Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Pharmacokinetics wikipedia , lookup
Discovery and development of beta-blockers wikipedia , lookup
Environmental impact of pharmaceuticals and personal care products wikipedia , lookup
Discovery and development of cyclooxygenase 2 inhibitors wikipedia , lookup
Neuropharmacology wikipedia , lookup
Effect size wikipedia , lookup
Pharmacognosy wikipedia , lookup
Spironolactone wikipedia , lookup
Neuropsychopharmacology wikipedia , lookup
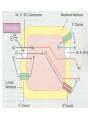
Diuretic drugs Assoc. Prof. Ivan Lambev ([email protected]) Diuretics exert their effect directly on the kidneys. Most of them lead to electrolyte excretion and Hydrochlorothiazide consequently to Chlorthalidone Indapamide osmotic excretion of water, which increases the 24-hr Mannitol urine volume. Amiloride Triamterene Spironolactone Acetazolamide Furosemide Furosemide Torsemide Torsemide 1. Salidiuretics (thiazides and their analogues) They increase equivalently Na+ and Clexcretion (1:1) in distal renal tubules and this increases diuresis. They lead to excretion of 5 to 10% from filtrated Na+ ions and have moderate diuretic action. They can be classified as sulfonamides with free –NH2 group, without antimicrobial activity. Salidiuretics (saluretics) Thiazides Thiazide analogues •Hydrochlorothiazide •Cyclopenthiazide •Clopamide •Chlorthalidone Vasodilators with antihypertensive effect •Indapamide (stimulates synthesis of renal PGs with vasodilating action) Indapamide SR (does not have metabolic effects) •cardioprotector •nephroprotector Hydrochlorothiazide Chlorthalidone Indapamide 5–10% Thiazides have a weak antihypertensive effect because they reduce arterial wall sensitivity to NA (noradrenaline) and AT (Angiotensin). They potentiate significantly the effect of other antihypertensive drugs. Thiazides increase plasma renin levels. Reduction of plasma Sodium and osmolarity leads to “paradoxal” antidiuretic effect in diabetes insipidus. Adverse reactions (ARs) of saluretics: Hypokalemia and enhancing therapeutic and toxic effects of CGs, hypochloremic alkalosis, GI disorders, skin rashes and photosensibilization, muscle weakness and fatigue, hyponatremia, hypoglycemia, increased plasma level of uric acids, hypercholesterolemia, impotence. Thiazides decrease GF (glomerul filtration). They reduce plasma volume in pregnant women and decrease fetal oxygenation (PRC: D). 2. Loop Diuretics Furosemide has p.o. bioavailability 65% and t1/2 30–60 min. It acts on the ascending limb of Henley's loop by increasing urine excretion of Na+, Cl, Mg2+ and Ca2+. Its diuretic effect is achieved in 20–30 min after p.o. administration and lasts 4–6 h. Its effect after i.v. administration begins in 3–5 min and lasts 2 h. In low doses (5 to 10 mg p.o.) furosemide has antihypertensive effect. It does not disrupt GF. Furosemide – indications: Oedemas of different origin, acute ischemic renal failure (in high DD, together with mannitol), anuria and eclampsia, forced diuresis in acute intoxications, hypertension, resistant cardiac failure. Furosemide enhances the action of antihypertensive drugs and non-depolarazing neuromuscular blockers. Furosemide – ARs: Hypokaliemia, skin rashes, hyperglycemia, increased plasma levels of uric acid. In fast i.v. administration – transient hearing disturbances with temporary deafness and orthostatic collapse. Ototoxic risk is increased in co-medicaton with aminoglycosides, cephalosporines, polymyxins, sulfonamides or quinolones. 3. Carbonic anhydrase inhibitors Acetazolamide inhibits carbonic anhydrase (CA) mainly in proximal tubules. H2O + CO2 CA H2CO3 H2CO3– + H+ Acetazolamide has weak diuretic action. It significantly enhances urine K+ excretion. The loss of HCO3– anions decreases blood alkaline reserve (for 48–72 h) and causes metabolic acidosis. In this state the drug becomes ineffective. Acetazolamide blocks not only renal CA, but also CA in the ciliary body in the eye (reducing production of eye liquid) and in the brain (facilitates GABA synthesis). 4. Potassiumsparing diuretics Amiloride Triamterene Spironolactone 3% They have weak diuretic action and save K+. Often they are used in combination with diuretics, causing hypokalemia. Potassium-sparing diuretics Competitive aldosterone antagonists: Blockers of the amiloride-sensitive Na+ channels: •Spironolactone •Amiloride •Triamterene Spironolactone is a steroid compound, which is a competitive aldosterone antagonist. It increases Na+ excretion and decreases K+ and urea excretion. Its diuretic action is weak and is achieved slowly. Spironolactone is effective in oedemas, caused by increased production of aldosterone ascites in liver cirrhosis and oedemas in congestive heart failure. Spironolactone in low doses (25 mg/24 h) potentiates the effect of ACE inhibitors. It saves K+ and Mg2+ ions and has antiarrhythmic effect. It also prevents the development of myocardial fibrosis, caused by aldosterone and in this way contributes to enhancing myocardial contractility. Diuretidin® (triamterene/hydrochlorothiazide) is indicated in oedemas cardiac, renal, liver or other origin and for the treatment of hypertension with other antihypertensive drugs. ® Moduretic (amiloride/hydrochlorothiazide) has the same indications too. 5. Osmotic diuretics 60–80% After oral administration Mannitol is not absorbed and has laxative effect. After i.v. administration it is not metabolized, it filtrates in the glomerulus and not reabsorbed in renal tubules, causing increased osmotic pressure and excretion of isoosmotic equivalent of water. It increases blood flow in 30%. Мannitol does not influence renin synthesis. It does not cross tissue barriers (BBB neither), does not penetrate to the eye and brain and in osmotic way reduces intraocular and intracranial pressure. It is included in the treatment of brain oedema, initial stages of acute renal failure, chronic renal failure, glaucoma, intoxications with drugs, excreted in the urine. 6. Phytodiuretics Rhizoma Graminis (Couch-grass) Stipites Cerasorum (Cherry) Fructus Faseoli sine semine (Haricot) Fructus Petroselini (Parsley) Stigmata Maydis (Maize, corn) Rubia tinctorum L. (madder). Radix Rubiae contains 2–3% di- or trioxyanthraquinones glycosides, flavonoids and other bioactive substances with diuretic, urolitholytic and spasmolytic effects. Infusions (1:10) made from madder facilitate dilution of calculi, containing calcium and magnesium sulfate in the renal pelvis and bladder. It is an important ingredient of many phytoproducts (Cystenal©, Rowatinex©), indicated in urolithiasis.