Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
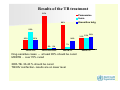
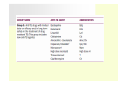
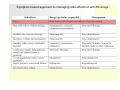
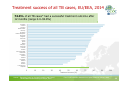
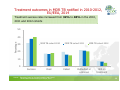
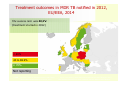
Results of the TB treatment 95% Paranemine Surm Krooniline kulg 69% 50% 31% 33% 25% 25% 36% 24% 7% 2% TB ilma ravita 2% TB hea ravikorraldus MDR TB ravi Drug-sensitive cases -- at least 85% should be cured MDRTB - over 70% cured XDR-TB- 30-40 % should be cured TB/HIV coinfection- results are on lower level XDR-TB ravi TREATMENT REGIMENS l The preferred regimen for active drug-sensitive TB disease is minimum of 6 months First 2 months (the intensive phase of treatment), rifampicin, isoniazid, pyrazinamide, ethambutol followed by isoniazid and rifampicin for 4 months (the continuation phase of treatment) Relaps - 8 months 3 months 5 months - 5 drugs - 3 drugs Treatment efficacy and progress are usually monitored with repeat sputum smears, cultures and chest X-rays. TB treatment is free for all persons in Estonia, despite of living place and having health insurance or not Drug dosing freaquency • The optimal dosing frequency is daily throughout the course of therapy • Dosing of anti-TB drugs is based on the weight of the patient. • Monthly monitoring of patient body weight is important, medication dose should be adjusted. • Once-daily dosing is mandatory for anti-TB drugs from Group 1, 2, and 3, as this is thought to improve the peak-dependent killing. • Twice-daily dosing is an excellent strategy to reduce adverse effects of Group 4 drugs. • Many patients can tolerate a full dose of ethionamide and cycloserine once daily Traditionally they have been given twice daily to reduce adverse effects. • Once-daily dosing is allowed for Group 4 drugs. There are no studies comparing once-daily to twice-daily dosing for Group 4 drugs in terms of efficacy. The common adverse events are mild increases in the level of liver enzymes, skin rash, gastrointestinal intolerance, neuropathy and arthralgia and can be managed symptomatically without discontinuation of the offending drugs. Serious adverse events are severe hepatitis, immune thrombocytopaenia, agranulocytosis, haemolysis, renal failure, optic neuritis and ototoxicity. prolonged therapy undermines patient compliance. As a result, supportive measures are necessary to ensure optimal adherence, as lack of treatment completion contributes to treatment failure, relapse and the emergence of drug resistance. Symptom-based approach to managing side-effects of anti-TB drugs The action of anti-tuberculosis drugs 1. Rapidly multiplying→ INH 2. Slowly multiplying→ PZ 3. Intermittent growth→ RIF Bactericidal activity H>>SM>R>E Z>>R>H R>>H Total duration of MDR-TB treatment Treatment should continue for a minimum of 20 months and at least 18 months after the patient becomes culture-negative Chronic patients with extensive pulmonary disease may require MDR-TB treatment for 24 months or longer. A 9–12-month regimen (conditional WHO recommendation with very-low-quality evidence) might be used in selected patients, in appropriate settings, taking into account previous treatment and local resistance profiles Medicines recommended for the treatment of rifampicin-resistant and multidrug-resistant TB1 Directly Observed Treatment, DOT The most common adherence monitoring approach is directly observed therapy (DOT) • • Every dose of treatment is directly supervised by a health professional, although the effectiveness of this measure is controversial. Although DOT continues to be valuable in many settings, various alternative methods are now being tried out to improve adherence o mobile phone reminders, o smart pill boxes, o video DOT and the use of call centres to follow-up with patients. • Regardless of the method, it is crucial to use a team-based, patientcentric approach that incorporates education, counselling and patient empowerment. Surgical treatment It remains one of the treatment options for TB. Surgery has been employed in treating TB patients since before the advent of chemotherapy Segmentectomie, lobectomie, atypical resection, pulmonectomy Partial lung resection for patients with MDR-TB is only to be considered under conditions of good surgical S Facilities, trained and experienced surgeons and with careful selection of candidates. Treatment with TB drugs after hte surgery Drug sensitive TB case : 4-6 months MDR-TB: 9-12 months Аgnessa 29 years X-ray:10.01.2011 - before the surgery TB treatment before the surgery- 1 year After the surgery - 11 months TB treatment. EPTB A 6 to 9-month regimen is recommended as initial therapy for all forms of extrapulmonary tuberculosis unless the organisms are known or strongly suspected to be resistant to the first-line drugs. 2 months of isoniazid, rifampicn, pyrazinamide, ethambutol, 4 -7 months of isoniazid and rifampin For patients with CNS tuberculosis, including meningitis, at least nine to 12 months of therapy is recommended. Extended therapy also may be required for patients with bone and joint tuberculosis, delayed treatment response, or drug resistance. Adjunctive corticosteroids may be useful in patients who have tuberculous meningitis, tuberculous pericarditis, or miliary tuberculosis with refractory hypoxemia. Treatment success of all TB cases, EU/EEA, 2014 74.0% of all TB cases* had a successful treatment outcome after 12 months (range 0.0–92.8%) Slovakia Iceland Sweden Netherlands Norway Bulgaria United Kingdom Romania Belgium Slovenia Latvia Spain Malta Hungary Portugal Estonia Austria Czech Republic Lithuania Germany Poland Ireland Denmark Finland Cyprus Croatia Luxembourg EU/EEA 0 10 20 30 40 50 60 70 80 90 100 Treatment success (%) Source: European Centre for Disease Prevention and Control. TB surveillance and monitoring in Europe, 2016. * Four EU/EEA Member States did not report treatment outcome data 16 Indicator 7: Treatment success rate new pulmonary culture positive MDR TB cases* Target: Treatment success of 70% for new pulmonary culture-positive MDR TB cases Status 2014: Success rate in EU/EEA was 55.6% (range 0–100.0%), target met by 6 countries 17 European Centre for Disease Prevention and Control. Source: TB surveillance and monitoring in Europe, 2016. * Luxembourg reported ‘zero’ cases; France, Greece, and Italy did not report treatment outcome results. Treatment outcomes in MDR TB notified in 2010-2012, EU/EEA, 2014 Treatment success rates increased from 32% to 40% in the 2010, 2011 and 2012 cohorts 50 Percentage 40 MDR TB cohort 2010 30 MDR TB cohort 2011 MDR TB cohort 2012 20 10 0 Success Died Source: European Centre for Disease Prevention and Control. TB surveillance and monitoring in Europe, 2016. Failed Defaulted or unknown Still on treatment 18 Additional support Since 2011 the NTP allocates additional finances for provision of voluntary treatment of Alcohol Use Disorders and/or drug abuse (including methadone substitution treatment, naltrexone, disulfiram etc.) psycho-social counselling support together with TB treatment These additional services are given by a team consisting of social workers, psychologist, psychiatrist and they belong to this department. Treatment outcomes in MDR TB notified in 2012, EU/EEA, 2014 The success rate was 40,3% (treatment started in 2012 ) < 40% 40 to 69.9% ≥ 70% Not reporting 20 European Centre for Disease Prevention and Control. Source: TB surveillance and monitoring in Europe, 2016. * Cyprus, Luxembourg, Malta and Slovenia reported zero MDR TB cases in 2012. Nine Member States did not report treatment outcome data for MDR TB cases.