Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Remote ischemic conditioning wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
History of invasive and interventional cardiology wikipedia , lookup
Drug-eluting stent wikipedia , lookup
Coronary artery disease wikipedia , lookup
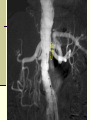
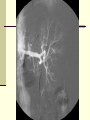
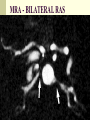
Renal Vascular Disease & HTN Mark D. Purcell DO Nephrology/Internal Medicine Carolina Nephrology, PA 203 Mills Avenue Greenville, SC 29605 (864) 271-1844 [email protected] Hypertension and the Kidney The Kidney and Hypertension Chicken or the Egg? Overview – Secondary Hypertension HTN affects >50 million adults in US 95% - Essential HTN 5-10% - “ Secondary” HTN Potentially curable disease Often overlooked / under screened – OSA and Hyperaldosteronism Controversy over screening and treatment Expensive, index of clinical suspicion and knowledge of limitations of different tests Suspect Secondary Hypertension General principles: New onset HTN if <30 or >50 years of age HTN refractory to medical Rx (>3-4 meds) Specific clinical/lab features typical for diagnosis Hypokalemia, epigastric bruits, differential BP in arms, episodic HTN/flushing/palpitations Features of OSA (Obstructive Sleep Apnoea) OTC, Steroids, Licorice etc RESISTANT HYPERTENSION Definition BP > 140/90 mm of Hg on at-least three anti–hypertensive medications (one diuretic) Prevalence - 10% Clinical conditions: Non-compliance Sub-optimal doses White coat effect Exogenous substances (cocaine) Secondary causes Causes of Secondary HTN Common Intrinsic Renal Disease Retention of salt Uncommon Pheochromocytoma Glucocorticoid excess/ Cushing’s disease Coarctation of Aorta Hyper/hypothyroidism Renovascular Disease RAAS Renal a. stenosis Mineralocorticoid excess Aldosteronism OSA (Obst. Sleep apnea) Sympathetic overactivity Hypertensive Nephrosclerosis? Moser M and Setaro J. NEJM 2006;355:385-392 Kidney Disease in Hypertension A Historical Perspective Ludwig Traube (Berlin, 1856) “High BP Necessary” … arterial pressure was elevated to overcome mechanical resistance … through thickened arteries. … increased BP pressure was necessary for excretory efficiency. … concepts which were unchallenged … Page (Cleveland, 1934) “High BP Not Required for Kidney Function” Developed kidney clearance techniques that estimated kidney blood flow in humans. Reduced elevated BP without a fall in urea clearance. Radical sympathectomy in essential & malignant HTN safely lowered BP w/o loss of function. Traube L. Ueber den zusammenhang von herz und nierenkrankeiten. Berlin: Hirschwald, 1856. Page IH. Effect on kidney efficiency of lowering blood pressure in cases of essential hypertension and nephritis. J Clin Invest 1934;13:909. ESRD: Incident Counts & Adjusted Rates By Primary Diagnosis 72% illi illi lla lla Incident ESRD patients. Rates adjusted for age, gender, & race. ESRD Care Only — $17.3 million USD United States Renal Data Survey, 2006 Adjusted Relative Risk for Developing ESRD Associated with BP Level BP level (mm Hg) Adjusted relative risk 95% CI <120/80 Reference — 120-129/80-84 1.62 1.27-2.07 130-139/85-89 1.98 1.55-2.52 140-159/90-99 2.59 2.07-3.25 160-179/100-109 3.86 3.00-4.96 180-209/110-119 3.88 2.82-5.34 >210/120 4.25 2.63-6.86 Pohl MD et al. J Am Soc Nephrol 2005. Available at: http://www.jasn.org. Nephrosclerosis Definition Stiff vessels from hypertension Hyaline in vessels, loss of glomeruli and tubules from microvascular ischemia Called benign to distinguish clinical course from malignant Nephrosclerosis – Target Regions Arcuate arteries Intralobular arteries Afferent arteriole Hypertensive Nephrosclerosis Two processes Loss of lumen through medial hypertrophy (growth) and intimal thickening (encroachment) Deposition and accumulation of hyaline material (protein in origin, eg, C3b) in vessel wall, causing further narrowing of vessel. Glomeruli Shrunken (ischemic) Benign Hypertesion Clinical Features of Nephrosclerosis Proteinuria, variable, <1 g/d Uric acid elevations more common UA bland If SCr is elevated, even minimally, the kidneys are usually small Calculate GFR Nephrosclerosis Occurs with aging Modest Accounts for most of aging-related decline of GFR Ethnic predilection African Americans Relatively younger Worse histology SCr correlates with histology Case presentation 1 41 yr old white female with no significant PMH Evaluated for kidney donation to her father Spiral CT: Single renal arteries B/L: 7-8 mm in size Reno gram:- Normal and 5/2011 – kidney donation 14 months later she presented with HTN (BP -150/100 mm of Hg) and mild renal insufficiency (creat.1.5 mg %) Date 04/07/2012 08/22/2011 08/07/2011 08/02/2011 07/25/2011 07/10/2011 07/03/2011 Time BUN CREAT mg/dL 1.1 1.1 1.1 1.4 1.3 1.4 Presented with HTN & 1.5 renal Failure 15:52 16:45 09:45 14:07 15:00 00:00 15:21 23 18 25 29 36 34 05/25/2010 05/24/2010 05/23/2010 00:05 9 00:10 11 00:10 11 1.0 1.2 1.2 04/09/2010 11:02 9 0.8 kidney Donation Differential Diagnosis ? Hypertension and Azotemia Renal parenchymal disease Ischemic renal disease Reno-vascular stenosis (single kidney) Aortic Coarctation Vasculitis (PAN) Athero-embolic disease What is next ? ANGIOGRAM OF FIBROMUSCULAR DYSPLASIA Unique features of this case Presentation: Ischemic renal disease (HTN & azotemia) ? Silent severe FMD vs. Rapid progression FMD gradient of > 120 mm of Hg) (systolic Failure to detect by CTA ? Unilateral (Recipient had no definite features of severe FMD) Fibromuscular dysplasia 10-25% of all RAS Young female, age 15-40 Medial disease 90%, often involves distal RA ~ 30% progressively worsen but total occlusion is rare Treatment – Percutaneous Transluminal Renal Angioplasty (PTRA) Successful in 82-100% of patients Restenosis in 5-11% “Cure” of HTN in ~60% Fibromuscular dysplasia Medial Fibroplasia : 70-85 % Classic “String of beads” Perimedial Fibroplasia:10-25% Small (focal) string of beads Intimal Fibroplasia: 10% Localized smooth stenosis With Post-stenotic dilatation Case presentation 2 A 72 yr old Caucasian female Recent onset of mild kidney injury and HTN Meds: Prinivil, Cardizem & third unknown agent BP 200/100 mm of Hg, SCr. 1.6 mg/dL PMH: Smoker 50 pk.yrs & Hypercholesterolemia Date 08/28/2011 08/21/2011 08/17/2011 08/17/2011 08/17/2011 08/16/2011 07/25/2011 07/24/2011 06/12/2011 05/23/2011 05/03/2011 04/26/2009 02/23/2009 Time 00:00 00:00 21:00 14:30 05:30 19:38 15:10 19:48 17:10 16:01 11:10 21:45 11:33 BUN 96 62 41 39 39 31 37 34 42 34 14 19 CREAT mg/dL 5.8 3.5 2.3 2.2 2.2 1.9 1.7 PTRA with Stent 1.6 Referral to Nephrology 2.0 1.9 1.5 1.2 0.9 Case presentation 2 Post-PTRA outcome Severe renal failure Severe HTN and CVA Patient died a week later Case presentation 3 A 72 yr old AA male, Smoker with h/o DM, HTN, CAD, Hypercholesterolemia & CRF Hytrin 5 mg QD, Lasix 80 mg BID, Vasotec 20 mg BID, Norvasc 5 mg BID, Clonidine 0.2 mg TID, Metoprolol 100 mg BID and K-Dur 20 meq TID BP 150/100 mm of Hg Sr. Creat. 1.8 –2.3 mg/dL MRA - BILATERAL RAS Case presentation 3 Bilateral renal artery stenosis PTRA with stent placement BP – 130 / 85 mm Hg on 3 anti – hypertensive drugs 2 yrs later his Sr. Creat. is 1.6 –1.7 mg/dL RENOVASCULAR HYPERTENSION (RVH) Definition of Reno-vascular Hypertension Hypertension cured or improved by reversal of stenosis Confirmation is retrospective Hypertension Reno vascular stenosis Cause and Effect Relationship CAUSES OF RVH Atherosclerotic RAS (90%) Usually ostial and associated with diseased aorta Fibromuscular dysplasia Aortorenal dissection Vasculitis involving the renal artery (i.e. PAN) AVMs involving the renal artery Irradiation of the renal artery Scleroderma Characteristics of Atherosclerotic Renal-Artery Stenosis and Fibromuscular Dysplasia. Dworkin LD, Cooper CJ. N Engl J Med 2009;361:1972-1978. PREVALENCE OF RAS Hypertensive patients PCP clinic hospital based clinic specialized HTN clinic Autopsy series >60yrs - 1% - 5% - 40% 25 - 30% Extrarenal vascular diseases 18 - 42% ASSOCIATION BETWEEN DEGREE OF STENOSIS AND HYPERTENSION DEGREE OF STENOSIS HYPERTENSION 0 –49% 46% 50 –75%% Unilateral Bilateral 78% 93% >75% Unilateral Bilateral 86% 94% Morphological stenosis may not always result in clinical HTN DIAGNOSIS OF RAS (Renal A. Stenosis) Commonest form of curable hypertension if diagnosed early Less amenable to pharmacotherapy Worse prognosis than primary hypertension Definitive therapy mandates diagnosis of RAS 4-8 % of all ESRD : Ischemic Nephropathy RVH - CLINICAL DILEMMA 1. Who should be investigated for RVH? 2. Which is the ideal screening test ? 3. What is the functional relevance of morphological stenosis ? 4. How to recognize critical RAS in timely manner ? 5. How to predict response to Renal Revascularization? RAS – Hemodynamic significance Definition for Hemodynamically significant RAS Stenosis > 75% > 50% stenosis with poststenotic dilitation Luminal stenosis between 50 –75% Peak SBP gradient of >10 % across the stenosis Mean pressure gradient > 5 % or 10 mm of Hg Resistive Index of < 80 (PSV – EDV / PSV*100) RAS – Clinical significance Morphological RAS Clinically significant BP uncontrolled on medical management Impairment of renal function Evidence of nephron loss on follow-up imaging studies Poor Quality of life – pulmonary edema or resistant HTN Decision to re-vascularize depends up on clinical significance rather than morphological or hemodynamic significance Who should be investigated for RVH? Prediction Rule for Quantifying the Probability of Renal Artery Stenosis Predicted probability of renal artery stenosis in patients with drug-resistant hypertension as a function of the sum score. SUGGESTED WORK-UP FOR RVH INDEX OF CLINICAL SUSPICION LOW (1%) NO FURTHER WORK UP - MODERATE (5-15%) CAPTOPRIL RENOGRAM CAPTOPRIL TEST RV RENINS MRA OR DUPLEX SCAN HIGH (>25%) ARTERIOGRAM + Which is the ideal screening test ? Diagnostic Imaging Tests for Renal-Artery Stenosis. Dworkin LD, Cooper CJ. N Engl J Med 2009;361:1972-1978. So some tests are inconclusive while others are expensive or have inherent risks, does it really matter to pursue RAS in today’s health care system??? Dismal Prognosis Associated with RAS 3 year mortality 26% in patients treated with stents (Circulation 1998;98:642-647) 28% in patients managed medically (Mayo Clin Proc 2000;75:437) 4 year mortality 43% in patients with RAS discovered incidentally at cardiac catheterization (Kidney International 2001;60:1490-1497) 35% in patients with RAS discovered incidentally at cardiac catheterization (JASN 1998;9:252-256) 26% in a multi-center study of patients undergoing percutaneous renal revascularization (Circulation 1998;98:642-647) 5 year mortality 33% in a single-center study of patients undergoing percutaneous renal artery revascularization (Catheter Cardiovasc Interv. 2007;69:1037) Effect of RAS on Prognosis – Relative Five year Survival 100 Survival 80 60 40 20 0 Breast Cancer RAS Colorectal Cancer Non-Hodgkins Lymphoma Ries LAG et al. SEER Cancer Statistics Review, 1973-1998. National Cancer Institute. September 2000. Clinical Events in Patients With RAS Claims data from a 5% random sample of the United States Medicare population were used to select patients without atherosclerotic renovascular disease in the 2 years preceding December 31, 1999 (N= 1,085,250), followed J Am Coll Cardiol Intv 2009;2:175-182 until December 31, 2001. INDICATIONS FOR ANGIOPLASTY IN HEMODYNAMICALLY SIGNIFICANT RAS HYPERTENSION CONTROL Reasonable likelihood of cure Refractory, accelerated or malignant HTN FMD suspected clinically Intolerant or non-compliant to medications Onset of HTN < 30 or > 60 RENAL SALVAGE Loss of renal mass or function unexplained or on medication (ACE-I or ARB) Progression of RAS under surveillance CARDIAC DISTURBANCE SYNDROME Unstable angina or flash pulmonary edema INDICATIONS FOR RENAL ARTERY STENT DEPLOYMENT Failure to attain satisfactory angioplasty results > 30 % stenosis Persistent hemodynamically significant gradient Flow limiting Dissection Ostial stenosis – standard of care Ostial stenosis that has normal diameter of 5 mm or more (restenosis rate is higher) Re-stenosis of successful previous angioplasty CONTRAINDICATIONS FOR RENAL ARTERY STENT DEPLOYMENT Inelastic stenosis that cannot be reduced to < 50 % by angioplasty Presence of sepsis Stent would preclude surgical salvage should re-stenosis occur Stenosis of artery with 4 mm or less in diameter COMPLICATIONS OF RENAL REVASCULARIZATION Controversies in ASO –RAS management Optimal non – invasive test ACEI / ARB in Bilateral RAS Follow up protocol for Imaging in patients on medical management Medical vs. Interventional management Angioplasty and STent for Renal Artery Lesions (ASTRAL) NEJM 2009;361:1953-1962 ASTRAL Trial Substantial atherosclerotic RAS Suitable for endovascular revascularization Patient's doctor was uncertain that the patient would benefit from revascularization Revascularization (n = 403) No revascularization (n = 403) with angioplasty and/or stent (and medical treatment) Medical treatment according to local protocol PATIENT CHARACTERISTICS Revasc. Medical P-value 70 (42 – 86) 71 (43 – 88) 0.7 Male 63% 63% 0.9 Current smoker 20% 22% 0.5 Diabetes 31% 29% 0.5 CHD 49% 48% 0.2 PVD 41% 40% 0.7 40.3 (5.4 – 124.5) 39.8 (7.1 – 121.7) 0.7 Mean age (range) GFR (ml/min) Procedural Complications 38 peri-procedural complications in 31 of 359 patients (9%) who underwent revascularization 19 of these events were considered to be serious complications Pulmonary edema (1) and Myocardial infarction (1) Renal embolizations (5), Renal arterial occlusions (4) and Renal-artery perforations (4) Femoral-artery aneurysm (1) Cholesterol embolism leading to peripheral gangrene and amputation of toes or limbs (3) Blood Pressure The ASTRAL Investigators. N Engl J Med 2009;361:1953-1962. Kaplan–Meier Curves for the Time to the First Renal and Cardiovascular Events. The ASTRAL Investigators. N Engl J Med 2009;361:19531962. Kaplan–Meier Curves for Overall Survival. The ASTRAL Investigators. N Engl J Med 2009;361:1953-1962. • “An important limitation of our trial concerns the population that we studied. As noted, patients were enrolled in the trial only if their own physician was uncertain as to whether revascularization would provide a worthwhile clinical benefit.” • Patient selection (single center) – – – – 508 patients with atherosclerotic renovascular disease Of these, 283 patients had renal-artery stenosis of more than 60% 71 underwent randomization 24 underwent revascularization outside the trial • • – poorly controlled hypertension rapidly declining renal function, 188 received medical treatment only. Criticisms of ASTRAL Selection bias/ Inexperienced Operators Reduction in number of anti-HTN Rx in stent-treated patients Patients with severe RAS were not enrolled Not all patients in the intervention group had stenting High Adverse Event Rate Trial Centers were not high-volume centers Await Coral (Cardiovascular Outcomes in Renal Atherosclerotic Lesions) Where do we stand now? In the absence of trials showing benefit from revascularization over conventional therapy and the significant risk of complications it seems reasonable to restrict procedures to patients who fail medical therapy with: resistant or poorly-controlled hypertension (pts on many meds) recurrent flash pulmonary edema dialysis-dependent kidney failure resulting from renal artery stenosis chronic renal insufficiency and bilateral renal artery stenosis renal artery stenosis to a solitary functioning kidney. Agency for Healthcare Research and Quality (AHRQ) Available at www.guideline.gov Summary RAS is an unusual cause of hypertension but a common finding in patients with vascular disease RAS identifies patients with very poor prognosis and a high risk of cardiovascular events Revascularization will benefit select patients with RAS but predicting who responds favorably is challenging A better understanding of the pathophysiology of RAS is needed in order to design more effective therapies