Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
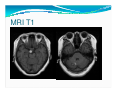
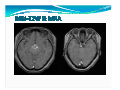
Basic information Date of admission: 96.11.06 Gender: female Age: 36 Present and past history Chief complaint: general weakness and lethargic about several weeks presnet illness and Past history : 1. Seizure history since junior high school f/u in CGMH and never attack her after senior high school 2. Brain tumor was found by brain MRI 2 years ago and reported as benign tumor Present and past history 3. she was presented to our outpatient department for the second opinion and received R/T with SRT 300 cGy * 10 4. Another Brain MRI was done on 96/09/03 and showed:1. Multiple cavernous angiomas 5. On 96/11/12, CT sim for boost after evaluation Present and past history 6. headache,general weakness and lethargic about several weeks ago 7. Then, admitted after evaluation for R/T Physical examination Vital sign: stable, but high BP 153/82 No consciousness change HEENT: grossly normal Chest: breathing sound clear, regular heart beat, no heart murmur Abdomen: soft, normactive bowel sound Extremities: ROM intact, no pitting edema Neurologic examination Cranial nerve: 1. CN I ~ CN XI intact 2. CN XII showed positive fasciculation Motor system 1. Normal muscle power and muscle tone 2. DTR of bicepes, tricepes, knee, supinator, and ankle all normal Neurologic examination Sensation: intact light touch, pain, temporature, and joint position Coodination: 1. Finger-nose-finger test: no ataxia (+ ) 2. Heal-chin test no ataxia (+ ) 3. Romberg's test (- ) Laboratory data WBC RBC 8740/mm3 3.64 X 106 /mm3 Hb Hct PLT Alb BUN/Cr Na/K Ca: 11.5 g/dl 34.6 % 203 X 103/mm3 3.1g/dl 12/ 0.8 137/4.0 8.3 mg/dl Image findings MRI T1W MRI T1 MRI T1 MRI-T2W& MRA Differential diagnosis Vascular malformation 1. AVM 2. Developmental venous anomaly 3. Cavernous hemagioma Tumor with bleeding Impression Multiple heterogeneously high signal intensity on T1W, mixed high signal and dark signal rim on T2W Multiple Subacute intracranial hemorrhage with hemosiderin rim with focal edema Obstructive hydrocephalus of 3rd ventricle Suspected mass effect by hemorrhagic tumor pathology cavernous angioma with ectatic vascular channels containing blood clots and fibrins walled by fibrotic to scelrotic tissue lacking intervening neural tissue. The neural tissue at the peripehral area shows focal calcification and scatterd hemosiderin-laden microglia Discussion Clinical presentation Cerebrum 70%, pons and cerebellum 25% Mean age: 30~40, male: female = 1 : 1 Sporadic or familial location Symptoms and signs Supratentorial 1. hemorrhage 5%, 2. seizures 50%, 3. progressive neurologic deficits 30%. Infratentorial 1. hemorrhage and progressive neurologic deficits , 2. brainstem present with cranial neuropathies and long-tract signs Typical image CT scan: nonspecific, irregular, hyperdense mass with variable degrees of calcification MRI: 1. popcorn" pattern of variable image 2. dark hemosiderin ring, best seen on T2 Angiograpy: Blood flow through CMs is minimal. Thus, they may not be seen on angiography treatment Asymptomatic generally observed carefully, with follow-up MR imaging performed at yearly or 2-year intervals. Symptomatic (severe headache, should be resected with the aid seizures, progressive of frameless stereotactic neurological deficits) guidance. prognosis more than two-thirds of patients were seizure free at 3 years after surgery Predictors for good outcome: 1. mesiotemporal location, 2. size <1.5 cm 3. the absence of secondarily generalized seizures.