Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Adherence (medicine) wikipedia , lookup
Environmental impact of pharmaceuticals and personal care products wikipedia , lookup
Psychedelic therapy wikipedia , lookup
Specialty drugs in the United States wikipedia , lookup
National Institute for Health and Care Excellence wikipedia , lookup
Orphan drug wikipedia , lookup
Polysubstance dependence wikipedia , lookup
Neuropharmacology wikipedia , lookup
Pharmacognosy wikipedia , lookup
Prescription drug prices in the United States wikipedia , lookup
Pharmacogenomics wikipedia , lookup
Drug interaction wikipedia , lookup
Pharmaceutical industry wikipedia , lookup
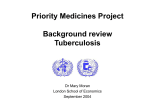
Neuropsychopharmacology wikipedia , lookup
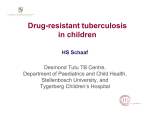
Thank you for viewing this presentation. We would like to remind you that this material is the property of the author. It is provided to you by the ERS for your personal use only, as submitted by the author. 2012 by the author MDR-TB management: what is new? GB Migliori WHO Collaborating Centre for TB and Lung Diseases, Fondazione S. Maugeri, Tradate Italy Aims • • • • • To describe and discuss: Existing guidelines and definitions The epidemiology of TB and MDR-TB in Europe and globally derived from surveillance and M&E (Monitoring and Evaluation) The new information on MDR-TB diagnosis The new information on MDR-TB treatment The principles of MDR-TB control, with prevention and public health aspects 3 Aims • • • • • To describe and discuss: Existing guidelines and definitions The epidemiology of TB and MDR-TB in Europe and globally derived from surveillance and M&E (Monitoring and Evaluation) The new information on MDR-TB diagnosis The new information on MDR-TB treatment The principles of MDR-TB control, with prevention and public health aspects 4 200 0 5 6 Guidelines for the programmatic management of drug-resistant tuberculosis (1) 1 Background information on DR-TB 2 Framework for effective control of DR-TB 3 Political commitment and coordination 4 Definitions: case registration, bacteriology and treatment outcomes 5 Case-finding strategies 6 Laboratory aspects 7 Treatment strategies for MDR-TB and XDR-TB 8 Mono- and poly-resistant strains 9 Treatment of DR-TB in special conditions and situations 10 DR-TB and HIV infection 11 Initial evaluation, monitoring of treatment and management of adverse effects 7 Guidelines for the programmatic management of drug-resistant tuberculosis (2) 12 Treatment delivery and community-based DR-TB support 13 Management of patients with MDR-TB treatment failure 14 Management of contacts of MDR-TB patients 15 Drug resistance and infection control 16 Human resources: training and staffing 17 Management of second-line antituberculosis drugs 18 Category IV recording and reporting system 19 Managing DR-TN through patient-centered care ANNEX 1 Drug information sheets ANNEX 2 Weight-based dosing of drugs for adults ANNEX 3 Suggestions for further reading ANNEX 4 Legislation, human rights, and patient’s right in TB care prevention and control ANNEX 5 Use of experimental drugs outside of clinical trials 8 ANNEX 5 Methodology Causes of DR 9 Causes of MDR Patient mismanagement 10 DOTS FUNDING: Government Commitment (10$/ case) DIAGNOSIS: SS microscopy, QA and safety measures MDR-TB > money Up to 20,000 $/ case +C, DST, SRL, QA, infection control TREATMENT: SCC,DOT, 6-8 months, no hospitalization 24 months, mandatory DOT & hospitalization in reference facilities TB drugs only, no AE relevant toxicity, need special drugs + expertise TREATMENT MONITORING: SS, standard outcome definitions C, DST, special outcome definitons 11 Definitions • • • • Mono-R Poly-R MDR XDR • SS+, C+ • Cure, failure • Treatment monitoring 12 XDR= extensively drug-resistant TB Definition Resistance to at least rifampicin and isoniazid, in addition to any fluoroquinolone, and to at least one of the three following injectable drugs used in anti-TB treatment: capreomycin, kanamycin and amikacin. 13 XDR= HR + 1 FQ + 1 Injectable (KM or AMK or CM) 1st-line oral •INH Injectables •RIF •SM Fluoroquinolones •PZA •KM •Cipro •EMB •AMK •Oflox •Levo •CM •(Rfb) •Moxi •(Gati) Oral bacteriostatic 2nd line •ETA/PTA •PASA •CYS Unclear efficacy Not routinely recommended, efficacy unknown, e.g., amoxacillin/clavulanic acid, clarithromycin, clofazamine, linezolid, inmipenem/cilastatin, 14 high dose isonizid Aims • • • • • To describe and discuss: Existing guidelines and definitions The epidemiology of TB and MDR-TB in Europe and globally derived from surveillance and M&E (Monitoring and Evaluation) The new information on MDR-TB diagnosis The new information on MDR-TB treatment The principles of MDR-TB control, with prevention and public health aspects 15 Estimated absolute numbers of reported cases with MDR-TB* <100 100–999 1000–9999 >10,000 *among reported pulmonary TB patients Distribution of MDR-TB among new TB cases, 1994-2010. 17 Distribution of MDR-TB among previously treated TB cases, 1994-2010. 18 Top 19 settings with MDR among new cases > 6% (1994-2007) Indicates survey data reported in an earlier phase of the project 19 The new MDR-TB world record The highest proportions of MDR-TB ever reported in a survey have recently been found in Minsk, the capital city of Belarus: • 35.3% (95%CI: 27.7-42.8) in new pts • 76.5% (95%CI: 66.1-86.8) in previously treated pts 20 Notifications of MDR-TB increasing BUT only ~ 1 in 6 (16%) of estimated cases of MDR-TB among reported TB patients diagnosed and treated in 2010 Notified cases of MDR-TB Global Plan target ~270,000 in 2015 MDR-TB cases treated and estimated numbers not treated for MDR-TB, among notified TB patients, 2010 290,000 53,000 19,000 Proportion of TB patients tested for MDR-TB remains low New cases Global plan target for 2015 = 20% Previously treated Global plan target for 2015 = 100% Scale-up of MDR-TB treatment vs. Global Plan targets 2007 2008 2009 2010 2011 2012 2013 2014 2015 Trend of MDR-TB among new cases, Estonia, Latvia and…Tomsk Oblast, RF Estonia Latvia Tomsk oblast, RF TB notification rate % MDR among new 24 Countries that had reported at least one XDR-TB case by Oct 2011 Aims • • • • • To describe and discuss: Existing guidelines and definitions The epidemiology of TB and MDR-TB in Europe and globally derived from surveillance and M&E (Monitoring and Evaluation) The new information on MDR-TB diagnosis The new information on MDR-TB treatment The principles of MDR-TB control, with prevention and public health aspects 26 20/36 HBCs* have insufficient capacity to diagnose MDR-TB ≥1 Culture and DST <1 laboratories per 5M, 2010 *HBC= high-burden country Countries = Afghanistan, Armenia, Azerbaijan, Bangladesh, Belarus, Brazil, Bulgaria, Cambodia, China, DR Congo, Estonia, Ethiopia, Georgia, India, Indonesia, Kazakhstan, Kenya, Kyrgyzstan, Latvia, Lithuania, Mozambique, Myanmar, Nigeria, Pakistan, Philippines, Republic of Moldova, Russian Federation, South Africa, Tajikistan, Tanzania, Thailand, Uganda, Ukraine, Uzbekistan, Viet Nam, Zimbabwe Traditional view: who needs DST? • • • • • • • • • • Cat I, II failures, chronics Failure anti-TB TX in the private sector Contacts of DR-/MDR-TB HCW at risk, prisoners, homeless, etc. No SS/C conversion Month 2,3 Residence in very high DR-prevalence settings Exposure to poor quality drugs Previous treatment by poor programmes Co-morbidities favouring rapid transit/ malabsorbtion HIV+ 28 Who needs DST? • • • • • • • • • • Cat I, II failures, chronics Failure anti-TB TX in the private sector Contacts of DR-/MDR-TB HCW at risk, prisoners, homeless, etc. No SS/C conversion Month 2,3 Residence in very high DR-prevalence settings Exposure to poor quality drugs Previous treatment by poor programmes Co-morbidities favouring rapid transit/ malabsorbtion HIV+ • ALL CASES?? 29 The “magic” Gene Xpert Roll-out of Xpert MTB/RIF As of 30 September 2011 GeneXpert ordered – 40 countries 105 countries eligible for concessional prices, no order yet Not eligible for concessional pricing Source: FIND; more info at: www.who.int/tb/laboratory/mtbrifrollout 32 The message Any person at high risk of MDR-TB should • undergo rapid testing • to start an appropriate treatment immediately • while an additional sputum specimen undergoes conventional culture and DST 33 Aims • • • • • To describe and discuss: Existing guidelines and definitions The epidemiology of TB and MDR-TB in Europe and globally derived from surveillance and M&E (Monitoring and Evaluation) The new information on MDR-TB diagnosis The new information on MDR-TB treatment The principles of MDR-TB control, with prevention and public health aspects 34 The challenge of MDR 35 Expensive and toxic drugs are necessary 36 Grouping drugs Group 1 1st-line oral •INH Injectables •RIF •SM Fluoroquinolones •PZA •KM •Cipro •EMB •AMK •Oflox •Levo •CM •(Rfb) Group 2 Group 3 •Moxi •(Gati) Group 4 Oral bacteriostatic 2nd line •ETA/PTA •PASA •CYS Group 5 Unclear efficacy Not routinely recommended, efficacy unknown, e.g., amoxacillin/clavulanic acid, clarithromycin, clofazamine, linezolid, inmipenem/cilastatin, 37 high dose isonizid How to design a MDR-TB regimen 38 39 Metanalysis of 9,153 cases from 32 Countries • Treatment success vs. to failure/relapse, was associated with use of: • later generation quinolones, ofloxacin, ethionamide or prothionamide • use of 4 or more likely effective drugs in the initial intensive phase, and 3 or more likely effective drugs in the continuation phase. • Maximum odds of success: initial intensive phase of 7.1-8.5 months and total treatment duration of 18.6-21.5 months Changes to the recommendations on regimen composition between the 2008 and 2011 updates of WHO MDR-TB guidelines 2008 emergency update 2011 update Include at least four anti-TB drugs with either certain, or almost certain, effectiveness during the intensive phase of Tx Include at least 4 2nd -line anti-TB drugs likely to be effective as well as Z during the intensive phase of Tx Consider adding more drugs in patients with extensive disease or uncertain effectiveness No evidence found to support the use of > 4 2nd-line anti-TB drugs in patients with extensive disease. Increasing the number of 2nd line drugs in a regimen is permissible if the effectiveness of some of the drugs is uncertain. The regimen should include Z and/or E one FQ, one parenteral agent and 2nd -line oral bacteriostatic anti-TB drugs (no preference of oral bacteriostatic 2nd -line anti-TB drug was made). E may be considered effective and included in the regimen if DST shows susceptibility Tx with Group 5 drugs is recommended only if additional drugs are needed to bring the total to 4 The regimen should include Z a FQ, a parenteral agent, ethionamide (or prothionamide), and cycloserine, or else PAS if cycloserine cannot be used. E may be used but is not included among the drugs making up the standard regimen. Group 5 drugs may be used but are not included among the drugs making up the standard 41 regimen Treatment monitoring • Treatment failure was detected best with monthly culture in MDR-TB cases. • Thus the available evidence does not support replacing monthly culture (or quarterly culture) with monthly smear 43 44 45 GLC: advantages for projects • Access to quality-assured drugs • Access to low-cost drugs • Access to a continuous drug supply • Access to technical assistance • Access to an external monitoring mechanism • Increased rational use of drugs • Creation of wide evidence base for policy development 46 Estonia % of NTP budget spent on second line drugs 1998-2000 100% 73% 80% 60% 15% 40% 20% 0% Open Market Prices GLC Prices 47 MDR treatment programme Decentralised case management Centralised Registration Establishment of treatment Monitoring Data management Supervision Decentralised case management Case finding Case management • in specialized MDR-TB hospitals • in district TB department, at home, at family physician Ensure adherence Record keeping Consilium for MDR-TB case and programme management 48 Latvia, Side Effects - Cohort 2000 86% of patients experienced side effects Median of 4 side effect reports per person Most common side effects • • • • • Nausea Vomiting Abdominal pain Dizziness Hearing problems 73.0% 38.7% 38.2% 35.8% 28.4% 61% changed or discontinued drugs during treatment owing to side effects 2 patients stopped treatment due side effects 49 Results: Final Conversion Over Time N = 129 patients who converted, Latvia 50 51 What was not known on XDR? • Is the risk of death/ probability of success different from that of MDR? • Are their clinical characteristics different? in HIV-negative patients? • Is their infectiousness different? • Has the XDR definition a clinical relevance? Which is the role of susceptibility to first-line drugs different from HR? 53 54 55 XDR: a death sentence? 56 57 XDR compared with MDR, Italy-Germany • Death rate: 36.4 % vs 6.3% (RR 5.45) • Longer hospitalization (241.2±177.0 vs. 99.1±85.9 days) Cost? • Longer treatment duration (30.3±29.4 vs. 15.0±23.8 months) Cost? • Bacteriological conversion in 4/11 XDRvs. 102/126 MDR-TB cases (median: smear: 110 vs. 41 days; culture: 97.5 vs. 58 days) Cost of new infections? 58 Emerging Infectious Diseases 2007 4,853 C+, 361 MDR, 64 XDR MDR-TB, susceptible at least one 1st drug MDR-TB, resistant to all 1st line drugs XDR-TB 59 Eur Respir J 2007 Aims • • • • • To describe and discuss: Existing guidelines and definitions The epidemiology of TB and MDR-TB in Europe and globally derived from surveillance and M&E (Monitoring and Evaluation) The new information on MDR-TB diagnosis The new information on MDR-TB treatment The principles of MDR-TB control, with prevention and public health aspects 60 TB patients with inappropriate regimen have a 27fold higher risk of developing MDR-TB Multidrug resistance after inappropriate tuberculosis treatment: A meta-analysis Marieke J. van der Werf, Miranda W. Langenda3, Emma Huitric, Davide Manissero ERJ 2012 in press 61 Global Policy: MDR-TB and XDR-TB 1. 2. 3. 4. 5. 6. 7. 8. Strengthen basic TB control, to prevent M/XDR-TB Scale-up programmatic management and care of MDR-TB and XDR-TB Strengthen laboratory services for adequate and timely diagnosis of MDR-TB and XDR-TB Ensure availability of quality drugs and their rational use Expand MDR-TB and XDR-TB surveillance Introduce infection control, especially in high HIV prevalence settings Mobilize urgently resources domestically and internationally Promote research and development into new diagnostics, drugs and vaccines 62 Global Policy: MDR-TB and XDR-TB 1. 2. Strengthen basic TB control, to prevent M/XDR-TB Scale-up programmatic management and care of MDR-TB and XDR-TB 3. Strengthen laboratory services for adequate and timely diagnosis of MDR-TB and XDR-TB 4. Ensure availability of quality drugs and their rational use Expand MDR-TB and XDR-TB surveillance Introduce infection control, especially in high HIV prevalence settings Mobilize urgently resources domestically and internationally Promote research and development into new diagnostics, drugs and vaccines 5. 6. 7. 8. 63 Global Policy: MDR-TB and XDR-TB 1. 2. 3. 4. 5. 6. 7. 8. Strengthen basic TB control, to prevent M/XDR-TB Scale-up programmatic management and care of MDR-TB and XDR-TB Strengthen laboratory services for adequate and timely diagnosis of MDR-TB and XDR-TB Ensure availability of quality drugs and their rational use Expand MDR-TB and XDR-TB surveillance Introduce infection control, especially in high HIV prevalence settings Mobilize urgently resources domestically and internationally Promote research and development into new diagnostics, drugs and vaccines 64 Global Policy: MDR-TB and XDR-TB 1. 2. 3. 4. 5. 6. 7. 8. Strengthen basic TB control, to prevent M/XDR-TB Scale-up programmatic management and care of MDR-TB and XDR-TB Strengthen laboratory services for adequate and timely diagnosis of MDR-TB and XDR-TB Ensure availability of quality drugs and their rational use Expand MDR-TB and XDR-TB surveillance Introduce infection control, especially in high HIV prevalence settings Mobilize urgently resources domestically and internationally Promote research and development into new diagnostics, drugs and vaccines 65 Global Policy: MDR-TB and XDR-TB 1. 2. 3. 4. 5. 6. 7. Strengthen basic TB control, to prevent M/XDR-TB Scale-up programmatic management and care of MDR-TB and XDR-TB Strengthen laboratory services for adequate and timely diagnosis of MDR-TB and XDR-TB Ensure availability of quality drugs and their rational use Expand MDR-TB and XDR-TB surveillance Introduce infection control, especially in high HIV prevalence settings Mobilize urgently resources domestically and internationally 8. Promote research and development into new diagnostics, drugs and vaccines 66 “Nobody wants me around..” 67 68 Interventions over time: old weapons might be useful again to manage XDR First sanatorium Germany, 1857 First Dispensary, Scotland, 1897 BCG vaccination Pneumotorax, Italy, 1907 Drugs, 1945-1962 Koch, Mtb, 1882 MMR,1950-1980 Fox:Ambulatory treatment, 1968 Styblo model, 1978 DOTS, 1991 Outbreak Management, sanatoria Risk Group Management screening drug therapy Socio-economic improvement 69 XDR and TB control: which future ? 70