我解尿時有困難 0 1 2 3 4 我解尿的問題限制了我的活動 0 1 2 3 4 我能夠且維持勃起 0 1 2 3 4 BL2 P8 BL5 我比以前頻尿 51