Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Panic disorder wikipedia , lookup
Dementia with Lewy bodies wikipedia , lookup
Glossary of psychiatry wikipedia , lookup
Sluggish schizophrenia wikipedia , lookup
Parkinson's disease wikipedia , lookup
Bipolar II disorder wikipedia , lookup
Antisocial personality disorder wikipedia , lookup
Conduct disorder wikipedia , lookup
Abnormal psychology wikipedia , lookup
Autism spectrum wikipedia , lookup
Alcohol withdrawal syndrome wikipedia , lookup
Generalized anxiety disorder wikipedia , lookup
Rumination syndrome wikipedia , lookup
Narcissistic personality disorder wikipedia , lookup
Depersonalization disorder wikipedia , lookup
Factitious disorder imposed on another wikipedia , lookup
Classification of mental disorders wikipedia , lookup
Spectrum disorder wikipedia , lookup
Schizoaffective disorder wikipedia , lookup
Asperger syndrome wikipedia , lookup
Diagnostic and Statistical Manual of Mental Disorders wikipedia , lookup
Child psychopathology wikipedia , lookup
Dissociative identity disorder wikipedia , lookup
Controversy surrounding psychiatry wikipedia , lookup
Conversion disorder wikipedia , lookup
Attention deficit hyperactivity disorder controversies wikipedia , lookup
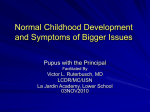
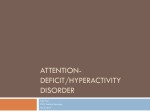
C 2004) Journal of Abnormal Child Psychology, Vol. 32, No. 5, October 2004, pp. 491–503 ( The Relation Between Sluggish Cognitive Tempo and DSM-IV ADHD1 Christie A. Hartman,2,4 Erik G. Willcutt,2 Soo Hyun Rhee,2 and Bruce F. Pennington3 Received August 28, 2003; revision received March 12, 2004; accepted March 21, 2004 To test the relation between sluggish cognitive tempo (SCT) and DSM-IV ADHD symptoms, parent and teacher ratings of the 18 DSM-IV ADHD items and five potential SCT items were obtained in a community sample of 8–18 year-old twins that was overselected for ADHD and learning disabilities (n = 296). Confirmatory factor analyses revealed that a three-factor model provided the best fit to the data for both parent and teacher ratings. DSM-IV inattention and hyperactivity–impulsivity symptoms loaded on two factors consistent with the DSM-IV model, and five SCT symptoms loaded primarily on a third factor. The SCT and inattention factors were highly correlated, whereas SCT and hyperactivity–impulsivity were weakly related. Both raters indicated that children meeting symptom criteria for the combined and inattentive subtypes exhibited significantly more SCT symptoms than those meeting symptom criteria for hyperactive–impulsive type and the comparison group without ADHD. Children meeting symptom criteria for the inattentive type exhibited significantly more SCT symptoms than those meeting criteria for the combined type, based on teacher ratings. These results suggest that SCT is an internally consistent construct that is significantly associated with DSM-IV inattention. KEY WORDS: attention-deficit/hyperactivity disorder; DSM-IV; subtypes; factor analysis; sluggish cognitive tempo. INTRODUCTION subtype describes children who exhibit significant symptoms of hyperactivity and impulsivity in the absence of significant symptoms of inattention. The combined subtype includes individuals with significant elevations on both symptom dimensions. The overall goal of this study was to examine the relation between the DSM-IV subtypes and the putative construct of sluggish cognitive tempo (SCT) as one test of the validity of the subtypes. The optimal nosology of ADHD would discriminate among meaningful subtypes to reduce the heterogeneity that has characterized previous studies (e.g., Barkley, 1998; Lahey & Willcutt, 2002; Milich, Balentine, & Lynam, 2001). If subtypes of ADHD differ consistently in their etiology, severity, or treatment response, studies that include multiple subtypes in the same group may mask effects associated primarily with one of the subtypes. In contrast, the most parsimonious taxonomy would not include subtypes that lack empirical support, as the inclusion of such subtypes tacitly reifies the validity of these subclassifications, and may therefore mislead both clinical diagnosis and research design. The diagnostic criteria for attention-deficit/hyperactivity disorder (ADHD) in the fourth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSMIV; American Psychiatric Association, 1994) define three diagnostic subtypes based on differential elevations of inattention and hyperactivity–impulsivity symptoms. The predominantly inattentive subtype includes individuals who exhibit significant symptoms of inattention and disorganization without significant hyperactivity or impulsivity, whereas the predominantly hyperactive–impulsive 1 Portions of these results were presented at the 2003 meeting of the Inter- national Society for Research in Child and Adolescent Psychopathology, Sydney, Australia. 2 Institute for Behavioral Genetics and Department of Psychology, University of Colorado at Boulder, Boulder, Colorado. 3 Department of Psychology, University of Denver, Denver, Colorado. 4 Address all correspondence to Christie Hartman, Institute for Behavioral Genetics, UCB 447, University of Colorado, Boulder, Colorado 80309-0447; e-mail: [email protected]. 491 C 2004 Springer Science+Business Media, In. 0091-0627/04/1000-0491/0 492 Some recent reviews concluded that the inattentive type is a valid subtype within the overarching DSM-IV ADHD diagnosis (e.g., Carlson, Shin, & Booth, 1999; Lahey & Willcutt, 2002; McBurnett, 1997), whereas others have suggested that the inattentive type may be a distinct attentional disorder that is not a subtype of ADHD at all (e.g., Barkley, 2001; Milich et al., 2001). Studies that compared the inattentive and combined types suggest that the combined type is associated with greater overall impairment (e.g., Faraone, Biederman, Weber, & Russell, 1998), a higher frequency of accidental injuries requiring care from a physician (e.g., Lahey et al., 1998), and greater social impairment in many domains (e.g., Gaub & Carlson, 1997), whereas individuals with the inattentive type are more likely to be socially passive or isolated (e.g., Hinshaw, 2002; Maegden & Carlson, 2000). On the other hand, available data reveal few consistent differences between the inattentive and combined types on neurocognitive tasks or measures of academic functioning (e.g., Chhabildas, Pennington, & Willcutt, 2001; Hinshaw, Carte, Sami, Treuting, & Zupan, 2002), and family and twin studies suggest that these subtypes may be attributable largely to common etiological influences (e.g., Todd et al., 2001; Willcutt, Chhabildas, & Pennington, 2001). Taken together, previous studies provide some support for the discriminant validity of the DSM-IV inattentive and combined types, but these results are inconsistent. One possible explanation for these mixed results may be heterogeneity within the group identified by the DSM-IV criteria for the inattentive type. Recent studies suggest that a subset of individuals who meet criteria for the DSM-IV inattentive type exhibit elevations of hyperactivityimpulsivity that fall only slightly below the diagnostic threshold on the hyperactivity-impulsivity symptom dimension (e.g., Barkley, 2001), whereas a second subset of individuals with the inattentive type exhibits few or no hyperactive-impulsive symptoms (e.g., Chhabildas et al., 2001; Milich et al., 2001). This heterogeneity may be exacerbated by the fact that the inattentive type is defined by the presence of a subset of the same symptoms used to define the combined type (i.e., inattention) in the absence of clinically significant elevations of hyperactivity-impulsivity. To address this concern, several authors have suggested that rather than defining a primarily inattentive subtype based on a negative diagnostic criterion such as the absence of hyperactivity, the validity of this subtype may be improved by developing positive diagnostic criteria based on additional attentional difficulties that specifically characterize this group (e.g., Carlson & Mann, 2002; Hinshaw, 2001; McBurnett, Pfiffner, & Frick, 2001; Milich et al., 2001; Willcutt et al., 2001). Hartman, Willcutt, Rhee, and Pennington Sluggish Cognitive Tempo Studies of ADHD subtypes as defined in the third edition of the DSM (DSM-III; American Psychiatric Association, 1980) revealed some differences in the specific attentional dysfunction exhibited by each of the groups. Specifically, children with DSM-III attention deficit disorder with hyperactivity exhibited inattention symptoms characterized by sloppy work and distractibility, whereas children with DSM-III attention deficit disorder without hyperactivity were rated higher on inattention items measuring daydreaming, tendency to become confused, lack of mental alertness, and physical hypoactivity (e.g., Barkley et al., 1990; Hynd et al., 1989; Lahey & Carlson, 1991; Stanford & Hynd, 1994), a cluster of symptoms that has subsequently been labeled sluggish cognitive tempo (SCT). On the basis of these findings, the DSM-IV field trials (Lahey et al., 1994) tested the utility of SCT symptoms for the diagnosis of the inattentive type. Consistent with studies of DSM-III ADD, the field trials found that SCT symptoms were associated most strongly with the DSM-IV predominantly inattentive type (Frick et al., 1994). However, further analyses indicated that the majority of individuals with the DSM-IV inattentive type did not exhibit SCT symptoms, so these symptoms were not included in the diagnostic criteria for DSM-IV ADHD. The finding that few individuals with the inattentive type exhibited SCT symptoms in the field trials suggests that these symptoms are relatively weak measures of the construct assessed by DSM-IV inattention symptoms. However, it is still possible that SCT symptoms may identify an important subgroup of individuals with DSM-IV ADHD or may even be a marker for a specific subset of individuals who meet symptom criteria for the DSM-IV inattentive type but are in fact better conceptualized as having a distinct primarily inattentive disorder. Therefore, several subsequent studies have examined the relation between ADHD and SCT symptoms and reevaluated the potential utility of SCT symptoms as part of the diagnostic criteria for ADHD (Carlson & Mann, 2002; Hinshaw et al., 2002; McBurnett et al., 2001; Skansgaard & Burns, 1998). Factor Analyses of SCT Symptoms McBurnett et al. (2001) factor analyzed parent and teacher ratings of DSM-IV ADHD symptoms plus the two SCT symptoms daydreams and sluggish/drowsy in a large clinic-referred sample. When all DSM-IV ADHD symptoms and the two SCT symptoms were included in the analysis, a two-factor solution was obtained in Sluggish Tempo and ADHD which SCT items loaded on a factor with DSM-IV inattention symptoms and DSM-IV hyperactivity-impulsivity symptoms loaded on a second factor. In contrast, when hyperactivity-impulsivity items were excluded from the analysis the inattention and SCT items separated into two factors: the first factor included all DSM-IV inattention items with the exception of often forgetful in daily activities, which loaded on a second factor along with the two SCT items. The authors then examined the potential implications of these results for the DSM-IV model of ADHD by analyzing the relation between SCT and the DSM-IV ADHD subtypes. Results of these analyses revealed that the mean severity of the SCT items was significantly higher in the group with the DSM-IV inattentive type than the combined type, hyperactive-impulsive type, or a clinic-referred comparison group without ADHD, and similar results were obtained in two studies of teacher ratings (Carlson & Mann, 2002; Skansgaard & Burns, 1998). Moreover, whereas McBurnett et al. (2001) found that the positive predictive power of the SCT symptoms was similar for the combined and inattentive types, the negative predictive power of these symptoms was substantially higher for the inattentive type. Thus, although the initial two-factor result suggests that SCT symptoms are related closely to DSMIV inattention, analyses of the inattention symptoms alone suggest that SCT symptoms may represent a separable symptom dimension that relates differentially to the inattentive and combined types. External Validity of SCT Symptoms To test the external validity of SCT symptoms, Carlson and Mann (2002) reanalyzed a large sample of nonreferred children with DSM-IV ADHD (Gaub & Carlson, 1997). They identified a subgroup (28%) of children with the inattentive type who also exhibited extreme scores on a summary measure comprised of several possible SCT items from the Child Behavior Checklist (Achenbach, 1991b). The subgroup with elevations on the SCT items was rated by teachers as showing less externalizing behavior and higher levels of unhappiness, anxiety/ depression, and withdrawn behavior than the remaining children with the DSM-IV inattentive type or combined type, as well as more social dysfunction than children with the DSM-IV inattentive type without significant SCT. In contrast to the results reported by Carlson and Mann (2002), however, another recent study found few group differences on neurocognitive measures when females with the inattentive type were subdivided into groups with and without elevations of SCT (Hinshaw et al., 2002). 493 Discriminant Validity of SCT Lahey (2001) pointed out that in addition to examining the association between ADHD and SCT, it is also essential to understand the relation between SCT symptoms and other related disorders. For example, many aspects of SCT are similar to symptoms of internalizing disorders such as major depressive disorder (e.g., drowsiness and psychomotor retardation) and generalized anxiety disorder (e.g., mind going blank), and slow processing of cognitive stimuli is also a correlate of learning disabilities and mental retardation (e.g., Stanford & Hynd, 1994; Willcutt, Pennington, et al., 2001). Because a diagnosis of an attentional disorder may be more palatable to parents than a diagnosis of major depression, it is essential that the discriminant validity of SCT symptoms be carefully demonstrated to avoid precipitating inappropriate treatment for individuals with these other disorders (e.g., Lahey, 2001). Carlson and Mann (2002) found that the inattentive groups with low and high SCT did not differ on measures of learning problems, suggesting that the relation between SCT symptoms and the inattentive type is at least partially independent of comorbid learning difficulties. However, no previous studies have examined the relation between SCT symptoms and intelligence or internalizing and externalizing psychopathology, suggesting that additional research is needed. This Study In summary, previous studies of the relation between SCT and ADHD have yielded promising but mixed results, suggesting that additional research is needed to clarify these findings. In this study, parent and teacher ratings of the 18 DSM-IV ADHD symptoms and five putative SCT items were obtained for a sample of children with and without DSM-IV ADHD. Three sets of analyses were conducted to test the relation between SCT symptoms and DSM-IV ADHD symptom dimensions and diagnostic subtypes. (1) Confirmatory factor analyses were conducted to test the fit of several competing models of the relation between DSM-IV ADHD and SCT symptoms. (2) Scores on the obtained factors were compared among groups with the DSM-IV ADHD subtypes and a comparison sample without ADHD to test if SCT symptoms are associated differentially with the DSM-IV inattentive type. (3) Finally, to address the concern that SCT symptoms may be confounded with lower intelligence, 494 Hartman, Willcutt, Rhee, and Pennington learning difficulties, or another disorder such as depression or anxiety (e.g., Lahey, 2001), we examined the phenotypic relation between parent and teacher ratings of SCT symptoms and measures of general cognitive ability, academic achievement, and internalizing and externalizing behaviors, and tested whether these correlated variables influenced the association between ADHD and SCT. METHOD Participants Recruitment Participants completed the measures described in this paper as part of their participation in the Colorado Learning Disabilities Research Center (CLDRC) twin study, an ongoing study of the etiology of learning disabilities, ADHD, and other related disorders (e.g., DeFries et al., 1997; Willcutt et al., 2003). In collaboration with 27 local school districts, parents of all twins between the ages of 8 and 18 were contacted by letter and invited to participate in the study. Approximately 35% of the families who were contacted agreed to participate in the initial screening procedure. To preserve family confidentiality until they provided informed consent, most school districts mailed the recruitment letter directly to the family so that the twins’ names would remain confidential until the family replied to our letter to indicate their interest in participating in the study. Therefore, it is not possible to compare directly the families who participated in the study to the specific families who did not respond to the initial recruitment letter. Instead, the representativeness of the sample that agreed to participate was indirectly examined by comparing the characteristics of the families who participated in the study to the demographic information for each school that is available in the public record. These comparisons indicated that the families who agreed to participate in the screening were drawn proportionally from the schools in each district, and were representative of the overall population of each district in terms of gender ratio and ethnicity. After obtaining parental consent, parents and teachers were asked to complete the Disruptive Behavior Rating Scale (Barkley & Murphy, 1998) to assess symptoms of DSM-IV ADHD. If one of the twins met symptom criteria for any DSM-IV ADHD subtype based on parent or teacher ratings, the twin pair was recruited for the larger study. In addition, twin pairs in which one twin had a history of academic difficulties were recruited independent of the procedure to ascertain the sample of twins with ADHD, and a third group of twins without ADHD or academic difficulties was recruited from the same school districts as a comparison sample. These procedures yield a community-based sample that is enriched for ADHD and learning difficulties. Approximately 95% of the families in the screening sample agreed to participate in the larger study if invited. Exclusionary Criteria After the initial screening but prior to the inception of any testing, CLDRC staff conducted an additional telephone screening interview. Because the focus of the overall project is on familial ADHD and its correlates, potential participants with a documented brain injury or other rare genetic or environmental etiology that might produce a phenotypic manifestation of ADHD were excluded from the sample. In addition, three participants were excluded from analyses because their Full Scale IQ scores were below 75. The Sample Used for This Paper The use of twins for phenotypic analyses in which each twin is considered as an individual data point presents a methodological difficulty, as the scores of the twins in each pair do not represent fully independent observations. To address this issue most conservatively, one twin was randomly selected from each twin pair in which both twins met inclusion criteria for the study. Results were virtually identical when analyses were repeated in a sample in which the selected twin was replaced by the cotwin that was excluded from the first set of analyses, suggesting that the random selection of one twin from each of these pairs did not inadvertently bias the results. A dummy code for zygosity was included in all initial models to control for any differences between participants from MZ and DZ pairs, but this code was dropped from all final models because it had no significant impact on any result. The final sample for this analyses includes all participants for whom complete data were available for parent or teacher ratings of ADHD and SCT. The SCT items were added to the battery in January, 1999, whereas the overall project has been ongoing since 1984. Therefore, the sample described in this paper is a subset of the overall CLDRC sample. After randomly selecting one twin from each pair, parent ratings were available for 286 individuals (141 males and 145 females) and teacher ratings were available for 229 individuals (119 males and 110 females). Sluggish Tempo and ADHD Although the overall sample ranged in age from 8 to 18 years, recruitment was weighted toward individuals between 8 and 13 years of age (85% of the overall sample) to facilitate follow-up analyses in a separate longitudinal component of the study. Therefore, the mean age of the present sample was 10.6 years (SD = 2.5). The pattern of results was virtually identical when each set of analyses was conducted after regressing variance associated with age out of each variable; therefore, to simplify interpretation we present results of analyses without controlling for age. The ethnicity of the participants included in these analyses (82% Caucasian, 9% Hispanic, 4% African American, 5% other ethnicity) is consistent with the ethnic breakdown of the overall CLDRC sample and the total population of students in the school districts from which the twins were recruited. Ratings on the Hollingshead 2-factor inventory (1975) indicate that the socioeconomic status (SES) of the overall sample falls near the middle of the range on this scale (M = 3.02, SD = 1.13) Measures 495 as predominantly hyperactive/impulsive type, and individuals with six or more symptoms on both dimensions were coded as combined type. Because the primary goal of this paper is to better understand the relation among the DSM-IV ADHD symptom dimensions and SCT symptoms, the DSM-IV age-of-onset and cross-situation impairment criteria were not used to assign individuals to groups for the categorical analyses. A total of 76 participants met symptom criteria for DSM-IV ADHD based on parent ratings (51 males and 25 females), and 57 individuals met symptom criteria based on teacher ratings (38 males and 19 females). Consistent with other community samples (e.g., DuPaul et al., 1998; Gaub & Carlson, 1997), the majority of participants who met symptom criteria for DSM-IV ADHD met criteria for the inattentive type (30 males and 15 females based on parent ratings, 24 males and 12 females based on teacher ratings). Most of the remaining participants met symptom criteria for the combined type (14 males and seven females based on parent ratings; seven males and five females based on teacher ratings), and a small subset met criteria for the hyperactive-impulsive type (seven males and three females based on parent ratings; seven males and two females based on teacher ratings). Symptoms of ADHD The Disruptive Behavior Rating Scale (DBRS; Barkley & Murphy, 1998) was used to obtain parent and teacher ratings of the 18 symptoms of DSM-IV ADHD. Because maternal report was available for more participants than paternal report (95% vs. 73% of the sample), maternal report was used for the analyses described in this report. Each symptom on the DBRS is rated on a four-point scale (never or rarely, sometimes, often, and very often). Previous results from this sample and others indicate that parent and teacher ratings on the DBRS or other similar scales are internally consistent (α = .92–.96) and have adequate to high test–retest reliability (r = .59– .89; e.g., DuPaul, Power, & Anastopoulos, 1998; Willcutt, Chhabildas, et al., 2001). To facilitate the assignment of participants to groups for comparisons among the DSM-IV ADHD subtypes, items rated as often or very often were scored as positive symptoms and items rated as never or rarely or sometimes were scored as negative symptoms, consistent with the procedure used in previous studies of similar rating scales (e.g., Pelham, Gnagy, Greenslade, & Milich, 1992). Individuals with six or more symptoms of inattention but fewer than six symptoms of hyperactivity-impulsivity were identified as predominantly inattentive type, participants with six or more symptoms of hyperactivity-impulsivity but fewer than six symptoms of inattention were categorized SCT Items Although several published measures include at least a few items that may reflect SCT (e.g., Achenbach, 1991a, 1991b), there is no clear consensus regarding the behaviors that best capture the construct of SCT (e.g., McBurnett et al., 2001). Therefore, an item pool of five potential SCT symptoms was developed based on items used in other studies (e.g., Achenbach, 1991; Frick et al., 1994) or created for this study, including sluggish/slow to respond, seems to be “in a fog,” drowsy or sleepy, easily confused, and daydreams/stares into space. The items daydreams and sluggish/drowsy were used in the study by McBurnett et al. (2001) and the DSM-IV field trials (e.g., Frick et al., 1994). The five SCT items were then added to the parent and teacher rating forms and administered on the same four-point scale as the DBRS. Measures of Other Psychopathology The DSM-III-R parent-report version of the Diagnostic Interview for Children and Adolescents (DICA-P; Reich & Welner, 1988) was administered to parents to assess symptoms of oppositional defiant disorder (ODD), conduct disorder (CD), generalized anxiety disorder (GAD), and major depressive disorder. The DSM-III-R 496 Hartman, Willcutt, Rhee, and Pennington version of the DICA has been maintained to allow analyses of the entire sample in the overall study. To facilitate the assessment of DSM-IV disorders, DICA modules were modified as necessary to include all DSM-IV symptom criteria. In addition to the DICA, the parent and primary classroom teacher of each participant completed the appropriate version of the Child Behavior Checklist (CBCL; Achenbach, 1991a, 1991b), a widely used measure of child and adolescent psychopathology. Broad-band internalizing and externalizing summary scores were used for this report. The externalizing score is based on the Delinquent Behavior and Aggressive Behavior scales, whereas the internalizing score includes the Somatic Complaints, Withdrawn, Anxious/Depressed scales. Neither the CBCL Attention Problems scale nor any putative SCT items used in previous studies are included in the internalizing or externalizing summary scores. Finally, each youth also completed the GAD module from the self-report version of the DICA and the Children’s Depression Inventory (CDI; Kovacs, 1988), a self-report checklist that is widely used to screen for symptoms of depression. Intelligence and Academic Achievement The revised version of the Wechsler Intelligence Scale for Children (WISC-R; Wechsler, 1974) was used to assess the Full Scale IQ (FSIQ) of participants 16 years of age or younger, and the Wechsler Adult Intelligence Scale (WAIS; Wechsler, 1981) was administered to participants who were 17 or 18 years of age. Academic achievement in reading and mathematics was assessed with the Peabody Individual Achievement Test (PIAT; Dunn & Markwardt, 1970). To simplify interpretation a reading composite score was created based on a previous discriminant function analysis of the PIAT Reading Recognition, Reading Comprehension, and Spelling subtests (DeFries, 1985). Procedures Each participant completed a detailed psychoeducational battery that included the WISC-R, PIAT, and self-report measures of internalizing disorders. While the child completed these measures their parent completed the DICA and CBCL. All interviews and tests were administered by graduate students in psychology who had experience working with children and families. Interviewers and testers were unaware of the child’s diagnostic status or the results of the other measures in the battery. Parents of participants who were taking psychostimulant medication were asked to withhold medication for 24 hr prior to each Fig. 1. Confirmatory factor analysis models. session of study to minimize the influence of medication on the results. Data Analysis Confirmatory Factor Analyses CFA was conducted to compare the fit of three nested models (Fig. 1). In all specified models each symptom loaded only on its respective latent factor, and the latent factors were allowed to correlate with one another. The first model was specified such that all DSM-IV ADHD and SCT symptoms loaded on a single factor. This model is most parsimonious, and the fit of this one-factor model can then be compared to the fit of the more complex models. A two-factor model was then fitted based on the hypothesis that SCT items are additional manifest indicators of the same latent trait measured by DSM-IV inattention symptoms. Specifically, one factor included all DSM-IV hyperactivity-impulsivity items, and the second factor included both DSM-IV inattention and SCT items. The final three-factor model retained the hyperactivity-impulsivity factor, but DSM-IV inattention symptoms and SCT symptoms were specified to load on separate factors. Sluggish Tempo and ADHD Fit Indices A first appraisal of the fit of each CFA model was obtained by examining the overall chi-square for the model, and the relative fit of each pair of competing models was compared using the chi-square difference test. This method compares the fit of two nested models by testing if the more complex model yields a significant improvement in fit (as indicated by reduction in chi-square), with degrees of freedom equal to the difference in degrees of freedom between the two models (Kline, 1998). Because chi-square values are extremely sensitive to sample size, three additional fit indices were also used to compare the relative fit of the competing models. Bentler’s Comparative Fit Index (CFI; Bentler, 1990) describes the overall proportion of variance explained by the model, with a value of .90–.95 indicating acceptable fit (Bollen and Long, 1993). Akaike’s Information Criterion (AIC; Akaike, 1987) utilizes chi-square while adjusting for model complexity; a decreasing value is desired when comparing models (Kline, 1998). Root mean square error of approximation (RMSEA; Steiger and Lind, 1980) compares the observed and expected covariances for a particular model; a value close to zero, and less than .10, is desired. The Relation Between SCT and DSM-IV ADHD Subtypes Correlations among the latent factors yielded by the CFA provided initial information regarding the relation between SCT scores and DSM-IV inattention and hyperactivity-impulsivity symptoms. To examine the relation between SCT and the DSM-IV ADHD subtypes, the mean score of the items that loaded on each factor was compared among the groups. As in other studies, the symptom ratings were positively skewed and highly kurtotic (i.e., most children scored at or near zero), and were best described by a random Poisson distribution. Therefore, planned comparisons between each pair of groups were conducted by fitting a Poisson regression model (e.g., Gardner, 1995; McCullagh & Nelder, 1983). The Relation Between SCT and Intelligence and Other Psychopathology To address the concern that SCT symptoms may simply be proxies for lower intelligence, comorbid internalizing disorders, or other variables that are typically correlated with ADHD (e.g., Lahey, 2001), we first examined the zero-order correlations between SCT symptoms and internalizing and externalizing psychopathology, reading 497 and mathematics achievement, and intelligence. Two sets of analyses were then conducted to test if parent or teacher ratings of DSM-IV ADHD symptom dimensions and subtypes were associated with elevations of SCT after controlling for the influence of these variables. The first analysis examined the partial correlation between SCT scores and DSM-IV inattention and hyperactivity-impulsivity symptoms, controlling for intelligence, academic achievement, and internalizing and externalizing symptoms. Similarly, these covariates were added to the initial Poisson regression models to test if any of the DSM-IV ADHD subtypes exhibited significant elevations of SCT symptoms when scores on the measures of psychopathology, academic achievement, and intelligence were controlled. RESULTS Confirmatory Factor Analyses Overall, confirmatory factor analyses showed that the three-factor model represented the best fit when compared to the two-factor or one-factor models (Table I). Chisquare values decreased significantly between the onefactor and two-factor models and between the two-factor and three-factor models, indicating that the three-factor model provided a significant improvement in fit over the other models. Similarly, decreasing AIC values indicated that the fit of the three-factor model was better than the fit of the two-factor or one-factor models even after accounting for increased model complexity, and the increase in CFI and decrease in RMSEA values across models provide additional evidence that the three-factor model best represents the data. These results were consistent for both parent and teacher ratings. Please see Fig. 2 for 3-factor model loadings. The Relation Between SCT and DSM-IV ADHD Symptom Dimensions and Subtypes To evaluate the implications of the present results for the DSM-IV model of ADHD, correlations among the three factors obtained from the CFA were examined. Consistent with previous studies (e.g., Chhabildas et al., 2001; DuPaul et al., 1998), the correlation between the Inattention factor score and the Hyperactivity-impulsivity factor score was high for both parent ratings (r = .73) and teacher ratings (r = .63). The correlation between the Inattention and SCT factors was similarly high (r = .75 for teacher ratings, r = .76 for parent ratings). In contrast, the correlation between the Hyperactivity-impulsivity and SCT factors was moderate for parent ratings (r = .51), and was small and nonsignificant for teacher ratings (r = .18). 498 Hartman, Willcutt, Rhee, and Pennington Table I. Confirmatory Factor Analysis of Parent and Teacher Ratings of ADHD and SCT Symptoms Fit indices Model Parent ratings 1. Single-factor model 2. Two-factor model Difference between model 1 and model 2 3. Three-factor model Difference between model 2 and model 3 Teacher ratings 1. Single-factor model 2. Two-factor model Difference between model 1 and model 2 3. Three-factor model Difference between model 2 and model 3 χ 2 (df) CFI AIC RMSEA 1296(230)∗ 854(229)∗ .75 .85 836 397 .130 .100 652(227)∗ .90 198 .083 1478(230)∗ 831(229)∗ .64 .83 1018 373 .174 .121 667(227)∗ .87 213 .104 2 (df) χdiff 442(1)∗ 202(2)∗ 647(1)∗ 164(2)∗ Note. CFI = Comparative Fit Index; AIC = Akaike’s Information Criterion; RMSEA = root mean square error of approximation. ∗ p < .0001. The CFA results also provided further support for the hypothesis that SCT symptoms are more strongly associated with symptoms of inattention than symptoms of hyperactivity-impulsivity: For both parent and teacher ratings, when the correlation between the SCT and Inattention factors was dropped from the 3-factor model, the result was a large and significant decrease in model fit (data not shown). In contrast, when the correlation between SCT and hyperactivity-impulsivity factors was dropped from the 3-factor model, the resulting decrease in fit was much smaller. Comparisons among groups with and without ADHD revealed significant differences for both parent ratings and teacher ratings of SCT symptoms (Table II). To facilitate comparison to results from other studies (e.g., McBurnett et al., 2001), the scores presented in Table II are the means of the 0–3 scale of the DBRS (not at all– very often) for the five SCT items, the nine DSM-IV inattention symptoms, and the nine DSM-IV hyperactivityimpulsivity symptoms. The pattern of results was identical when factor scores from the CFA were compared across groups. Pairwise comparisons between the groups Fig. 2. Three-factor model with loadings. Note. Top loadings and correlations are based on parent ratings, bottom loadings and correlations are based on teacher ratings. S1–S5 = Sluggish cognitive tempo items in the order listed on pg. 495, I1–I9 and H1–H9 = Inattention and Hyperactivity/Impulsivity items in the order listed in DSM-IV. Sluggish Tempo and ADHD 499 Table II. Mean Scores of Groups With and Without DSM-IV ADHD on Sluggish Cognitive Tempo and DSM-IV ADHD Symptoms Parent ratings Sluggish cognitive tempo DSM-IV Inattention DSM-IV Hyp–imp Teacher ratings Sluggish cognitive tempo DSM-IV Inattention DSM-IV Hyp-imp Comparison group without ADHD Hyperactive– impulsive type Combined type Inattentive type N = 210 0.19 (0.33)a 0.46 (0.34)a 0.38 (0.39)a N = 172 0.27 (0.43)a 0.38 (0.47)a 0.21 (0.35)a N = 10 0.30 (0.19)a 1.04 (0.33)b 1.93 (0.34)b N =9 0.34 (0.36)a 1.23 (0.37)b 1.89 (0.27)b N = 21 1.10 (0.75)b 2.36 (0.39)c 2.14 (0.36)b N = 12 0.80 (0.49)b 2.34 (0.29)c 2.16 (0.41)b N = 45 1.26 (0.65)b 2.11 (0.36)c 0.95 (0.51)c N = 36 1.35 (0.71)c 2.13 (0.32)c 0.74 (0.54)c Note. Means with different superscripts are significantly different, p < .05. indicated that both parents and teachers rated the combined and inattentive groups significantly higher on the SCT symptoms than the hyperactive-impulsive and comparison groups. The SCT mean of the inattentive group was also significantly higher than the mean of the combined type based on teacher ratings, but the inattentive and combined types were not significantly different when ratings were completed by parents. The Relation Between SCT and Other Psychopathology Many of the correlations between SCT ratings and measures of externalizing psychopathology, academic functioning, and FSIQ were significant, but the correlations were generally small in magnitude and similar to the correlations between these measures and symptom scores on the DSM-IV inattention and hyperactivity-impulsivity items (Table III). In contrast, the relation between SCT and internalizing symptoms was more variable across measures. Although correlations were small if different raters completed the measures of SCT and internalizing symptoms, correlations between SCT and internalizing ratings completed by the same individual were substantially larger. For example, the correlation between SCT and CBCL internalizing behaviors was significant for both parents (r = .52) and teachers (r = .51). Table III. Zero-Order Correlations Between Parent and Teacher Ratings of Sluggish Cognitive Tempo and DSM-IV ADHD and Measures of Psychopathology, Intelligence, and Academic Achievement Intelligence/academic achievement WISC-R full scale IQ PIAT reading PIAT math Externalizing symptoms Parent CBCL Teacher CBCL DICA-P ODD symptoms DICA-P CD symptoms Internalizing symptoms Parent CBCL Teacher CBCL DICA-P MDD symptoms DICA-P GAD symptoms DICA-C GAD symptoms CDI total score Sluggish cognitive tempo DSM-IV inattention DSM-IV hyp/imp Teacher Parent Teacher Parent Teacher Parent −.33∗ −.33∗ −.23∗ −.19∗ −.16∗ −.11 −.39∗ −.39∗ −.32∗ −.22∗ −.25 −.18∗ −.22∗ −.25∗ −.13∗ −.12 −.15∗ −.10 .25∗ .25∗ .17∗ .12 .38∗ .27∗ .30∗ .23∗ .30∗ .53∗ .22∗ .15∗ .51∗ .32∗ .35 .24∗ .33∗ .68∗ .24∗ .19∗ .64∗ .36∗ .43∗ .28∗ .21∗ .51∗ .05 −.03 .07 .10 .52∗ .24∗ .33∗ .19∗ .20∗ .33∗ .17∗ .46∗ .12 .00 .17∗ .18∗ .38∗ .29∗ .34∗ .14∗ .15∗ .24∗ .13∗ .33∗ .10 .04 .15∗ .13∗ .39∗ .26∗ .22∗ .13∗ .17∗ .12 Note. WISC-R = Wechsler Intelligence Scale for Children—Revised; PIAT = Peabody Individual Achievement Test; CBCL = Child Behavior Checklist; DICA-P = Diagnostic Interview for Children and Adolescents—Parent Report version; ODD = Oppositional Defiant Disorder; CD = Conduct Disorder; DICA-C = Diagnostic Interview for Children and Adolescents—Self-report version; MDD = Major Depressive Disorder; GAD = Generalized Anxiety Disorder; CDI = Children’s Depression Inventory. ∗ p < .05 (1-tailed). 500 Because SCT symptoms were significantly associated with these other constructs that are related to ADHD, a final set of analyses was conducted to test if the relation between ADHD and SCT remained significant after covarying scores on each of these other measures. For each analysis all measures that were significantly correlated with SCT ratings were included as covariates in the model. Partial correlations between SCT and ADHD symptoms remained significant for both parent ratings and teacher ratings of inattention (pr = .53 for parent ratings; pr = .58 for teacher ratings) and parent ratings of hyperactivityimpulsivity (pr = .26). Similarly, parent ratings of SCT symptoms remained significantly higher in the inattentive and combined types than the hyperactive-impulsive type and comparison group. In contrast, whereas the inattentive type exhibited more SCT symptoms than the other three groups based on teacher ratings, the combined type no longer differed significantly from the comparison group when the covariates were included in the model. Hartman, Willcutt, Rhee, and Pennington toms (daydreams and sluggish/drowsy) and one DSM-IV inattention symptom (forgetful) loaded on a factor separate from the other DSM-IV inattention symptoms when the inattention items were analyzed alone. In contrast, the DSM-IV inattention and SCT symptoms loaded on the same factor when DSM-IV hyperactivity-impulsivity symptoms were also included in the model. Thus, the present results provide even stronger support for the internal validity of the SCT construct, as the third SCT factor emerged even when symptoms of both DSM-IV inattention and DSM-IV hyperactivity-impulsivity were included in the analysis. Moreover, similar results were obtained for both parent and teacher ratings. Therefore, these results suggest that when a sufficient number of SCT items are included in the analysis, SCT symptoms load on a factor separate from both DSM-IV inattention and hyperactivityimpulsivity. The Relation Between SCT and DSM-IV ADHD DISCUSSION This study examined the relation between symptoms of DSM-IV ADHD and five potential symptoms of SCT in a sample of twins overselected for ADHD and learning difficulties. Confirmatory factor analyses showed that the three-factor model resulted in an improvement in fit over both a two-factor structure in which SCT items loaded on the same factor as symptoms of DSM-IV Inattention and a single-factor model in which all symptoms loaded on the same factor. The five items that loaded on the SCT factor (sluggish/slow to respond, in a fog, drowsy or sleepy, easily confused, daydreams) are strongly characterized by slow processing and hypoactivity, and appear to capture both cognitive and physiological sluggishness. Moreover, although items from the Child Behavior Checklist were not included in the final factor analyses because the items are assessed on a different scale of measurement and are somewhat redundant with the items described here, initial exploratory analyses indicated that several CBCL items (confused/in a fog, daydreams, stares blankly, overtired, and underactive/lacks energy) also generally loaded on the same factor as the five SCT symptoms described in this report. Taken together, these findings support the internal validity of the SCT construct, and suggest that the five items described here and several additional items from the CBCL may be useful manifest indicators of SCT. These results replicate and extend the results of McBurnett et al. (2001), who found that two SCT symp- SCT factor scores were highly correlated with ratings of DSM-IV inattention by both parents and teachers, and mean SCT scores were significantly higher in both DSM-IV ADHD subtypes that are characterized by significant elevations of inattention (i.e., the inattentive and combined types) than in the hyperactive-impulsive type or comparison sample without ADHD. In contrast, the correlation between SCT symptoms and DSM-IV hyperactivityimpulsivity was substantially lower for both parent and teacher ratings, and the mean SCT score of the hyperactiveimpulsive type was not significantly different from the mean of the comparison sample. These results suggest that SCT is related to DSM-IV ADHD, but primarily to the inattention symptom dimension. As noted previously, several authors have suggested that SCT symptoms might better distinguish the inattentive and combined types than the inattention symptoms included in DSM-IV (e.g., Carlson & Mann, 2002; Hinshaw, 2001; McBurnett et al., 2001; Willcutt, Chhabildas, et al., 2001). Interpretation of the present results is complicated by differences between parent and teacher ratings. Teacher ratings indicated that the inattentive type exhibited significantly more SCT symptoms than any other group, and the combined type did not differ from the comparison group when symptoms of comorbid disorders and other related variables were controlled. In contrast, parent ratings indicated that both the inattentive type and combined type exhibited significant elevations of SCT in comparison to the group without ADHD, and the means of the two subtypes were not significantly different. Sluggish Tempo and ADHD In summary, teacher ratings provide fairly strong support for the hypothesis that SCT symptoms are associated primarily with the inattentive type, whereas parent ratings suggest that SCT is associated more generally with both the inattentive and combined types. This rater difference limits the conclusions that can be drawn at this time regarding the potential utility of SCT symptoms as part of the diagnostic criteria for ADHD in DSM-V. Future studies of larger samples are needed to test further the difference between parent and teacher ratings, and to directly compare the functional and neurocognitive correlates of groups with each DSM-IV ADHD subtype with and without SCT. Until such studies are able to demonstrate that the presence of significant SCT identifies a meaningful subgroup of individuals with ADHD, it is premature to suggest that SCT symptoms be included in future diagnostic criteria for ADHD. The Relation Between SCT and Other Psychopathology In addition to those who suggest that SCT symptoms may distinguish between the inattentive and combined types, some authors have hypothesized that these symptoms might even be a marker for a new attentional disorder that is distinct from ADHD (e.g., Barkley, 2001; Carlson & Mann, 2002; Milich et al., 2001). As future research begins to evaluate this possibility, it will be essential to test not only the internal and external validity of diagnostic criteria based on elevations of SCT, but also the discriminant validity of the new disorder and other psychopathology (Lahey, 2001). Although this study provides no information regarding the diagnostic validity of a group defined based on elevations of SCT, our findings do have implications for the relation between SCT and several other disorders. These results suggest that SCT is significantly correlated with internalizing and externalizing symptoms, academic difficulties, and lower intelligence. Most of these correlations are small in magnitude, however, and elevations of SCT in individuals with the DSM-IV inattentive type remain significant when all of these variables are controlled. Therefore, although future research is clearly needed to answer this question more definitively, these results suggest that SCT is associated with internalizing symptoms and some specific neurocognitive difficulties, but that a substantial proportion of the variance in SCT is independent of the variance associated with these other variables. Nonetheless, if a new attentional disorder is defined based on SCT in the future, it will be essential to ensure that this new diagnosis does not inadvertently preclude children with 501 other disorders from receiving an appropriate diagnosis and treatment, especially among individuals with severe internalizing disorders that may be experiencing suicidal ideation. Limitations and Future Directions Sampling Issues Because this sample was overselected for both ADHD and learning difficulties (e.g., DeFries et al., 1997; Willcutt et al., 2003), these results warrant replication in samples that are representative of the population and samples ascertained from clinics. Similarly, the average age of the participants in this study (M = 10.6 years) is somewhat older than the age at which many children with ADHD are first referred for a clinical evaluation. Future studies should examine the relation between SCT and ADHD in samples of both younger children and older adolescents and adults. Finally, although the overall sample size is adequate for the procedures described in this report, our current sample is too small to conduct factor analyses separately in males and females. Preliminary results from a larger sample in another laboratory suggest that the three-factor model with separate SCT, inattention, and hyperactivity-impulsivity factors may hold more strongly for males than females (R. Todd, personal communication, July 10, 2003) suggesting that additional studies of potential gender differences in the relation between ADHD and SCT are needed. Measurement Although the availability of both parent and teacher ratings is a strength of this study, SCT symptoms were measured exclusively on a four-point Likert rating scale. Therefore, future studies should examine other methods of assessing SCT, such as diagnostic interviews, ratings by peers or the children themselves, or direct observation in the classroom or testing setting. Due to the relatively unobtrusive nature of SCT behaviors, structured behavioral observations may be especially useful to complement parent and teacher ratings. Further Development of Potential SCT Symptoms As noted previously, the internal and external validity of an exclusively inattentive disorder may be improved by developing positive diagnostic criteria rather than defining the disorder based on a negative diagnostic criterion such 502 as the absence of hyperactivity. By using the largest initial pool of potential SCT items to date, this study provides an important step in this direction. However, our final list of five items is still smaller than the number that is typically recommended to reliably assess a latent construct (e.g., DeVellis, 1991). Therefore, additional research is needed to identify additional SCT items to facilitate the development of a reliable SCT scale. These studies should use an initial pool of potential SCT items of sufficient size to ensure that an adequate number of items remain for the final symptom list even after some items are inevitably discarded due to weak psychometric characteristics. Functional Impairment and Other External Correlates of ADHD and SCT Data from this study and others increasingly support the hypothesis that SCT is an internally consistent construct that relates to ADHD and other disorders in important ways. Therefore, it is essential that future studies test further the external validity of the SCT construct by examining the relation between SCT and important external correlates such as functional impairment and neuropsychological functioning. Such analyses will provide an important step toward determining whether SCT symptoms mediate or moderate the relation between ADHD and these external correlates, or if SCT symptoms identify a unique disorder that is independent of DSM-IV ADHD. Conclusions Confirmatory factor analyses revealed that five putative SCT symptoms loaded on a third factor separate from DSM-IV inattention and hyperactivity-impulsivity symptoms. Teacher ratings of SCT were most strongly associated with the inattentive type, whereas parent ratings indicated that both the combined and inattentive subtypes exhibited significant SCT. In summary, these results suggest that SCT is an internally consistent construct that is significantly associated with DSM-IV inattention. ACKNOWLEDGMENTS Funding for the present research was provided by NICHD grant HD 27802 (Center Director: J. C. DeFries). The authors were also supported in part during the preparation of this manuscript by NIH grants T31 MH 16880 (J. Wehner), F32 MH 12100, R01 MH 62120, and R01 MH 63941 (E. Willcutt), K01 DA 13956 (S. H. Rhee), and MH 38820 and MH 04024 (B. Pennington). The authors thank Hartman, Willcutt, Rhee, and Pennington Ben Lahey, Caryn Carlson, and Keith McBurnett for their helpful suggestions regarding the analyses described in this report. REFERENCES Achenbach, T. (1991a). Manual for the Child Behavior Checklist/4– 18 and 1991 Profile. Burlington, VT: University of Vermont, Department of Psychiatry. Achenbach, T. (1991b). Manual for the Teacher’s Report Form and 1991 Profile. Burlington, VT: University of Vermont, Department of Psychiatry. Akaike, H. (1987). Factor analysis and AIC. Psychometrika, 52, 317–322. American Psychiatric Association. (1980). Diagnostic and statistical manual of mental disorders, 3rd ed. Washington, DC: Author. American Psychiatric Association. (1994). Diagnostic and statistical manual of mental disorders, 4th ed. Washington, DC: Author. Barkley, R. A. (1998). Attention-deficit hyperactivity disorder: A handbook for diagnosis and treatment, 2nd ed. New York: Guilford. Barkley, R. A. (2001). The inattentive type of ADHD as a distinct disorder: What remains to be done. Clinical Psychology: Science and Practice, 8, 489–493. Barkley, R. A., DuPaul, G. J., & McMurray, M. B. (1990). Comprehensive evaluation of attention deficit disorder with and without hyperactivity as defined by research criteria. Journal of Consulting and Clinical Psychology, 58, 775–789. Barkley, R. A., & Murphy, K. (1998). Attention-deficit hyperactivity disorder: A clinical workbook, 2nd. ed. New York: Guilford. Bentler, P. M. (1990). Comparative fit indexes in structural models. Psychological Bulletin, 107, 238–246. Bollen, K. A., & Long, J. S. (1993). Testing structural equation models. Newbury Park, CA: Sage. Carlson, C. L., & Mann, M. (2002). Sluggish cognitive tempo predicts a different pattern of impairment in the Attention Deficit Hyperactivity Disorder, Predominantly inattentive type. Journal of Clinical Child and Adolescent Psychology, 31, 123–129. Carlson, C. L., Shin, M., & Booth, J. (1999). The case for DSM-IV subtypes in ADHD. Mental retardation and developmental disabilities research reviews, 5, 199–206. Chhabildas, N. A., Pennington, B. F., & Willcutt, E. G. (2001). A comparison of the cognitive deficits in the DSM-IV subtypes of ADHD. Journal of Abnormal Child Psychology, 29, 529–540. DeFries, J. C. (1985). Colorado Reading Project. In D. Gray & J. Kavanaugh (Eds.), Biobehavioral measures of dyslexia (pp. 107– 122). Parkton, MD: York Press. DeFries, J. C., Filipek, P. A., Fulker, D. F., Olson, R. K., Pennington, B. F., Smith, S. D., et al. (1997). Colorado learning disabilities research center. Learning Disabilities, 8, 7–19. Devellis, R. F. (1991). Scale development: Theory and applications. New York: Sage. Dunn, L. M., & Markwardt, F. C. (1970). Examiner’s manual: Peabody Individual Achievement Test. Circle Pines, MN: American Guidance Service. DuPaul, G. J., Power, T. P., & Anastopoulos, A. D. (1998). ADHD Rating Scale—IV. New York: Guilford. Faraone, S. V., Biederman, J., Weber, W., & Russell, R. L. (1998). Psychiatric, neuropsychological, and psychosocial features of DSM-IV subtypes of attention-deficit/hyperactivity disorder: Results from a clinically-referred sample. Journal of the American Academy of Child and Adolescent Psychiatry, 37, 185–193. Frick, P. J., Lahey, B. B., Applegate, B., Kerdyck, L., Ollendick, T., Hynd, G. W., et al. (1994). DSM-IV field trials for the disruptive behavior disorders: Symptom utility estimates. Journal of the American Academy of Child and Adolescent Psychiatry, 33(4), 529– 539. Sluggish Tempo and ADHD Gardner, W. (1995). Regression analysis of counts and rates: Poisson, overdisposed poisson, and negative binomial models. Psychological Bulletin, 118, 392–404. Gaub, M., & Carlson, C. (1997). Behavioral characteristics of DSMIV ADHD subtypes in a school-based population. Journal of Abnormal Child Psychology, 25, 103–111. Hinshaw, S. P. (2001). Is the inattentive type of ADHD a separate disorder? Clinical Psychology: Science and Practice, 8, 498–501. Hinshaw, S. P. (2002). Preadolescent girls with attention-deficit/ hyperactivity disorder: I. Background characteristics, comorbidity, cognitive and social functioning, and parenting practices. Journal of Consulting and Clinical Psychology, 70, 1086–1098. Hinshaw, S. P., Carte, E. T., Sami, N., Treuting, J. J., & Zupan, B. A. (2002). Preadolescent girls with attention-deficit/hyperactivity disorder: II. Neuropsychological performance in relation to subtypes and individual classification. Journal of Consulting and Clinical Psychology, 70, 1099–1111. Hollingshead, A. (1975). Two-factor index of social status. Unpublished manuscript. Hynd, G., Nieves, N., Connor, R., Stone, P., Town, P., Becker, M., et al. (1989). Attention deficit disorder with and without hyperactivity: Reaction time and speed of cognitive processing. Journal of Learning Disabilities, 22, 573–580. Kline, R. B. (1998). Principles and practice of structural equation modeling. New York: Guilford. Kovacs, M. (1988). The Children’s Depression Inventory manual. New York: Multi-Health Systems. Lahey, B. B. (2001). Should the combined and predominantly inattentive types of ADHD be considered distinct and unrelated disorders? Not now, at least. Clinical Psychology: Science and Practice, 8, 494–497. Lahey, B. B., Applegate, B., McBurnett, K., Biederman, J., Greenhill, L., Hynd, G. W., et al. (1994). DSM-IV field trials for Attention Deficit Hyperactivity Disorder in children and adolescents. American Journal of Psychiatry, 151, 1673–1685. Lahey, B. B., & Carlson, C. (1991). Validity of the diagnostic category of attention deficit disorder without hyperactivity: A review of the literature. Journal of Learning Disabilities, 24, 110–120. Lahey, B. B., Pelham, W. E., Stein, M. A., Loney, J., Trapani, C., Nugent, K., et al. (1998). Validity of DSM-IV Attention-deficit/Hyperactivity Disorder for young children. Journal of the American Academy of Child and Adolescent Psychiatry, 37, 695–702. Lahey, B. B., & Willcutt, E. (2002). The validity of attentiondeficit/hyperactivity disorder among children and adolescents. In P. S. Jensen & J. R. Cooper (Eds.), Diagnosis and treatment of attention deficit hyperactivity disorder: An evidence-based approach. New York: Civic Research Institute, pp. 1–23. Maedgen, J. W., & Carlson, C. L. (2000). Social functioning and emotional regulation in the attention deficit hyperactivity disorder subtypes. Journal of Clinical Child Psychology, 29, 30–42. McBurnett, K. (1997). Attention-deficit/hyperactivity disorder: Review of diagnostic issues. In T. Widiger, A. Frances, H. Pincus, R. Ross, 503 M. First, & W. Davis (Eds.), DSM-IV sourcebook. Washington, DC: American Psychiatric Association, pp. 111–143. McBurnett, K., Pfiffner, L. J., & Frick, P. J. (2001). Symptom properties as a function of ADHD type: An argument for continued study of sluggish cognitive tempo. Journal of Abnormal Child Psychology, 29(3), 207–213. McCullaugh, P., & Nelder, J. A. (1983). Generalized linear models. London, England: Chapman and Hall. Milich, R., Balentine, A. C., Lynam, D. R. (2001). ADHD combined type and ADHD predominantly inattentive type are distinct and unrelated disorders. Clinical Psychology: Science and Practice, 8, 463–488. Pelham, W. E., Gnagy, E. M., Greenslade, K. E., & Milich, R. (1992). Teacher ratings of DSM-III-R symptoms for the disruptive behavior disorders. Journal of the American Academy of Child and Adolescent Psychiatry, 31, 210–218. Reich, W., & Welner, Z. (1988). Revised version of the Diagnostic Interview for children and adolescents (DICA-R). St. Louis, MO: Washington University School of Medicine, Department of Psychiatry. Skansgaard, E. P., & Burns, G. L. (1998). Comparison of DSM-IV ADHD combined and predominantly inattentive types: Correspondence between teacher ratings and direct observations of inattentive, hyperactivity/impulsivity, slow cognitive tempo, oppositional defiant, and overt conduct disorder symptoms. Child and Family Behavior Therapy, 20, 1–14. Stanford, L. D., & Hynd, G. W. (1994). Congruence of behavioral symptomatology in children with ADD/H, ADD/WO, and learning disabilities. Journal of Learning Disabilities, 27, 243–253. Steiger, J. H., & Lind, J. M. (1980). Statistically-based tests for the number of common factors. Paper presented at the annual meeting of the Psychometric Society, Iowa City, IA. Todd, R. D., Rasmussen, E. R., Neuman, R. J., Reich, W., Hudziak, J. J., Bucholz, K. K., et al. (2001). Familiality and heritability of subtypes of attention deficit hyperactivity disorder in a population sample of adolescent female twins. American Journal of Psychiatry, 158, 1891–1898. Wechsler, D. (1974). Examiner’s manual: Wechsler Intelligence Scale for children—revised. New York: The Psychological Corporation. Wechsler, D. (1981). Manual for the Wechsler Adult Intelligence Scale—Revised. San Antonio: The Psychological Corporation. Willcutt, E. G., Chhabildas, N., & Pennington, B. F. (2001). Validity of the DSM-IV subtypes of ADHD. The ADHD Report, 9, 2–5. Willcutt, E. G., DeFries, J. C., Pennington, B. F., Olson, R. K., Smith, S. D., & Cardon, L. R. (2003). Comorbidity of reading difficulties and ADHD. In R. Plomin, J. C. DeFries, P. McGuffin, & I. Craig (Eds.), Behavioral genetics in a postgenomic era (pp. 227–246). Washington, DC: American Psychological Association. Willcutt, E. G., Pennington, B. F., Boada, R., Tunick, R. A., Ogline, J., Chhabildas, N. A., et al. (2001). A comparison of the cognitive deficits in reading disability and attention-deficit/hyperactivity disorder. Journal of Abnormal Psychology, 110, 157–172.