Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Medical prescription wikipedia , lookup
Discovery and development of beta-blockers wikipedia , lookup
Discovery and development of proton pump inhibitors wikipedia , lookup
Discovery and development of direct thrombin inhibitors wikipedia , lookup
Discovery and development of angiotensin receptor blockers wikipedia , lookup
Drug design wikipedia , lookup
Drug discovery wikipedia , lookup
Adherence (medicine) wikipedia , lookup
Pharmacognosy wikipedia , lookup
Electronic prescribing wikipedia , lookup
Pharmaceutical industry wikipedia , lookup
Pharmacogenomics wikipedia , lookup
Pharmacokinetics wikipedia , lookup
Neuropsychopharmacology wikipedia , lookup
Prescription drug prices in the United States wikipedia , lookup
Prescription costs wikipedia , lookup
Theralizumab wikipedia , lookup
Neuropharmacology wikipedia , lookup
Drug interaction wikipedia , lookup
Psychopharmacology wikipedia , lookup
Dydrogesterone wikipedia , lookup
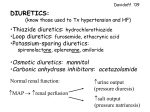
DIURETICS (2 of 2) Dr R. P. Nerurkar Dept. of Pharmacology T. N. Medical College & BYL Nair Ch. Hospital, Mumbai DECEMBER 7, 2005 Learning Objectives At the end of my 2 lectures you should be able to 1) List 5 major types of diuretics and their mechanism and site of action 2) List the major applications and toxicities of them 3) Describe the measures that reduce K+ loss during natriuresis 4) List the Rx of hypercalcimia and hypercalciuria 5) manage refractory edema cases 6) List Rx of nephrogenic diabetes insipidus Overview of 1st lecture • Definition • Physiology of Urine formation and drugs modifying it • Classification and Mechanism of action • Pharmacology of Loop diuretics and CA inhibitors • Group discussion and Exercises on – Prescription writing, – Patient oriented problem solving – Identification of drugs acting – ADR and drug interactions Thiazides - Sites of Action Thiazide Diuretics - Actions • Acts on early part of distal tubules • Inhibit Na+-Cl- symporter and reabsorption • Increase NaCl excretion (5-10% Medium efficacy) • Na exchanges with K+ in the DT K+ loss Hypokalemia • Not effective in very low GFR of < 30ml/min, may reduce GFR further – Metolazone additional action on PT, effective at low GFR, can be tried in refractory edema Thiazide Diuretics - Other actions • Hypotensive action • reduce Ca++ excretion may ppt hypercalcemia in patients of hyperparathyroidism, bone malignancy with metastasis • Increase Mg++ excretion • Hypochloremic alkalosis • Hyperuricemia • Hyperglycemia (inhibit insulin release ?) • Hyperlipidimia (Cholesterol and TG) Thiazides Preparations Drug Name Dose (oral) Duration (hr) Chlorothiazide (1957) 500-2000 6-12 Hydrochlorothiazide 25-100 8-12 Benzthiazide 25-100 12-18 Hydroflumethiazide 25-100 12 Chlorthalidone 50-100 48 Metolazone 5-20 18 Xipamide, Clopamide 20-40 12-24 Indapamide (No CAI) 2.5-5 24-36 Thiazides - Uses 1) Hypertension (Hydrochlorothiazide, Indapamide) 2) Edema : Cardiac, Hepatic Renal • Less efficacious than loop diuretic • Useful for maintainence therapy 3) Hypercalciuria and renal Ca stones 4) Diabetes Insipidus (DI) (Nephrogenic responds better) 5) • Paradoxical use, • MOA - ? Reduce GFR, ? More complete reabsorption in PT • Convenient, Cheaper than Desmopressin in Neurogenic DI • Amiloride is the DOC for Lithium induced nephrogenic DI Metolazone useful even when GFR is as low as 15ml/min Thiazides -Adverse Effects 1) Hypokalemia 7) Hypchloremic alkalosis 2) May ppt renal failure 8) Hypersensitivity 3) Hyperuricemia 9) ppt. Hypercalcemia 4) Hyperglycemia 5) Hyperlipidemia 10) Not safe in pregnancy (all diuretics) 6) Hypomagnesemia Osmotic Diuretics Ideal properties 1. Orally effective 2. Well abosorbed 3. Not metabolized 4. Freely filtered at glomeruli 5. Not reabsorbed 6. Inert 7. Cheap Drugs used • Mannitol • Glycerol • Isosorbide Mannitol - Actions • not mediated by any receptors or target site • Expands ECF volume – increase RBF, GFR • Osmotic gradient in the tubular lumen prevent reabsorption of mainly H2O dilute urine diuresis • prevent Na+ reabsorption - upto 20% NaCl excretion (Acute effect) • May inhibit transport process in Asc loop of Henle • classified as weak diuretic in some textbooks • never used for chronic edema or as a natriuretic Osmotic diuretic - Preparations Drug Daily dose Mannitol I.V. 1-2 gm/kg 10% or 20% soln. 100 – 300 ml rapid infusion Over 30 to 90 min Glycerol oral 1-1.5 gm/kg metabolized to glucose Isosorbide oral 1.5 gm/kg Mannitol - USES 1) ARF : treatment & prevention 2) To maintain GFR during major surgeries, trauma cases, severe jaundice, hemolytic reactions etc To lower intracranial tension Before brain surgery 3) To lower intraocular tension 4) Acute glaucoma Before intraocular surgeries Forced diuresis in drug poisoning 5) Cerebral edema (FAD in barbiturate poisoning To counteract low plasma osmolality after dialysis Mannitol -Adverse Effects 1) Acute Intravascular volume expansion • Before diuresis starts it exerts osmotic effect in the blood • Contraindicated in pulmonary edema, Cardiac edema (CHF) and intracranial hemorrage, established renal failure 2) Thrombophlebitis 3) Headache (due to hyponatremia), Nausea 4) If overdose dehydration hypernatremia Monitoring of urine output, S. electrolytes, CVP is very imp. Step 6 of rational pharmacotherapy Potassium Sparing Diuretics - Site of Action Potassium sparing diuretics – MOA at cortical DT Potassium sparing diuretics: Preparations Aldosterone Antagonist Dose (mg) Route Spironolactone 25-100 oral I.V. K canrenoate Eplerenone 25-100 oral Amiloride 5 Oral, Aerosol Triamterene 50 oral Directly Acting Fixed dose combinations with thiazides and frusemide available but not advisable Spironolactone - Actions • Acts on cortical segment of distal tubules • Competitive antagonist of Aldosterone • Inhibit AIP inhibit Na reabsorption • Causes K’ retention (K sparing effect) Hyperkalemia • Mild saluretic (natriuresis) 3% of NaCl • Never used alone as diuretic • Useful when combined with thiazide or frusemide Spironolactone - Pharmacokinetics • Given orally microfine powder tab. • Bioavailability 75% • Converted to active metabolite canrenone • K canrenoate is water soluble can be given I.V. gets converted to canrenone • Onset of action is very slow (steroid receptors) Spironolactone - uses 1) Edema more useful in cirrhotic and nephrotic syndrome breaks resistance to thiazides or frusemide in refractory edema 2) To counteract K loss due to thiazides, frusemide 3) Hypertension: combined with thiazide 4) Eplerenone is a new drug approved for HT, No gynaecomastia CHF: as a adjunctive therapy it retards disease progression and reduces mortality – 5) RALES (Randomized ALdosterone Evaluation Study) Primary Hyperaldosteronism (Conn’s syndrome) Spironolactone – Adverse Effects 1) Hyperkalemia risk • In CRF patients • Patients taking ACEI (Enalapril) or ATRA (Losartan) • KCl supplement 2) Related to steroid structure • Gynaecomastia, Impotence in males • Hirsutism, menstrual irregualarities in females 3) Misc: drowsiness, abdominal upset 4) Drug Interactions • may increase digoxin levels in CHF • NSAIDs (Aspirin) decreases its effect Amiloride & Triamterene - Actions • Direct action on DT and CD • Amiloride sensitive or renal epithelial Na channels are blocked • Weak diuretic never used alone • Indirectly inhibit K+ secretion • Also inhibit H+ secretion • Amiloride in aerosol form cystic fibrosis • ADRs, precautions similar to spironolactone but does not cause sexual dysfunction Refractory Edema & Diuretic Resistance Causes Management • Decreased access Salt restriction Bed rest • Binding to proteins Omit NSAIDs • 2ndary hyperaldosteronism Multiple doses • Delayed absorption Metolazone • Nephron hypertrophy Spironolactone Combination of diuretics Thiazide + Frusemide Exercises on 2nd Lecture Question Fastest Finger First Q . Arrange the following diuretics according to their site of action starting from proximal to distal parts of the nephron. A. Triamterene B. Hydrochlorothiazide C. Acetazolamide D. Bumetanide Answer: C D B A Prescription - Criticize and Correct Prescription given to patient suffering from chronic congestive heart failure with hypertension with edema feet and basal crepts in the chest Rx Tab. Enalapril 20 mg twice daily Tab. Digoxin 0.25 mg once a day Inj. Hydrochlorothiazide 5 mg IV once a day Tab. Spironolactone 50 mg twice daily MCQ – Case Study type A patient with long standing diabetic renal disease and hyperkalemia and recent onset congestive heart failure requires a diuretic. Which of the following would be LEAST harmful in a patient with severe hyperkalemia A. Amiloride B. Hydrochlorothiazide C. Spironolactone D. Losartan Answer B MCQ – Effects of thiazides When used chronically to treat hypertension, thiazide diuretics have all of the following properties or effects EXCEPT A. reduce blood volume or vascular resistance or both B. have maximal effects on blood pressure at doses below maximum diuretic dose C. may cause elevation of plasma triglyceride levels D. decrease the urinary excretion of calcium E. cause ototoxicity Answer E MCQ – Matching type One of the following diuretic is NOT properly matched with its indication for use A. Hydrochlorothiazide – Diabetes insipidus B. Eplerenone – Hypertension C. Mannitol – Acute pulmonary edema D. Spironolactone – Edema in cirrhosis of liver Answer C True or False 1. Amiloride is a drug of choice for lithium induced nephrogenic diabetes insipidus 2. Mannitol is contraindicated in barbiturate poisoning 3. Spironolactone can be given intravenously 4. Diuretics should be avoided in pregnancy induced hypertension 5. Metolazone is useful even when GFR is very low Answer T F F T T End of diuretic lectures. Any Questions?