Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
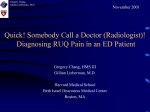
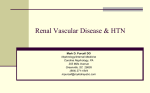
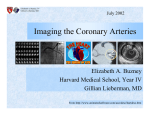
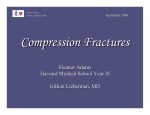
May 2001 Diagnosis of Renal Artery Stenosis (RAS) Kurt Fink, Harvard Medical School, Year III Gillian Lieberman, MD Kurt Fink, HMSIII Gillian Lieberman, MD Epidemiology Hypertension -Affects 60 million Americans Essential HTN Secondary HTN >95% of cases 1-5% of cases Renovascular HTN Other Causes: *accounts for majority of cases of secondary HTN Hyperaldosteronism Cushing's Syndrome Pheochromocytoma Aortic Coarctation 2 Kurt Fink, HMSIII Gillian Lieberman, MD Physiology of RAS Hypertension RAS RBF Renin AII Efferent Arteriolar Vasoconstriction Key: RBF=Renal Blood Flow Maintains GFR!! If this compensatory mechanism fails, patient will experience renal failure!! AII=Angiotensin II GFR=Glomerular Filtration Rate 3 Kurt Fink, HMSIII Gillian Lieberman, MD Clinical Presentation of RAS • • • • • • Onset of HTN in patient >60 or <20 y.o. Acute rise in B.P. above stable baseline Acute elevation in plasma creatinine Abdominal bruit Atherosclerotic disease (PVD, CAD) Unilateral small kidney (<9cm) Patients presenting with any of the above findings warrant further evaluation for RAS… 4 Kurt Fink, HMSIII Gillian Lieberman, MD Major Forms of RAS 1) Atherosclerotic Accounts for 90% of cases of RAS Often associated with diffuse atherosclerotic disease Usually involves ostium and proximal 1/3 of renal artery Progressive: unilateral bilateral 2) Fibromuscular Dysplasia Classically seen in young women Etiology unknown Can affect intima, media or adventitia of vessel Involves distal 2/3 of renal artery and segmental branches Aneurysmal appearance on angiography 5 Kurt Fink, HMSIII Gillian Lieberman, MD Anatomy Medulla (pyramids) Main Renal Artery Minor Calices Cortex Segmental Arteries Interlobar Arteries Netter FH. Atlas of Human Anatomy. New Jersey, Novartis, 1997, p. 315. 6 Kurt Fink, HMSIII Gillian Lieberman, MD “Patient E.O.” • 90 y.o. woman with a h/o CAD, CHF, HTN and hypercholesterolemia • Over a period of 6 months, her previously wellcontrolled HTN has progressed and is currently refractory to treatment with maximum dosages of 4 antihypertensive medications • Additionally, during this time, her Creatinine has increased to 1.5 from a baseline of 1.0-1.2 • No Abdominal bruit was detected on examination 7 Kurt Fink, HMSIII Gillian Lieberman, MD Work-up of suspected RAS Menu of tests Invasive Conventional Angiography Non-Invasive MR Angiography Renal Scintigraphy Doppler Ultrasound 8 Kurt Fink, HMSIII Gillian Lieberman, MD MR Angiogram (MRA) General 3-D anatomic reconstruction using MRI Sensitivity=100%; Specificity=96% Advantages Excellent anatomic visualization (especially w/ gadolinium) Non-invasive, no contrast, no ionizing radiation Disadvantages Costly Limited availability Claustrophobia 9 Kurt Fink, HMSIII Gillian Lieberman, MD MRA of Patient E.O. Stenosis of Left Renal Artery Stenosis of Right Renal Artery PACS, BIDMC. PACS, BIDMC. MRA clearly demonstrates bilateral stenosis of proximal Renal Arteries 10 Kurt Fink, HMSIII Gillian Lieberman, MD MRA of Another Patient Celiac Trunk Superior Mesenteric Artery Right Renal Artery Enlargement of Infrarenal Aorta (~4.2cm) Left Renal Artery with focal stenotic lesion PACS, BIDMC. Click for 3-D Animation and Labels! 11 Kurt Fink, HMSIII Gillian Lieberman, MD Renal Scintigraphy General Assesses differential renal blood flow using Tc99m-MAG3, a compound that is NOT filtered, but IS secreted. PPV=85%; NPV=90% (in high risk patients) Advantages Most Funtional Study Preferred method in suspected Fibromuscular Dysplasia Non-invasive, no contrast Disadvantages Poor at detecting Bilateral RAS Not as useful in elderly, as their HTN tends not to be renin-dependent Poor NPV Some exposure to radioactivity 12 Kurt Fink, HMSIII Gillian Lieberman, MD Renal Scintigraphy • This is a pre ACE Inhibitor renal scan of a patient with RAS. Notice that uptake and excretion of Tc99-MAG3 is symmetrical in the two kidneys. Thus, this patient is well-compensated and is able to maintain GFR. Courtesy of Mallinckrodt Institute of Radiology, Washington University, http://gamma.wustl.edu/rs001te187.html. Hypertension RAS RBF Renin AII Efferent Arteriolar Vasoconstriction Maintains GFR!! 13 Kurt Fink, HMSIII Gillian Lieberman, MD Renal Scintigraphy •After administration of an ACE Inhibitor, notice that the right kidney (on your right-hand side! As these are posterior views) has normal uptake and excretion, while the left kidney demonstrates significant retention of Tc99MAG3, with impaired excretion. This implies a drop in GFR in the left kidney, and is a positive test for RAS. Courtesy of Mallinckrodt Institute of Radiology, Washington University, http://gamma.wustl.edu/rs001te187.html. Hypertension RAS RBF Renin AII Effects of ACE Inhibitor... Efferent Arteriolar Vasoconstriction Drop in GFR!! 14 Kurt Fink, HMSIII Gillian Lieberman, MD Renal Scintigraphy in action... Post ACE Inhibitor Courtesy of Dr. Donohoe, BIDMC. • Again, notice that there is marked asymmetry in function between the two kidneys, with normal uptake and excretion by the right kidney, but significant retention of radiolabeled MAG3 by the left kidney, with little or no excretion. Once again, this is a positive scan for RAS of the left renal artery. 15 Kurt Fink, HMSIII Gillian Lieberman, MD Doppler Ultrasound General Evaluates post-stenotic, intra-renal vessels for alterations in normal renal waveforms PPV=99%; NPV=97% (in high risk patients) Advantages Funtional & Anatomic Inexpensive Non-invasive, no contrast, no ionizing radiation Disadvantages Time-consuming (often >1-2 hours) Highly operator-dependant Limited by obesity and bowel gas 16 Kurt Fink, HMSIII Gillian Lieberman, MD Doppler Ultrasound of Renal Arteries Right Renal Artery Abdominal Aorta Radiologic Clinics of North America 1996; 5: 1017-1036. Left Renal Artery 17 Kurt Fink, HMSIII Gillian Lieberman, MD Doppler Ultrasound Waveforms Normal waveforms Radiologic Clinics of North America 1996; 5: 1017-1036. Rapid upstroke & early systolic peak (arrow) RAS waveforms Radiologic Clinics of North America 1996; 5: 1017-1036. “Tardus & Parvus” waveform, i.e. slowed uptroke and low amplitude peak Quantitative characterization of waveforms has not proven to be more sensitive 18 than “pattern recognition” in doppler ultrasound detection of RAS. Kurt Fink, HMSIII Gillian Lieberman, MD Conventional Angiography General Gold Standard “Digital Subtraction” angiography has allowed for use of decreased volume of contrast Advantages Anatomic Allows for immediate intervention (PTCA/stent) Disadvantages Invasive Iodinated contrast can be nephrotoxic in patients with renal failure! Exposure to ionizing radiation 19 Kurt Fink, HMSIII Gillian Lieberman, MD …Back to our Patient “E.O.”: • Given her clinical scenario of worsening HTN and renal function, along with the finding of bilateral RAS on MRA, the decision was made to proceed to Angiography for further imaging and possible intervention. 20 Kurt Fink, HMSIII Gillian Lieberman, MD EO: Digital Subtraction Angiography Collateral vessels • A catheter is advanced through E.O.’s Left Femoral Artery into the upper Abdominal Aorta • Contrast is injected, allowing for visualization of anatomy of Aorta, Renal Arteries, etc. • Digital Subtraction involves “subtracting” an initial scout image (no contrast) from the aortogram, providing enhanced vascular detail Bilateral Stenosis of Renal Arteries PACS, BIDMC. 21 Kurt Fink, HMSIII Gillian Lieberman, MD EO: Angioplasty • This fluoroscopic image shows the positioning of a guidewire in a segmental renal artery • Contrast in collecting system • Black dots represent proximal and distal ends of angioplasty balloon on catheter that has been advanced over guidewire into left renal artery PACS, BIDMC. 22 Kurt Fink, HMSIII Gillian Lieberman, MD EO: Angioplasty • Injection of contrast allows for visualization of angioplasty balloon in relation to stenotic lesion • 3 and 5 mm angioplasty balloons are then serially inflated • A Corinthian stent, mounted on a 5 mm balloon, was then positioned and inflated PACS, BIDMC. 23 Kurt Fink, HMSIII Gillian Lieberman, MD EO: Stent Placement Stent PACS, BIDMC. 24 Kurt Fink, HMSIII Gillian Lieberman, MD EO: S/P Stent Placement • Upon injection of contrast, correction of stenosis is confirmed visually • In addition, pre- and post-procedure pressure measurements are compared: Aortic Pressure = 159/49 Post Stenosis L. Renal Artery Pressure: Prior to PTCA/Stent = 43/31 After PTCA/Stent = 172/55 • Similar stenting was carried out in the R. Renal Artery PACS, BIDMC. • Post-op, E.O. experienced return of both BP and Creatinine to her previous baseline 25 Kurt Fink, HMSIII Gillian Lieberman, MD Patient 2: Characteristic Angiographic appearance of Fibromuscular Dysplasia • Beaded, aneurysmal appearance of distal Right Renal Artery in a young woman with refractory HTN and Fibromuscular Dysplasia N Engl J Med 2001; 344: 431-442. 26 Kurt Fink, HMSIII Gillian Lieberman, MD Algorithm & Summary • This figure represents one author’s algorithm for the evaluation of suspected RAS. However, as you have gathered from Patient E.O., there is considerable variability involved in how suspected cases of RAS are workedup by various physicians, reflecting the controversy of the field. 27 N Engl J Med 2001; 344: 431-442. Kurt Fink, HMSIII Gillian Lieberman, MD References • Dustan HP. Renal Arterial Disease and Hypertension. Medical Clinics of North America 1997; 5: 1199-1212. • Harbert JC, Eckelman WC, Neumann RD. Nuclear Medicine: Diagnosis and Therapy. New York, Thieme Medical Publishers, Inc., 1996, p. 713-724. • Kaplan NM, Rose BD. Screening for Renovascular Hypertension. UpToDate.com 2001. • Mitty HA et al. Renovascular Hypertension. Radiologic Clinics of North America 1996; 5: 1017-1036. • Netter FH. Atlas of Human Anatomy. New Jersey, Novartis, 1997, p. 315. • Safian RD, Textor SC. Renal Artery Stenosis. N Engl J Med 2001; 344: 431-442. 28 Kurt Fink, HMSIII Gillian Lieberman, MD Acknowledgements • Thanks to our Webmasters Larry Barbaras and Cara Lyn D’amour! • Special thanks to Dr. Reddy, Dr. Donohoe and Dr. Matthew Spencer for their valuable input and images! 29