Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
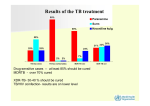
Diagnosis and treatment of MDR/XDR tuberculosis in HIV-infected patients in a slum setting in Mumbai, India Chiara Montaldo,1 Atul Dongre,1 Bhanumathi Varghese,1 Camilla Rodrigues,2 Giovanni Sotgiu,3 Rossella Centis,4 Gianbattista B Migliori,4 Emanuele Pontali,5 Tony Reid6 1MSF HIV/AIDS Comprehensive Care Clinic, Mumbai, India; 2Hinduja Hospital, Microbiology Laboratory, Mumbai; 3University of Sassari, Hygiene and Preventive Medicine Institute, Sassari, Italy; 4S Maugeri Foundation, Care and Research Institute, WHO Collaborating Centre for TB and Lung Diseases, Tradate, Italy; 5Galliera Hospital, Dept of Infectious Diseases, Genoa, Italy; 6MSF, Brussels, Belgium Contact: [email protected] Background Multi- and extensively drug-resistant tuberculosis (MDR/XDR-TB) increases mortality among HIVinfected patients. Treatment is associated with adherence challenges and drug toxicities. The MSF HIV/AIDS Comprehensive Care Clinic in Mumbai serves an extremely heavily populated urban area with substandard housing. Treatment is on an outpatient basis in collaboration with a network of non-governmental organisations (NGOs) and public and private directly observed therapy (DOT) providers. Methods We describe the outcomes of HIV-infected patients with MDR/XDR-TB followed by the MSF clinic from February 2006. All patients were screened for TB symptoms. Patients with confirmed MDR/XDR-TB received daily DOT (at least five drugs) given by the provider closest to the patient’s residence. MSF staff delivered drugs to the DOT provider monthly and telephoned weekly to identify adherence problems. Local NGOs traced defaulters and reinforced adherence messages. Patients visited the clinic monthly for medical assessment. Results Of our cumulative cohort of 611 patients (active 350), 193 were suspected of having TB and were screened with sputum microscopy, culture, and drug susceptibility testing. 34 samples grew Mycobacterium tuberculosis: nine were fully sensitive; 25 had drug resistance. Of the 25, 14 (56%) were resistant to all first-line drugs and 11/22 (50%) to fluoroquinolones (three had no history of TB treatment). MDR strains were identified in 18/25 (72%) and XDR in 2/25 (8%). Two patients presented symptoms suggestive of extra-pulmonary TB and started MDR-TB treatment. Pulmonary TB was diagnosed in 22 (82%) and extra-pulmonary in 5 (23%; one had both). 14 (53%) had already received at least one full course of TB treatment. 22 (81%) received HAART (12 started before diagnosis, 10 during treatment). 24 started TB treatment; three died before confirmation of MDR-TB. In February 2009, six were cured (WHO definition), four had died, five defaulted, and nine were still on treatment. 16/20 showed culture conversion. 21 received drugs with potential thyroid toxicity. Side-effects included thyroid dysfunction (eight [30%]), tendonitis (three [11%]), gastrointestinal disorders (three [11%]), and psychosis (two [7.4%]). Conclusions Our results are preliminary and the cohort is small, but integrating HIV, TB, and MDR/XDR-TB care was feasible and essential for the correct management of these patients. Implementing MDR/XDRTB care on an outpatient basis within an HIV clinic required infection control measures and involvement with local health structures and NGOs. Decentralised centres, easily accessible to patients, were essential. The high rate of thyroid toxicity reinforces recommendations to monitor and treat thyroid dysfunction.