Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Polyclonal B cell response wikipedia , lookup
Inflammation wikipedia , lookup
Gluten immunochemistry wikipedia , lookup
Adaptive immune system wikipedia , lookup
Immune system wikipedia , lookup
Immunosuppressive drug wikipedia , lookup
Hygiene hypothesis wikipedia , lookup
Pathophysiology of multiple sclerosis wikipedia , lookup
Molecular mimicry wikipedia , lookup
Adoptive cell transfer wikipedia , lookup
Sjögren syndrome wikipedia , lookup
Cancer immunotherapy wikipedia , lookup
Psychoneuroimmunology wikipedia , lookup
Antimicrobial peptides wikipedia , lookup
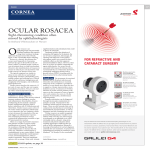
© 2007 Nature Publishing Group http://www.nature.com/naturemedicine NEWS AND VIEWS cytokines8. But there is also a similarity between IL-15 and high mobility group box-1 protein (HMGB-1), which is a transcriptional activator of proinflammatory cytokines in macrophages, especially in the setting of CLP-induced sepsis9. Like IL-15, HMGB-1 is secreted by macrophages, after which it interacts with an unidentified receptor on these cells to induce production of proinflammatory cytokines. As such, both IL-15 and HMGB-1 act intracellularly as well as extracellularly. The Orinska et al.5 study echoes other studies in which similar improvement in survival from CLP-induced sepsis was observed when cysteine protease dipeptidyl peptidase1 (ref. 10) or Smad3 (ref. 11) were genetically removed from mast cells. These data might lead one to conclude that some products of mast cells weaken the protective response to CLP-induced sepsis; as the present study indicates, intracellular IL-15 represses production of protective factors in mast cells. It is likely that mast cells can contribute either negatively or positively to defenses in sepsis, depending on the interplay between complex intracellular events. In the IL-15–deficient mice, the other features of sepsis seemed to be unaffected. For instance, the high levels of proinflammatory cytokines induced by CLP seemed to be largely unaltered, at least as assessed with peritoneal fluids5. The authors infer that the cytokine content in peritoneal fluids reflects the cytokine content in blood, but this assumption should be validated in future studies. Also, a matter of considerable debate is whether the abundance of proinflammatory cytokines during sepsis is linked to unfavorable outcomes, or whether their presence simply means that sepsis has compromised cytokine homeostasis. The data presented by Orinska et al. could suggest that the latter case is true5. There are several important unresolved issues regarding the role of IL-15 in sepsis. First, because IL-15 can be synthesized in a variety of cells, it is possible that IL-15– deficient mice are protected from sepsis through mechanisms involving these other cell types. Second, the balance between the immune and the inflammatory responses in IL-15–deficient mice should be investigated further. Finally, perhaps the information from the current study can be used to therapeutic advantage in treating sepsis in humans. It seems possible that reduced expression of IL-15 would induce neutrophil chemoattractants, presenting a potential treatment strategy for sepsis. The report from Orinska et al.5 provides us with useful information about the complex series of events unfolding during sepsis, and suggests that IL-15 might represent a target for clinical intervention. COMPETING INTERESTS STATEMENT The author declares no competing financial interests. 1. Angus, D.C. et al. Crit. Care Med. 29, 1303–1310 (2001). 2. Martin, G.S., Mannino, D.M., Eaton, S. & Moss, M. N. Engl. J. Med. 348, 1546–1554 (2003). 3. Echtenacher, B., Mannel, D.N. & Hultner, L. Nature 381, 75–77 (1996). 4. Remick, D.G., Newcomb, D.E., Bolgos, G.L. & Call, D.R. Shock 13, 110–116 (2000). 5. Orinska, Z. et al. Nat. Med. 13, 927–934 (2007). 6. Ohteki, T. Curr. Mol. Med. 2, 371–380 (2002). 7. Hiromatsu, T. et al. J. Infect. Dis. 187, 1442–1451 (2003). 8. Mulligan, M.S., Jones, M.L., Vaporciyan, A.A., Howard, M.C. & Ward, P.A. J. Immunol. 151, 5666– 5674 (1993). 9. Lotze, M.T. & Tracey, K.J. Nat. Rev. Immunol. 5, 331– 342 (2005). 10. Mallen-St Clair, J., Pham, C.T., Villalta, S.A., Caughey, G.H. & Wolters, P.J. J. Clin. Invest. 113, 628–634 (2004). 11. Kanamaru, Y. et al. J. Immunol. 174, 4193–4197 (2005). Rosacea: skin innate immunity gone awry? Charles L Bevins & Fu-Tong Liu Rosacea is a common skin disorder marked by chronic inflammation and vascular abnormalities. Two new features of the skin lesions have been identified: elevated levels of cathelicidin antimicrobial peptides and of a related serine protease. These molecules of innate immunity may represent key elements of pathogenesis, as well as new targets for effective therapies (pages 975–981). Attractive new hypotheses about the pathogenesis of idiopathic clinical disorders provide exciting opportunities for the development of novel therapies and new hope for affected individuals. Rosacea is a common chronic skin disorder often characterized by persistent erythema (redness) accompanied by visible blood vessels across the central portion of the face. Called the ‘curse of Charles L. Bevins is in the Departments of Microbiology and Immunology, School of Medicine, and Graduate Group in Immunology, University of California, Davis, California 95616, USA; Fu-Tong Liu is in the Department of Dermatology, School of Medicine, and Graduate Group in Immunology, University of California, Sacramento, California 95817, USA. e-mail: [email protected] or [email protected] 904 the Celts’, rosacea typically affects those of northern European descent, but its etiology is unclear1. The most cited theory links this disorder to abnormal cutaneous vasculature2. Dilated blood vessels feature prominently in the affected skin, which explains the persistent erythema3. On the other hand, as in acne, microbes and their associated immune responses are often implicated in the possible pathogenesis of rosacea2,4. In this issue of Nature Medicine, Yamasaki et al. show that high levels of an antimicrobial peptide and its processing serine protease are features of rosacea lesions, which suggests that aberrant innate immunity is central to this disease5. Cathelicidins, a major family of antimicrobial peptides in mammals and in other vertebrates, are expressed in leukocytes and in the epithelial cells of many tissues, where they play key roles in innate immune responses6,7. In addition to their function as endogenous antibiotics, cathelicidins are also signaling molecules, coordinating local vascular function, leukocyte migration and wound healing responses (Fig. 1a). Human cathelicidin begins as an 18-kDa precursor molecule that is cleaved into an N-terminal propeptide of approximately 100 amino acids and a C-terminal antimicrobial peptide, LL-37, named for the two leucines that comprise its first two N-terminal residues and its length of 37 amino acids. Depending on the tissue, specific serine proteases process cathelicidin to liberate active peptides, including stratum corneum tryptic enzyme (SCTE, also known as kallikrein 5) in the skin. Cathelicidin expression correlates with effective antibacterial defense in skin tissue in dermatological disorders such as psoriasis VOLUME 13 | NUMBER 8 | AUGUST 2007 NATURE MEDICINE and atopic dermatitis8. For example, in psoriatic lesions, LL-37 and other antimicrobial peptides are upregulated, and secondary infection is rare. By contrast, in atopic dermatitis the expression of these antimicrobial peptides is dampened and skin infection is more common8. In light of these facts, and knowing that the downstream effects of cathelicidin signaling mimic some features of rosacea, Yamasaki et al. proposed that abnormal expression of cathelicidin may be a salient component of this disease5. Yamasaki et al. found that cathelicidin expression is significantly elevated in rosaceaaffected skin as compared to healthy skin5. Additionally, the rosacea samples contained several additional cathelicidin processing isoforms, creating a rosacea-specific peptide profile. Two of the rosacea-specific peptides, but not a peptide found in normal skin, induced the release of the pro-inflammatory cytokine interleukin (IL)-8 from cultured human keratinocytes. What’s more, when the two rosacea-associated peptides were injected subcutaneously in mice in amounts similar to those seen in lesions, they induced erythema, vascular dilation and cutaneous inflammation. These results suggested that high expression and abnormal processing of cathelicidin might underlie the inflammation associated with rosacea. Yamasaki et al. also detected high levels of the dermal processing serine protease SCTE in rosacea lesions, suggesting that the elevated activity of this enzyme generated the rosacea-specific peptide profile. To test this, the authors performed a series of experiments to raise SCTE levels and to determine the resulting inflammatory response. Subcutaneous injection of SCTE at concentrations similar to those found in rosacea lesions caused erythema and cutaneous inflammation, and generated a peptide profile from the endogenous mouse cathelicidin precursor that resembled the rosacea-specific profile observed in the human clinical samples. Inactivated SCTE did not show this proteolytic activity, and cathelicidin-deficient mice had markedly reduced SCTE-induced cutaneous pathology. Together, these findings provide strong evidence that the elevated levels of SCTE and cathelicidin peptides found in rosacea-affected skin contribute to the chronic inflammatory response that characterizes rosacea skin lesions (Fig. 1b). One question that remains is why cathelicidin and SCTE levels are elevated in rosacea and, in particular, whether this occurs in response to specific triggers. Unlike in acne, no microorganism has been firmly associated with rosacea, but a b Normal Cathelicidin precursor Cathelicidin precursor Normal SCTE-mediated processing LL-37 Chemotactic Rosacea SCTE LL-37 and variant peptides Angiogenic Bactericidal Proinflammatory activities Effective innate immunity Chronic inflammation Katie Ris-Vicari © 2007 Nature Publishing Group http://www.nature.com/naturemedicine NEWS AND VIEWS Figure 1 Rosacea and proteolytic processing of cathelicidin peptides. (a) Cathelicidin peptides in normal cutaneous innate immunity. Cathelicidin is initially expressed as a propeptide that requires proteolytic processing to generate biologically active LL-37 peptide. In the skin, processing is mediated by stratum corneum tryptic enzyme (SCTE). LL-37 contributes to effective innate immunity through its bactericidal, chemotactic, angiogenic and other biological activities. (b) A model for cathelicidin peptides in rosacea. Yamasaki et al. show that expression of cathelicidin and its proteolytic processing enzyme, SCTE, is significantly elevated in rosacea. Increased expression of the biologically active LL-37 and several unusual processing isoforms is detected in rosacea lesions. The proinflammatory (chemotactic and angiogenic) activities of these processed peptides are central to the chronic inflammatory changes of rosacea, according to the new model proposed by Yamasaki et al. a cutaneous mite of the genus Demodex has been implicated2. These tiny creatures can be found in the skin of most healthy adults, but their numbers are significantly higher in rosaceaaffected skin1,2. It is possible that Demodex influences the expression levels and the processing of cathelicidin. House dust mites, for example, have enzymes that can cleave human proteins and activate host protease-activated receptors (PARs). PARs induce both the expression of antimicrobial peptides9 and the upregulation of proinflammatory cytokines in epithelial cells10. Perhaps Demodex activates PARs in the skin, promoting both cathelicidin induction and inflammation. Alternatively, the larger numbers of Demodex mites on rosacea-affected skin may be a result, rather than the cause, of abnormal cathelicidin processing. As Yamasaki et al. point out, the change in the local antimicrobial peptide expression profile may influence the population of commensal microbes, including Demodex, in rosacea-affected skin, which may in turn contribute to the inflammatory response. The cathelicidin peptides also regulate blood vessels, and this study therefore offers insight into the vascular phenotypes associated with rosacea. For example, LL-37 can induce angiogenesis through a direct, receptor-mediated effect on endothelial cells11. Yamasaki et al. noted that injection of LL-37 into the skin caused erythema and vascular dilation, together with the influx of inflammatory cells. Whether the vascular NATURE MEDICINE VOLUME 13 | NUMBER 8 | AUGUST 2007 response precedes or follows the inflammatory response remains to be determined. Finally, the findings by Yamasaki et al. suggest that therapeutic agents targeting cathelicidin peptides or SCTE could be useful for the treatment of rosacea. Although a number of treatments exist, many of rosacea’s clinical features, especially the persistent erythema, are difficult to remedy. Interestingly, tetracycline is one of the most commonly used treatments for this disease and, in addition to its antibiotic activity, this drug can inhibit metalloproteases12. Perhaps tetracycline lowers proinflammatory cathelicidin peptide levels by inhibiting metalloprotease activity in skin or by indirectly affecting SCTE. Direct measurement of LL-37 before and after tetracycline treatment could test this possible connection. Based on the new data, it will also be interesting to determine whether topical application of serine protease inhibitors could treat rosacea lesions. Additionally, because the innate immune system may be compromised in rosacea lesions, new antimicrobial therapies may be effective in eradicating microbes that might contribute to the disease. COMPETING INTERESTS STATEMENT The authors declare no competing financial interests. 1. Buechner, S.A. Dermatology 210, 100–108 (2005). 2. Crawford, G.H., Pelle, M.T. & James, W.D. J. Am. Acad. Dermatol. 51, 327–341 (2004). 3. Neumann, E. & Frithz, A. Int. J. Dermatol. 37, 263–266 (1998). 4. Fredricks, D.N. J. Investig. Dermatol. Symp. Proc. 6, 167–169 (2001). 5. Yamasaki, K. et al. Nat. Med. 13, 975–981 (2007). 905 NEWS AND VIEWS 6. Nizet, V. et al. Nature 414, 454–457 (2001). 7. Zanetti, M. Curr. Issues Mol. Biol. 7, 179–196 (2005). 8. Ong, P.Y. et al. N. Engl. J. Med. 347, 1151–1160 (2002). 9. Chung, W.O., Hansen, S.R., Rao, D. & Dale, B.A. J. Immunol. 173, 5165–5170 (2004). 10. Asokananthan, N. et al. J. Immunol. 169, 4572–4578 (2002). 11. Brown, A. et al. Am. J. Respir. Cell Mol. Biol. 29, 381– 389 (2003). 12. Koczulla, R. et al. J. Clin. Invest. 111, 1665–1672 (2003). 13. Acharya, M.R., Venitz, J., Figg, W.D. & Sparreboom, A. Drug Resist. Updat. 7, 195–208 (2004). David A Thorley-Lawson & Karen A Duca The role of microbial pathogens in human cancer is a fertile area of research, with important implications for treatment. Two pathogens implicated in Burkitt’s lymphoma have now been shown to directly interact with one another. Some microbial pathogens are known to play a role in the development of human cancers; topping the list are agents such as Helicobater pylori (gastric carcinoma), human papilloma virus (cervical carcinoma) and hepatitis B virus (hepatocellular carcinoma). But the granddaddy of them all is Epstein-Barr virus (EBV), which was discovered in the endemic form of Burkitt’s lymphoma (eBL) about 40 years ago. Interestingly, the virus was discovered thanks to studies on a different pathogen—malaria. It is now generally accepted that both malaria and EBV are concurrent risk factors for eBL. In a recent study in PLoS Pathogens1, it has now been shown that malaria and EBV interact with one another, raising the intriguing possibility that eBL may provide another first in human cancer biology—the first human cancer known to be causally associated with two interacting pathogens. Endemic Burkitt’s lymphoma was first described almost 50 years ago2 for its unusual presentation, notably in the jaw and in the orbit of the eye. The cancer has a striking epidemiology, being mostly restricted to the tropical regions of Africa, where it is the most common childhood cancer, with an incidence of 1–20 cases per 100,000 per year. This distribution closely follows that of holoendemic Plasmodium falciparum malaria infections3, an observation that led to the original hypothesis that mosquitoes are a vector for an infectious agent that is responsible for the tumor. Searches for this agent revealed that EBV David A. Thorley-Lawson is in the Department of Pathology, Tufts University School of Medicine, 150 Harrison Avenue, Boston, Massachusetts 02111, USA. Karen A. Duca is in the Department of Biochemistry and Biotechnology, Kwame Nkrumah University of Science and Technology, Kumasi, Ghana. e-mail: [email protected] 906 was often present in the tumor cells, but this discovery was serendipitous because it was immediately realized that EBV is not spread by insect vectors. Nevertheless, the potential role of EBV in eBL lymphomagenesis appeared to be confirmed by the findings that >95% of eBLs contain the virus, and that the virus potently transforms B lymphocytes in vitro4. Malaria is now recognized as a risk factor for eBL in its own right, as both anti-malarial treatment and migration of human hosts to areas of low malarial infection reduce the risk for eBL. Chêne et al. have now shown that malaria may join forces with EBV to heighten the risk for eBL. P. falciparum is highly mitogenic for B cells5 (Fig.1). The P. falciparum erythrocyte membrane protein 1 (PfEMP1) contains a cysteine-rich inter-domain region 1α (CIDR1α) that acts as a potent activator and stimulator of B lymphocyte proliferation6. It is particularly active against memory B cells7, which, coincidentally, are where EBV persists in vivo8. Chêne et al. show that when CIDR1α bound to B cells with latent EBV, the virus reactivated and began replicating1. The authors observed this reactivation both in the EBV-infected Akata cell line and in latently infected primary B cells derived from the peripheral blood and tonsils of healthy EBV carriers. This is the first demonstration that EBV can be reactivated directly by another pathogen. Chêne et al. propose that this interaction may account for the higher viral loads of EBV found in children with malaria, which in turn is thought to be a risk factor for eBL development1. Malaria, however, is known to have general immunosuppressive effects9, and EBV is activated when the immune system is compromised10. Consequently, the increased viral loads seem more likely to arise from this immunosuppression than from the modest reactivation-related effects reported in this study5. What’s more, the observed Arnaud Chêne © 2007 Nature Publishing Group http://www.nature.com/naturemedicine Pathogens cooperate in lymphomagenesis Figure 1 Plasmodium falciparum–infected red blood cells (labeled red) bind tightly to human B lymphocytes (labeled green). This binding is mediated through P. falciparum erythrocyte membrane protein 1 (PfEMP1) produced by the parasite. If this B cell happened to contain latent EBV, the virus would be reactivated by this interaction. The left panel shows light microscopy of the same cells with the presence of the malarial parasites indicated by white arrows. Images from Chêne et al.1 increase in viral replication seems too small to constitute a risk for eBL. Individuals who are immunosuppressed experience much greater increases in viral load but do not develop eBL. How, then, could EBV and malaria promote eBL together? We would like to propose an alternative explanation. eBL has been an annoyingly uncooperative tumor for fans of the tumor virus hypothesis. EBV is found in virtually every eBL, but the viral transforming proteins are not expressed in these tumors. In another paradox, EBV is a potent transforming virus of B cells in vitro and virtually everybody is infected with it, yet most people don’t develop Burkitt’s lymphoma. This is most likely because EBV persists in memory B cells in a dormant state, during which none of the viral proteins are expressed11. When reactivated by immunosuppression, EBV is a risk factor for EBV-positive lymphoma, but the tumors, immunoblastic lymphomas, resemble in vitro–transformed cells and are a completely different tumor type from Burkitt’s lymphoma10. VOLUME 13 | NUMBER 8 | AUGUST 2007 NATURE MEDICINE