Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Cortical stimulation mapping wikipedia , lookup
Dual consciousness wikipedia , lookup
Neuropsychopharmacology wikipedia , lookup
Hereditary hemorrhagic telangiectasia wikipedia , lookup
Brain damage wikipedia , lookup
Hemiparesis wikipedia , lookup
Chapter 10 (pp 139-167) of Multiple Sclerosis 2 - Blue Books of Practical Neurology, vol. 27. J.H Noseworthy, W.I. McDonald (eds.). Elsevier Science (USA), 2003.
Magnetic Resonance Imaging and Spectroscopy: Insights into the Pathology and
Pathophysiology of Multiple Sclerosis.
Zografos Caramanos†, A. Carlos Santos†*, and Douglas L. Arnold†
†
Magnetic Resonance Spectroscopy Unit, Montreal Neurological Institute, McGill University, Montreal, Canada
* Department of Clinical Medicine Imaging Center, Ribeirao Preto Medical School, University of Sao Paulo, Brazil
1.
INTRODUCTION
Since the time that Ormerod, du Boulay, and McDonald wrote
their chapter on the neuroimaging of multiple sclerosis (MS ) for the
first edition of this volume1, continuing advances in the field of
magnetic resonance (MR) and MR imaging (MRI) have made
tremendous impacts in our understanding of this disease2. Over the
last few years, findings from (i) “conventional” MRI techniques
[e.g., T 2-weighted imaging, proton-density-weighted imaging, and
T 1-weighted imaging] – as well as those from (ii) more-recently
developed “non-conventional” MRI techniques [e.g.,
magnetization-transfer imaging (MTI), diffusion-weighted imaging
(DWI), diffusion-tensor imaging (DTI), proton magnetic resonance
spectroscopy (1H-MRS ), and functional MRI (fMRI)] and (iii)
MRI-based estimates of brain and spinal cord atrophy – have
converged with findings from other areas of MS research (e.g.,
histopathological and clinical research) in order to give us a more
comprehensive picture of MS pathology and pathophysiology.
Given that a number of excellent reviews have been written on this
topic in recent years3-9, the purpose of the present chapter is to
describe some of the MRI techniques that are most-commonly used
in the study of MS and to summarize some of the main aspects of
our MRI-based understanding of MS. First, however, we will
briefly review some of the relevant aspects of our current
understanding of the pathology and pathophysiology of MS.
1.1. THE PATHOLOGY AND PATHOPHYSIOLOGY OF MULTIPLE
S CLEROSIS
The pathological hallmark of MS is the presence of
demyelinating lesions (also referred to as MS plaques) within the
central nervous system (CNS ) that are disseminated in both space
and time10. Acute and sub-acute plaques are associated with acute
inflammation and myelin breakdown. Chronic plaques are welldemarcated areas within the white matter that are hypocellular and
characterized by myelin loss and astrocytic scar-formation11.
Although usually described as being “relatively spared,” axons are
injured and their density is decreased in both these types of
demyelinating lesions.
The overt, symptomatic “attacks” of MS that signal the usual
initial “relapsing-remitting” (RR) stage of the disease are generally
attributed to focal inflammation, which is associated with axonal
injury and demyelination that result in slowing and/or blockade of
axonal conduction. Conversely, the remission of symptoms during
this stage is generally attributed to a combination of (i) the
resolution of inflammation, (ii) the insertion of new sodium
channels across demyelinated segments of axons, and (iii) the
remyelination of axons. The majority of patients will eventually
enter a “secondary-progressive” (S P) stage of the disease in which
there is progressive neurological disability that is speculated to
result from (i) the eventual failure of remyelination, (ii) gliosis, and
(iii) irreversible axonal injury and degeneration. Indeed, as reviewed
by Rieckmann and Smith12 and by Bjartmar and Trapp13, MS is no
longer viewed as simply being a disease of inflammation and
demyelination of the white matter: rather, axonal degeneration and
neuronal damage throughout the brain are now accepted as being
prominent features of MS – even early on in the disease.
1.2. S OME RECENT MRI-BASED INSIGHTS INTO MULTIPLE
S CLEROSIS
As we will soon see, insights into the pathology and
pathophysiology of MS have been greatly advanced by information
obtained using MRI. For example, it is now evident that the socalled “normal-appearing” white matter (NAWM, i.e., white matter
that appears normal on gross pathological examination or on
conventional MRI) in patients with MS is, in fact, far from normal;
this is true both on appropriate histological analysis 14; 15, as well as
on non-conventional MRI measures including MTI16, DWI17,
DTI18, and 1H-MRS19; 20. Indeed, further changes in patients’
NAWM may become visible on these measures months – if not
years – before the lesions associated with their MS become
detectable on conventional MRI: this is true for MTI21, DWI22, and
1
H-MRS23; 24.
In addition to this pathology of NAWM, there is now growing
evidence for a significant involvement of the normal-appearing grey
matter (NAGM) of the cerebral cortex in MS. Again, this is true
both on histological analysis 25; 26, as well as on non-conventional
MRI measures including MTI16; 27; 28, DWI29, and 1H-MRS30; 31.
Furthermore, there is now evidence from fMRI for adaptive cortical
reorganization in patients with MS in the absence of neurological
impairment: a finding which suggests that the extent of corticofunctional pathology is greater than that which is manifest
clinically 20; 32-34. Finally, there is also now MRI-based evidence that
brain and spinal cord atrophy (which reflect destructive, irreversible
pathology) are common – even early on in the course of the
disease35.
Page 1 of 18
Of course, all of these aforementioned MR measures that have
contributed to our increased understanding of MS are only surrogate
markers for different aspects of the pathological changes that
accompany the disease. In order to better appreciate what changes
in these MR surrogates mean, we will now review some of the MR
techniques that are currently being used to study MS – first the
conventional ones and then the non-conventional ones. We will then
go on to review some of the findings regarding MRI-based analyses
of cerebral atrophy in patients with MS.
2.
CONVENTIONAL MAGNETIC RESONANCE IMAGING
TECHNIQUES
The conventional MRI techniques used to study MS patients
produce images that reflect the physico-chemical state of protons
that are present mainly in the water in the tissue that is being
imaged. Contrast in such images is derived primarily from tissuespecific differences in the relaxation times, T1 (i.e., the time
constant for the recovery of magnetization in the direction of the
magnetic field) and T2 (i.e., the time constant for the decay of
magnetization in the plane perpendicular to the magnetic field). (For
a review of MRI theory and applications see Gadian36).
These conventional MRI techniques include (i) T 2-weighted
imaging, (ii) proton-density-weighted imaging, (iii) fluid-attenuated
inversion-recovery imaging, (iv) standard T 1-weighted imaging, and
(v) gadolinium-enhanced T 1-weighted imaging – each of which is
described below. Figure 10-1 presents examples of images obtained
using these techniques in patients with MS.
2.1. T2-WEIGHTED IMAGING
MR images are T 2-weighted by allowing more time for signal
decay to occur due to T 2 relaxation during a relatively-long echo
time (TE). Signals from water protons located in tissues associated
with longer T 2 values decay less during a long TE; because of this,
such tissues appear hyperintense on T 2-weighted images relative to
tissues with shorter T 2 values.
T 2 is prolonged in most pathologies that are associated with (i)
inflammatory edema or tissue destruction (i.e., pathologies that
increase bulk water that has less interaction with macromolecules)
or (ii) gliosis in the white matter of the brain. For these reasons, MS
lesions are hyperintense on T 2-weighted scans both in the early
stages of the disease (i.e., when inflammation is most prominent) as
well as in the later stages of the disease (i.e., when tissue injury and
gliosis are more prominent).
2.1.1. T2-Weighted Imaging of Multiple Sclerosis
Consistent with well-known pathological observations, the T 2weighted MR appearance of MS (see Figure 10-1) is primarily one
of multiple, hyperintense white-matter lesions with periventricular
predominance37. (See Narayanan et al38 for an example of the
probabilistic mapping of MS lesions). Because of their exquisite
sensitivity to subtle changes in water, T 2-weighted hyperintensities
can even identify regions of brain tissue that appear normal on gross
pathology and that are only associated with a very subtle
infiltration of inflammatory cells 39.
2.1.1.1. Evolution of T 2-Weighted Hyperintense Lesions
New lesions that are seen on T 2-weighted imaging [or on
proton-density-weighted imaging (see below)] have a characteristic
evolution40. Typically, they reach a maximum size in approximately
four weeks, decrease in size over the next six to eight weeks, and
leave a residual T 2-weighted abnormality37 that is a permanent
record of tissue injury 5. For this reason, the total lesion volume that
can be measured on such scans is often used as a surrogate measure
of disease burden in MS. Furthermore, changes across time in the
number and volume of lesions that are visible on T 2-weighted
imaging can be used as indicators of disease activity and of response
to treatment. It should be noted, however, that such changes in
volume consist partly of inflammatory edema that eventually
resolves with an associated decrease in the volume of T 2-weighted
abnormality41.
2.1.1.2. Clinical Significance of T 2-Weighted Hyperintense Lesions
Although the relationship between T 2-weighted imaging
abnormalities and abnormal findings on histological examination is
strong37; 39, the correlation between total cerebral T 2-weighted lesion
load and clinical disability at any given time is only modest42; 43.
Nevertheless, the predictive value of T 2-weighted lesions for the
future development of clinically-definite MS is strong – particularly
over the long term. For example, Brex et al44 recently published the
latest results of an ongoing, longitudinal study that had, at that
point, followed a group of 71 patients for 14 years from the time of
their initial episode of presumed CNS-demyelination. They found
that clinically-definite MS eventually developed in 44 of the 50
patients with T 2-weighted lesions at presentation (but in only 4 of
21 patients that had presented with normal MRI). Furthermore, the
number and the volume of T 2-weighted lesions at baseline, as well
as the change in lesion volume over the first 5 years, correlated
significantly with the patients’ degree of long-term disability as
measured by the EDSS (i.e., Kurtzke’s Expanded Disability Status
Scale45). The latter correlations were, however, of only moderate
strength – suggesting that, on its own, T 2-weighted lesion data
cannot be used to make strong predictions about the prognosis in a
patient that is known to have MS.
The modest correlation seen between T 2-weighted lesion load
and concurrent clinical disability may be explained by several
factors: (i) the lack of pathological specificity of T 2-weighted
abnormality, (ii) the fact that neurological disability is not easy to
quantify and that the instruments used to do so (primarily the
EDSS) are limited in their scope (e.g., the EDSS is based primarily
on ambulatory ability), (iii) the fact that lesions in different CNS
locations would be expected to correlate differently with disabilities
in different spheres of CNS function (e.g., cerebral lesion-load is
only weakly related to the sensorimotor dysfunction that results
from spinal cord lesions – a dissociation that increases as the MS
disease process progresses 46), and (iv) the fact that lesions may not
be the only pathology responsible for disability, particularly late in
the disease when a neurodegenerative process may develop 13. The
correlation between T 2-weighted lesion volume and disability is also
weakened by (v) the potential of the brain to functionally adapt to
injury 20; 32-34 and (vi) the fact that focal lesions have diffuse
consequences 19; 38. Thus, it is not surprising that it has been difficult
to demonstrate a strong, direct effect of the localization of cerebral
Page 2 of 18
T 2-weighted lesions on specific EDSS-measured functional
impairments47. Nevertheless, there are examples of specific
functional deficits that have been shown to correlate with the T 2weighted lesion load that is present in the region of the CNS
associated with those particular functions (e.g., olfactory
function48, sustained complex-attention and verbal workingmemory 49, and visual function50).
Centrum Semiovale
T2-weighted image
PD-weighted image
T1-weighted image
Gd-enhanced image
PD-weighted image
T1-weighted image
Gd-enhanced image
Lateral Ventricles
T2-weighted image
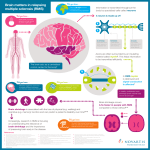
Figure 10-1. Cross-sectional slices through the centrum semiovale (top) and the lateral ventricles of a patient with multiple sclerosis (MS) as
seen on T 2-weighted, proton-density-weighted (PD), T 1-weighted, and gadolinium-enhanced T 1-weighted images. Of note at the level of the
centrum semiovale: (i) many of the hyperintense lesions that can be seen on the T 2- and PD-weighted images are also seen as hypointensities
on the T 1-weighted images and (ii) two of these lesions are still active and inflammatory (as evidenced by the ring-like Gd-enhancement). Of
note at the level of the lateral ventricles: (i) it is difficult to discriminate between the periventricular lesions and cerebrospinal fluid (CSF) on
the T 2-weighted image, (ii) it is easy to discriminate between the periventricular lesions and the CSF on the PD-weighted image; (ii) the extent
of T 2- and PD-weighted hyperintensity is much more extensive than the hypointensities seen on the T 1-weighted images; and (iii) there are
no active, inflammatory lesions at this level (as evidenced by the lack of Gd-enhancement). (Images are courtesy of the Canadian MS/BMT
Study Group).
2.1.1.3. T2-Weighted Hypointensities
In addition to the T 2-weighted white-matter hyperintensities
that we have dealt with thus far, grey-matter hypointensity on T 2weighted imaging of patients with MS (which is thought to reflect
pathologic iron deposition and brain degeneration) has also been
described51 and shown to be related to clinical status52; 53 and
prognosis 54 in MS.
2.2. PROTON -DENSITY-WEIGHTED IMAGING
Because both lesions and cerebrospinal fluid (CSF) are
hyperintense on T 2-weighted images, the discrimination of
periventricular lesions can be difficult. One way of increasing this
discrimination is to acquire images with, so-called, “proton-density
weighting” 55. Such images do not actually reflect the density of
protons; they do, however, have intermediate T 1- (see below) and
Page 3 of 18
T 2-weightings that, as shown in Figure 10-1, result in the CSF
appearing dark (because its long T 1 value predominates over its long
T 2) and lesions appearing bright (because their long T 2 values
predominate over their relatively shorter T 1).
2.3. FLUID-ATTENUATED INVERSION -RECOVERY IMAGING
Another means of increasing contrast between CSF and lesions
is through the use of fluid-attenuated inversion-recovery (FLAIR)
images 55. This approach involves the use of an inversion pulse to
suppress the signal arising from bulk water in the CSF 56. FLAIR
images provide both (i) better discrimination between ventricular
CSF and the periventricular T 2-weighted-hyperintensities that are
associated with MS lesions and (ii) increased contrast for lesions –
particularly for those that are cortical or juxtacortical57.
2.4. T1-WEIGHTED IMAGING
T 1-weighted images are produced by shortening the TR (i.e., the
amount of time between successive repetitions of water-proton
excitation) and, thereby, allowing less time for water to regain its
equilibrium magnetization. Water protons in tissues with a
relatively short T 1 recover more quickly and produce more signal at
relatively-short TR than do those in tissues with a longer T 1.
Protons in bulk water (e.g., in CSF, or in tissue that is associated
with either extracellular edema or with a loss of structural integrity)
have a long T 1 and, as shown in Figure 10-1, appear hypointense on
T 1-weighted sequences.
T 1-weighted images are less sensitive to changes in either watercontent or gliosis than are T 2-weighted images. Nevertheless, acute,
inflammatory lesions can sometimes be associated with so much
edema that they can show substantial T 1-weighted hypointensity.
Chronic T 1-weighted hypointensities are, however, much more
specific indicators of tissue destruction than are T 2-weighted
hyperintensities 58-60. The term “black hole” has been used to
describe hypointense lesions on T 1-weighted images 61. Given the
fact, however, that this term is typically used to imply an
association with irreversible tissue destruction, use of the term is
probably best reserved for lesions that are chronically-hypointense
on T 1-weighted imaging. Only about 30% of new T 2-weighted
lesions will evolve into chronic black holes 62.
2.4.1. T1-Weighted Imaging of Multiple Sclerosis
Given the increased pathological specificity associated with T 1weighted hypointensity, it is not surprising that lesions that show
this feature on T 1-weighted imaging are more strongly correlated to
disability in MS than are lesions that are T 1-isointense43; 59; 61. In a
recent study, Cid et al63 examined the relationship between RR-MS
patients’ (i) degree of lesion hypointensity on T 1-weighted imaging
obtained at the time of an MS relapse, (ii) change in EDSS score
between the time of the relapse and one month later, and (iii)
amount of neuronal apoptosis induced on neuronal cultures by CSF
obtained at the time of the relapse. They found a strong relationship
between T 1-weighted lesion hypointensity and both (i) poor
recovery from relapse and (ii) the amount of neuronal apoptosis
induced by the CSF.
weighted imaging can be increased with the injection of a chelated
form of gadolinium (Gd), which interacts with water so as to
shorten its T 1 relaxation time. Normally, Gd does not cross the
blood-brain barrier (BBB). However, focal inflammation in the CNS
– as occurs during an MS attack – is often associated with an
“opening” of the BBB65. This opening allows Gd to pass through in
a manner that is graded depending upon (i) the extent of the
associated increase in BBB permeability, (ii) the dose of Gd
administered, and (iii) the interval between Gd-injection and T 1weighted MR acquisition (i.e., the time available for the Gd to leak
across the BBB)66; 67.
2.5.1. Gd-Enhanced T1-Weighted Imaging of Multiple
Sclerosis
The acute inflammatory process that was described above is
transient. As a result, Gd only causes MS lesions to enhance for
two to six weeks after they become detectable by conventional
MRI 66; 68. Thus, a useful role for Gd-enhanced T 1-weighted imaging
is to help distinguish recently-appearing, inflammatory lesions from
ones that are more chronic (and no longer associated with sufficient
inflammation to result in Gd enhancement). Indeed, MRI
assessment of disease activity in MS is often based upon the
number of Gd-enhancing lesions that are seen within a T 1-weighted
scan. The majority of enhancing lesions are “nodular,” but about
25% of lesions show “ring-like” enhancement 69. Such ring-enhancing
lesions are associated with a more-severe clinical outcome and it has
been suggested that they reflect a more-destructive pathology 70.
Most lesions that are Gd-enhancing on T 1-weighted images
continue to be detectable on T 2-weighted images after the acute
inflammation (and, thus, the Gd-enhancement) have resolved.
Conversely, it is generally believed that (i) most T 2-weighted
lesions in the central white matter of MS patients are associated
with an initial, variable period of Gd-enhancement on T 1-weighted
imaging and (ii) Gd-enhancing lesions and T 2-weighted lesions
represent two different stages of a single pathological process.
There is evidence, however, to suggest that some of the lesions on
T 2-weighted images can develop independently of Gdenhancement 71 – perhaps because of (i) ongoing low-grade
inflammation that is not detected with Gd-enhancement or (ii)
mechanisms other than inflammation that are responsible for
progression in some existing lesions.
2.5.1.1. Clinical Significance of Gd-Enhancement
About 50% of patients with MS will have at least one Gdenhancing lesion at any given time. Surprisingly, in what is referred
as the “clinico-radiological paradox,” a large proportion of these
lesions are not associated with clinical manifestations: indeed, on
average, Gd-enhancing lesions occur about ten times more
frequently than clinical relapses 3; 72; 73. Despite the striking
difference between the frequency of new Gd-enhancing lesions and
the frequency of clinical exacerbations, there is still, however, a
strong relationship between them74. Furthermore, the number of
enhancing lesions on a single scan is (i) predictive of subsequent
relapse-rate and (ii) is correlated with both subsequent enhancinglesion activity and change in T 2-weighted lesion load75.
2.5. GADOLINIUM-ENHANCED T1-WEIGHTED IMAGING
As reviewed by Rovaris and Filippi64, signal intensity on T 1-
Although the presence of one or more Gd-enhancing brain
Page 4 of 18
lesions is predictive of conversion to clinically definite MS76, Gdenhancement is not a strong predictor of the development of
cumulative impairment or EDSS-measured disability74. These
findings are consistent with the hypothesis that different
pathogenetic mechanisms may be responsible for (i) the occurrence
of relapses and (ii) the development of long-term disability.
MT(on)
MT(off)
with saturation pulse
B
A
3.
% MTr Image
without saturation pulse
B
A
[1-(MTon / MToff)] x 100
B
A
NON-CONVENTIONAL MAGNETIC RESONANCE
IMAGING TECHNIQUES
Even though the aforementioned conventional-MRI techniques
have allowed us to image MS lesions with much greater sensitivity,
these techniques are not capable of fully characterizing and
quantifying the extent of tissue damage in patients with MS. A
number of recently-developed MR techniques are better suited for
such a role. These techniques include: (i) MTI, (ii) DWI, (iii) DTI,
(iv) 1H-MRS, and (v) fMRI – each of which are, in turn, described
below.
Figure 10-2. Examples of T 1-weighted images obtained during a
magnetization transfer (MT) study of a patient with multiple
sclerosis. Images are obtained both with (Mton) and without
(MToff) the presence of a saturation pulse, and MT ratios are
calculated as shown. Note that the MToff image is just a
standard T 1-weighted image and MTR values are more reduced
in lesions that are more hypointense on this image (e.g.,
compare A and B). (Images are courtesy of Dr. G.B. Pike).
3.1. MAGNETIZATION -TRANSFER IMAGING
Protons associated with molecules that are large and less mobile
than water (e.g., the macromolecules that make up cell membranes)
have a very short T 2 and are not visible on conventional MRI; this
is because their signals decay completely before conventional MRI
data is acquired. The effect of these protons can, however, be
observed indirectly by the phenomenon of magnetization transfer
(MT)77. In MTI, appropriate radio-frequency pulses are applied to
selectively saturate the magnetization of the bound protons. This
saturated magnetization is then naturally exchanged with those
protons that are found in the relatively “mobile” protons of CSF,
extracellular water, and intracellular water (i.e., the protons that are
normally observed by MRI). This transfer of saturated
magnetization to the MRI-observable, free-water pool results in a
reduction of the signal intensity from the observable protons to a
degree that depends upon (i) the nature and density of the
macromolecules at a given location and (ii) their interaction with
bulk water. In the white matter of the CNS, the MT effect is
dominated by the large surface area of myelin, and changes in MT
are considered more specific for demyelination78; 79 than are changes
in either T 2 or T 1 relaxation times. It should be noted that MT is
also sensitive to changes in bulk water that are associated with
edema80-82 as well as to macromolecular changes associated with
injury to other cell types (e.g., axons60; 83). Thus, changes in MT
should not be considered pathologically specific.
An important advantage of MTI is that it can be easily
quantified by calculating the magnetization-transfer ratio (MTR),
which is the relative MRI signal intensity measured in the absence
of a saturating pulse compared to the intensity that is measured in
the presence of a saturating pulse (see Figure 10-2). A low MTR
indicates less exchange of magnetization between tissue
macromolecules and the surrounding water molecules.
3.1.1. MTI of Multiple Sclerosis
MTR values are typically reduced in MS lesions in a manner
that is consistent with the degree of T 1-weighted hypointensity60; 84;
85
, which, as we have seen, is related to tissue destruction; thus,
lesions that are larger and more destructive have lower MTR values
than lesions that are smaller and less destructive. Furthermore,
greater reductions in MTR values are seen in lesions that are more
inflammatory 86. In addition to the MTR changes observed in MS
lesions, numerous studies have also reported decreased MTR in the
NAWM of MS patients compared to the white matter of healthy
normal controls 21; 85; 87-89. Greater decreases in MTR are found in
patients with SP-MS than in patients with RR-MS90-92, and these
decreases are related to both increasing EDSS-measured disability43;
93
and increasing cognitive impairment 94.
3.1.1.1. Temporal Evolution of Lesions on MTI
Because MTI produces very reproducible MTR values for a
given pulse sequence, it can be used to quantify the pathological
evolution of MS lesions over time. Such longitudinal MTI studies
have shown that, even before the detection of lesions is possible on
proton-density- or T 2-weighted images, MTR values have begun to
decline in the NAWM that is found at these locations21; 95; 96. Then,
as lesions begin to demonstrate Gd-enhancement on T 1-weighted
imaging, there is an explosive decrease in the lesional MTR values
due to a combination of inflammatory edema and demyelination;
this may be followed by either (i) a stabilization of lesional MTR
values at these lower levels, (ii) a recovery of lesional MTR values
several weeks after the initial decrease, or, in a small number of
lesions, (iii) a continuing decrease in local MTR values 97-99. The
recovery of MTR or its continued decline may be related,
respectively, to remyelination or to chronic activity of lesions.
Thus, MTR provides a potentially powerful tool for exploring
lesion evolution in MS.
3.1.1.2. Clinical Significance of MTI
The fact that MTR focal abnormalities in NAWM develop
Page 5 of 18
before the appearance of lesions implies that MTI might provide
information that could predict the future evolution of MS. This has
led to the assessment of the predictive value of MTI in MS. For
example, the prognostic value of MTI was recently examined by
Santos et al100,who found that mean NAWM-MTR values were
able to successfully predict whether or not levels of disability
would increase at five-year follow-up in patients with relativelylong-standing MS; importantly, MTR values within these
individuals’ T 2-weighted lesions could not predict such changes. In
a related study of patients with a clinically-isolated syndrome
suggestive of MS, Iannucci et al101 found that MTR values at the
time of presentation were significant predictors of the development
of clinically-definite MS within the next 25-42 months (although
not as strong predictors as these patients’ presenting T 2-weighted
lesion volumes). On the other hand, Brex et al102 found that mean
NAWM-MTR values in a similar group of patients could not
predict whether these individuals would go on to have MS in the
following 12 months (at which point, these newly-diagnosed MS
patients still had normal NAWM-MTR). Thus, while it is clear that
MTI has prognostic value in MS, further studies are necessary to
better characterize its strengths and limitations.
As reviewed by Filippi and Inglese106, the pathology associated
with MS modifies the water self-diffusion characteristics in the
CNS by altering the geometry and/or the permeability of structural
barriers that are found therein. The application of DWI techniques
to the study of MS is appealing in that they can provide a
quantitative estimate of the degree of fiber disruption and, thus,
potentially provide information on the mechanisms that lead to
irreversible disability in this disease.
3.2.1. DWI of Multiple Sclerosis
DWI studies have consistently shown that the ADC107; 108 and
of water is (i) higher in MS lesions than in NAWM (see
D
Figure 10-3) and (ii) higher in acute lesions than in chronic lesions.
Such studies have also consistently demonstrated that mean D
values are increased in the NAWM of MS patients compared to
those observed in the white matter of healthy normal controls – a
finding that hold true in the brain17; 110; 111, the spinal cord112, and
the NAGM 16.
109
PD-Weighted Image
Mean Diffusivity Image
Fractional Anisotropy Image
3.1.1.3. MTI of Normal-Appearing Grey Matter
As mentioned in the introduction, there is now an increasing
appreciation that, at the microscopic level, there is substantial
lesional pathology of the NAGM in patients with MS25; 26. The
lesions in NAGM are associated with much less inflammation and
demyelination than are the lesions in the white matter26. Perhaps
related to this, as well as to their size and to their location (i.e.,
adjacent to CSF), these lesions in the NAGM are largely undetected
by current conventional MRI techniques. Thus, it is important that,
in addition to the MTI changes in the lesional and normal-appearing
white matter of patients with MS, reductions in MTR values have
also been found in the NAGM of patients with MS relative to
normal controls 16; 27; 28. Together, these findings suggest that the
pathological process that is at work in the brains of patients with
MS is very diffuse and is not tissue-specific.
3.2. DIFFUSION -WEIGHTED IMAGING
As reviewed by Cercignani and Horsfield103, DWI allows for the
in vivo measurement of the diffusion of water in the CNS due to
Brownian motion. Because both the axolemma and the myelin
sheath restrict water diffusion in nerve fibers104, pathological
processes (such as those at work in MS) that modify the integrity
of such tissues can result in a loss of restricting barriers and,
thereby, increase the so-called “apparent diffusion coefficient”
(ADC) of water.
The ADC is a measure of the random displacement of water
molecules in a particular direction. Because of the restricting entities
that are found in biological tissues, ADC values in the CNS are
lower than the diffusion coefficient of pure water (hence the term
“apparent diffusion coefficient of water”). A measure of diffusion
that is independent of the orientation of structures is provided by
the mean diffusivity index, D . Also referred to as the directionallyaveraged ADC (or ADCavg) or trace, D is the average of the ADCs
measured in three orthogonal directions. (For a review of DWI
theory and applications see, for example, Schaefer et al105).
*
*
*
*
*
*
*
*
*
*
*
*
*
*
*
*
**
**
**
**
**
*
**
**
Figure 10-3. Cross-sectional slices through the lateral ventricles
of a patient with multiple sclerosis as seen on proton-densityweighted (PD), diffusion-weighted, and diffusion-tensor
imaging (which is reviewed in the next section). The asterisks
point out the lesions that are seen as (i) hyperintensities on
PD-weighted imaging, (ii) increased mean diffusivity ( D )
values on diffusion-weighted imaging, and (iii) decreased
fractional anisotropy (FA) values on diffusion-tensor imaging.
(Images are courtesy of J.S.W. Campbell).
D values have been shown to correlate with individual MS
patients’ EDSS scores 113-116 and disease durations114-116.
Furthermore, D values are higher in patients with SP-MS than in
those with RR-MS116; 117. Increases in lesional D values correlate
with hypointensity on T 1-weighted images 116, and ring-enhancing
lesions on Gd-enhanced T 1-weighted images have higher mean D
values than do nodular-enhancing lesions118 – a pattern that
corresponds to reported histopathological differences between these
types of lesions70.
Interestingly, individual patients’ D values are not significantly
related to their MTR values 119 and are only moderately related to
decreases in their 1H-MRS-measured NA/Cr values 120 (the relevance
of which is explained in the section on 1H-MRS below). These
findings suggest that MTI provides information about different
aspects of brain pathology in MS than do these other two imaging
techniques (i.e., MTI and 1H-MRS).
Page 6 of 18
3.2.1.1. Temporal Evolution of Lesions on DWI
Serial DWI studies have also been used in order to investigate
the changes in NAWM that precede the development of acute MS
lesions. For example, Rocca et al121 found that regions of NAWM
that would subsequently become Gd-enhancing lesions had a
significant increase in their mean D values starting six weeks prior
to the appearance of enhancement. Furthermore, Werring et al22,
who acquired a years’ worth of monthly DWI scans in MS
patients, observed (i) a steady and moderate increase in mean
NAWM D values that was followed by (ii) a rapid and marked
increase at the time of Gd-enhancement and (iii) a slow decay after
the end of enhancement. These two studies suggest that new focal
lesions that are associated with an eventual breakdown of the BBB
are preceded by subtle, progressive alterations in tissue integrity
that are below the resolution of conventional MRI. Interestingly,
Werring et al22 also found that there was a mild increase in the mean
D values of NAWM regions that were contralateral and
homologous to the NAWM regions that evolved into Gd-enhancing
lesions (but that themselves did not become lesional) – a finding
that supports the concept that structural damage in lesions can
cause disturbances in connected areas of NAWM 122.
3.3. DIFFUSION -TENSOR IMAGING
The ADC of water in biological tissue that has a regular and
ordered microstructure depends upon the direction along which it is
measured (i.e., it is anisotropic)103. Thus, D (which has a
magnitude but no direction) does not provide a complete
description of the diffusion phenomenon. A full characterization
can, however, be obtained in terms of a tensor (i.e., a matrix of
numbers) that describes the diffusion of water in three dimensions.
From such a tensor it is possible to derive an index of diffusion
anisotropy – the most commonly-used index being that of fractional
anisotropy (FA123; 124). FA values obtained using DTI reflect the
degree of cellular-structure alignment within the tissue that is being
imaged.
In the normal brain, FA images show a marked difference
between (i) grey matter and CSF (which are both virtually
isotropic) and (ii) white matter (which has a variable degree of
anisotropy)125. Maximum FA values are found in white-matter
regions that are characterized by a strongly-ordered parallel
arrangement of fibers, whereas much lower values are found in
regions where white matter fibers have incoherent orientations or
where fiber-bundles cross. In DTI voxels that are normally full of
highly-ordered fibers, a relative decrease in diffusion anisotropy
could signal structural disintegration within the CNS and could be
used to detect both focal damage to major neuronal pathways as
well as remote damage resulting from Wallerian degeneration126. It
should be noted that DTI would be expected to be less sensitive to
such damage in voxels that contained less-ordered tissue or that
contained crossing fibers.
3.3.1. DTI of Multiple Sclerosis
Results similar to those found using DWI have also been found
using DTI in patients with MS. For example, as shown in Figure
10-3, DTI measures of FA have been shown to be decreased in the
NAWM of patients with MS18; 29; 126; 127 and to be even more
decreased in lesions18; 126; 127 – the greatest FA decreases typically
being found in the most destructive (i.e., T 1-weighted hypointense)
lesions18; 126; 127. Similar to the D findings described above119, there
is also a lack of relationship between individual MS patients’ FA
values and their MTR values 128; 129 – further suggesting that
diffusion imaging and MTI provide somewhat independent
measures of brain pathology in MS. Interestingly, whereas
significant negative relationships have been found between
individuals’ EDSS scores and their FA values 18; 29; 127, abnormalities
in FA have not yet been found in RR-MS at the very early stages of
their disease130 and mean FA difference have not yet been found
between different MS subgroups16; 18; 29. If this is not simply the
result of a low sensitivity of DTI for detecting structural damage,
this would imply that the disability in RR-MS has a basis more in
dysfunction than in loss of structural integrity.
3.4. PROTON MAGNETIC RESONANCE S PECTROSCOPY
None of the water-based imaging methods that we have
reviewed so far can provide pathological specificity for injury to a
particular cell type. Pathological specificity for injury to neurons
and neuronal processes (i.e., axons and dendrites) can, however, be
provided by quantification of the neuronal marker compound, Nacetylaspartate (NAA) using 1H-MRS131.
1
H-MRS is fundamentally different from the water-protonbased MRI techniques that we have discussed thus far in that it
records signals that arise from protons in metabolites that are
present in brain tissue at concentrations approximately one
thousand times lower than that of tissue water132. Whereas the
signal-to-noise ratio and image resolution that is possible with these
metabolite-based images is much lower than that for water-based
images, the resulting images can provide chemico-pathological
specificity that is not possible with conventional MR images. The
various approaches to in vivo 1H-MRS include: (i) single-voxel 1HMRS studies (in which proton spectra are acquired from a single
volume) and (ii) 1H-MRS imaging (1H-MRSI) studies [in which
proton spectra are obtained from multiple volume elements (i.e.,
voxels) at the same time].
3.4.1.1.
1
H-MRS Metabolites of Interest
As shown in Figure 10-4, the water-suppressed, localized 1HMRS spectrum of the normal human brain that is recorded at
relatively-long echo times (usually 136 - 272 ms) reveals three
major resonance peaks [the locations of which are expressed as the
difference in parts per million (ppm) between the resonance
frequency of the compound of interest and that of a standard
compound (i.e., tetramethylsilane)]. These peaks are commonly
ascribed to the following metabolites: (i) tetramethyl amines (Cho),
which resonate at 3.2 ppm and are mostly choline-containing
phospholipids that participate in membrane synthesis and
degradation; (ii) creatine and phosphocreatine (Cr), which resonate
at 3.0 ppm and play an important role in energy metabolism; and
(iii) N-acetyl groups (NA), which resonate at 2.0 ppm and are
comprised primarily of the neuronally-localized NAA. A fourth
peak usually arising from either the methyl resonance of lactate
(LA) or lipids (which both resonate at 1.3 ppm), is normally onlybarely visible above the baseline noise but can be detected in certain
pathological conditions. Spectra acquired at shorter echo times (e.g.,
30 ms) are better for detecting resonances that have a short T 2 (e.g.,
Page 7 of 18
lipids and inositol). Unfortunately, such short-T 2 1H-MRS records
broad, overlapping signals that complicate the quantification of such
spectra.
Normal Control
Patient with MS
NA
[1] NWM
[1] NAWM
NA/Cr = 3.83
Cho/Cr = 1.30
NA/Cr = 2.86 NA
Cho/Cr = 1.84
Cho
Cho
Cr
Cr
1
1
[2] NWM
2
NA/Cr = 3.04
Cho/Cr = 1.14
[2] Lesion
NA
2
NA/Cr = 1.91
Cho/Cr = 1.12
NA
Cho
Cr
Cho
Cr
Figure 10-4. Proton-density-weighted magnetic resonance
images through the centrum semiovale and the results of
proton magnetic resonance spectroscopic imaging (1H-MRSI)
in a normal control subject and in a patient with multiple
sclerosis. The superimposed grid in each image represents
individual 1H-MRSI voxels, and the large, thick, white box
represents the entire 1H-MRSI volume of interest for that
individual. The smaller, numbered boxes represent voxels of
normal-appearing white matter (NAWM) and lesional brain
tissue in the patient and normal white matter (NWM) in the
normal control subject. The 1H-MRSI spectra from within
each of these voxels is shown to the right of each image. The
areas under the NA and Cho peaks (normalized to Cr) are
shown above each spectrum. The spectra have been scaled so
that the Cr peak in each of them has the same height. Note (i)
the decrease in NA/Cr values from the patient’s NAWM voxel
relative to the NWM voxels in the control subject, (ii) the even
greater decrease in lesional NA/Cr, and (iii) the increased
Cho/Cr in the patient’s NAWM voxel, which may be
predictive of a soon-to-appear lesion in that location.
The simplest approach to the quantitation of 1H-MR spectra is
to normalize the NA and Cho signal intensities to the signal
intensity from Cr in the same voxel131. Of course, this latter method
does not provide absolute quantification and, importantly, the
resulting measures of relative concentration are only valid if the underlying pathology does not substantially affect the local
concentration of Cr. Thus, it is important that Cr concentrations are
relatively constant throughout normal brain tissue and that they
have also been shown to be relatively constant in both the
lesions133; 134 and the NAWM 134-136 of patients with MS. It should
be noted , however, that Cr values have been shown to decrease in
acute133 and severely-hypointense lesions136: thus, it is
inappropriate to normalize within-lesion NA and Cho values to
within-lesion Cr values in either acute lesions or T 1-weighted black
holes.
The limitations of ratio-based quantitation can be overcome by
the various methods of semi-absolute quantification that have been
developed137; 138. Unfortunately, such methods have their own
limitations; for example, (i) they are dependent on many
assumptions, (ii) they can be difficult to carry out, and (iii) they
tend to have more variance than those based on ratios
3.4.2.
1
H-MRS of Multiple Sclerosis
The resonance intensity that is ascribed to NAA is, arguably,
the most important 1H-MRS signal in the characterization of MS
pathology because NAA is localized exclusively within neurons and
neuronal processes such as axons and dendrites 139; 140. Although
NAA has been found in cell cultures of oligodendroglial cell
lineage 141; 142, this appears to be a phenomenon that is limited to cell
cultures. Indeed, the specificity of NAA as an axon-specific marker
in vivo, even in the presence of injury and significant density of
oligodendroglial cell precursors, has been confirmed in a recent
biochemical and immunohistochemical study of rat optic nerve
transection143. Furthermore, the validity of NAA as a surrogate for
axonal density in MS has been confirmed in studies that correlated
(i) findings from in vivo 1H-MRSI and histopathological analysis of
cerebral biopsy specimens144 and (ii) findings from HPLC and
histopathological analysis of spinal cord biopsy specimens145.
3.4.2.1. NA/Cr
1
H-MRSI-measured NA/Cr values have been used to quantify
neuronal and axonal integrity in vivo in the brains of patients with
MS for over a decade now146; 147. 1H-MRS studies have shown that
periventricular NA/Cr values are low in both the lesions and, to a
lesser extent, the NAWM of patients with MS19; 122; 147; 148. Patients
with SP-MS are more affected than those with RR-MS19; 149.
Interestingly, however, this latter finding seems to be related more
to NA/Cr differences in NAWM than in lesions19. Importantly, just
as with MTI and DWI, 1H-MRSI-measured values of NA/Cr within
the cortical NAGM of patients with MS have also been shown to
be decreased relative to those in the cortical grey matter of healthy
normal controls 30; 31.
Decreases in MS patients’ periventricular-NA/Cr values
are strongly related to both their disease duration and their EDSS
scores 149. Importantly, the correlation between patients’ EDSS
scores and their periventricular NA/Cr values is as strong, or
stronger, than that of any other MRI measure150 – a relationship
that becomes even stronger when EDSS scores are correlated with
estimates of NA/Cr in pure periventricular NAWM 19; 20. In addition
to correlating with patient’s EDSS scores (which are greatly
influenced by a patients’ ambulatory status), periventricular-NA/Cr
values in MS patients have also been shown to be strongly related
to their cognitive abilities 151.
3.4.2.2. Other Metabolites
In addition to NA, several other 1H-MRS resonance intensities
are also important in understanding the MS disease process. For
example, 1H-MRS-observed Cho and lipid peaks are thought to
provide important information regarding myelin breakdown in the
MS disease process23; 148. Furthermore, the presence of myoinositol has been proposed as a marker of glial cells and gliosis 30.
3.4.2.3. Temporal Evolution of Lesions on 1H-MRS
As with MTI and DWI, the earliest abnormalities that are
visible on 1H-MRS occur months before the appearance of Gdenhanced or T 2-weighted lesions. For example, regions of NAWM
that will go on to become lesions have been shown to be associated
with locally-increased levels of both Cho24 and lipids23 – both of
which are markers of abnormality in cell membranes. As newly-
Page 8 of 18
developing lesions become detectable on conventional MRI, they
are associated with focal inflammation, demyelination, and axonal
injury – pathological processes that result in decreases to NA/Cr
values 148; 152-154, further increases to Cho/Cr values 148; 152-154, and
acutely-increased LA/Cr values 148.
Importantly, these NA-related decreases may persist
chronically – particularly in the core of chronic lesions148. On the
other hand, the presence of LA is more common in lesions that are
Gd-enhancing154 and seems to resolve within weeks148. Increases in
Cho/Cr are pronounced in Gd-enhancing lesions153; 154 and may
remain elevated for years148, but eventually return to normal136; 148.
3.4.2.4. Spatial Distribution of 1H-MRSI Pathology
Changes in 1H-MRSI metabolites are greatest in the core of
lesions and decrease with increasing distance from their center148.
Importantly, they do not end at the edge of the T 2-weighted
abnormality but extend into the surrounding NAWM 148. For
example, in the hyper-acute phase of the lesion (i.e., when it is still
expanding), both the decrease in NA/Cr and the increase in Cho/Cr
can be found around the lesion in the NAWM that is well beyond
the expanding T 2-weighted abnormality. It is still not clear if the
NAWM abnormalities in patients with MS result from (i) the sum
of the remote effects of focal, lesional pathology or (ii) an
independent process that is more diffuse.
been shown to be even more related to FA and NA/Cr values that
are measured specifically within the periventricular NAWM 20 –
implying that NAWM changes are more specifically related to
functional change than those in non-segmented periventricular brain
tissue (which contains NAWM, NAGM, and lesions). This reorganized cortico-motor activation has been found in regions of the
brain that are usually only activated in the execution of morecomplex motor tasks – suggesting that such activation reflects, at
least in part, disinhibition of latent motor pathways that are
“recruited” to limit any functional impairment related to the tissue
damage associated with MS157. Individual patients’ levels of
activation within these recruited areas have been shown to be
related to their (i) EDSS scores, (ii) disease duration, (iii) extent and
number of spinal cord lesions, (iv) brain and spinal-cord MTR, (v)
whole-brain D , and (vi) and whole-brain FA157. Together, these
findings suggest that compensation due to adaptive cortical changes
can contribute to sustaining motor functions during the early stages
of MS; as a result, the actual extent of cortico-functional pathology
in patients with MS may be greater than that which is clinically
evident.
Normal Control
MS Patient 1
w/ Low Disability, Normal NA/Cr
MS Patient 2
w/ Low Disability, Low NA/Cr
3.5. FUNCTIONAL MAGNETIC RESONANCE IMAGING
fMRI is another MR technique that differs fundamentally from
the others discussed so far. For example, the blood-oxygen level
dependent method of fMRI (a widely-used approach to such an
analysis) exploits the fact that hemoglobin and deoxyhemoglobin are
magnetically different such that hemoglobin shows up better on
MRI images than does deoxyhemoglobin155. Brain activation is
associated with increased blood flow and greater blood oxygenation
that, in turn, produce an increased MR signal. fMRI involves (i) the
acquisition of a series of such MR images of the brain in quick
succession and (ii) the statistical analysis of these images in order to
quantify subtle changes in the functional state of the brain across
time.
Figure 10-5. Examples of fMRI activation maps (in white)
obtained during a simple finger-flexion motor task and
registered on to anatomical MR images for a normal control
subject, a multiple sclerosis (MS) patient with normal
periventricular NA/Cr, and an MS patient with abnormallylow periventricular NA/Cr. Both patients were able to perform
the task without difficulty and had low disability ratings. Note
the larger, bilateral extent of functional activation in the patient
with low NA/Cr. (Images are courtesy of Dr. P.M.
Matthews).
3.5.1. fMRI of Multiple Sclerosis
Thus far, fMRI has been used in patients with MS to study
abnormal patterns of brain activation that occur during the
performance of simple motor tasks20; 32-34; 156; 157. These studies
have shown that, as with other forms of brain injury, there is
adaptive cortical reorganization in patients with MS as evidenced
by extended, bilateral activation in motor-related regions (as
opposed to the more-constrained, mostly-unilateral activation that
is seen in normal controls during the tasks that have been used in
these studies).
Reddy et al156 combined findings from fMRI of a simple fingerflexion task with those from 1H-MRSI. As shown in Figure 10-5,
they demonstrated that the extent of this functional reorganization
[as expressed in the form of a lateralization index (LI) that reflected
the degree of bilateral versus unilateral functional-activation] was
strongly related to the presence of axonal injury (as measured by
decreased periventricular NA/Cr on 1H-MRSI). LI values have since
4.
MR-BASED ASSESSMENT OF BRAIN ATROPHY
Atrophy of the brain or spinal cord at post mortem examination
is one of the pathological hallmarks of irreversible CNS damage. As
reviewed by Simon35, with the advent of MRI, it is now possible to
assess CNS atrophy in vivo using a variety of measures that
include, for example, (i) ventricular enlargement, (ii) grey- and
white-matter volumes, and (iii) the use of more-global measures
such as (a) the brain parenchymal fraction (BPF, i.e., the ratio of
brain parenchymal volume to the total volume within the surface
contour of the brain)158 or (b) BICCR (i.e., the ratio of brain
parenchymal volume within the surface contour of the inner table of
the skull)159.
Page 9 of 18
4.1.1. Atrophy in Multiple Sclerosis
CNS atrophy in patients with MS has been documented since
the original autopsy examinations of such individuals – with
atrophy having been shown to reflect (i) injury and loss of both (a)
neurons and their processes and (b) oligodendrocytes and the
myelin that they produce, as well as (ii) changes in the supporting
matrix that result from the contraction of glial tissue35. Until
recently, such atrophy has generally been thought of as occurring
late in the disease35; this view has changed, however, with the
development of neuroimaging techniques that have demonstrating
atrophy in the majority of patients with MS – even at very early
stages of the disease158; 160; 161.
4.1.1.1. Clinical Significance of CNS Atrophy
The average amount of accumulated spinal cord atrophy has
been shown to be greater in patients with SP-MS than in patients
with RR disease162-165. Similarly, as a group, SP-MS patients have
also been shown to have smaller brain volumes, and larger lateral
ventricles, than RR-MS patients159; 166 (see Figure 10-6).
Normal Control
Patient with RR-MS
Patient with SP-MS
Figure 10-6. Cross-sectional slices through the lateral ventricles
of a normal control subject, a patient with relapsing-remitting
multiple sclerosis (RR-MS), and a patient with secondaryprogressive multiple sclerosis (SP-MS) as seen on T 2-weighted
imaging. Note (i) the high degree of atrophy seen even in the
early stage of the disease (as evidenced visually by the
ventricular enlargement in the RR-MS patient as compared to
the control subject) and (ii) the even-greater degree of atrophy
that is seen in the secondary-progressive stage of the disease
(as evidenced visually by the sulcal enlargement, the decreased
volume of the white- and grey-matter, and the furtherincreased ventricular enlargement in the SP-MS patient).
Brainstem and upper-spinal-cord atrophy have been shown to
be strongly correlated with EDSS scores in patients with MS164; 167.
This may, in part, be due to the fact that atrophy in these regions
can be related to Wallerian degeneration following damage to the
cerebrum, to the spinal cord, or to both. Moderate correlations have
also been found between individuals’ EDSS scores and their degrees
of (i) callosal atrophy 42; 168, (ii) cerebral white-matter atrophy 162,
and (iii) ventricular enlargement 42; 169-172. On the other hand,
correlations between EDSS scores and brain-parenchyma-based
estimates of atrophy have been variable – ranging from strong158; 159;
173
to non-significant 115; 174; 175. It should be noted that MRI
measures of brain volume and atrophy have been also shown to be
significantly related to the presence of depression176, impaired
quality of life177, and cognitive decline173; 178 in patients with MS.
4.1.1.2. Rate of Atrophy
Brain atrophy develops at a remarkably-high rate in patients
with MS35. For instance, Fox et al179 showed that (i) the yearly rate
of cerebral atrophy in their MS group (0.8% per year) was over
twice that of normal controls (0.3%) and (ii) the yearly rate of
ventricular enlargement in patients was almost five times greater
than in the controls (1.6 versus 0.3 cc per year). Furthermore,
Simon et al180 studied 85 RR-MS patients with mild-to-moderate
disability over the course of two years and found that (i) the
volume of the lateral ventricles increased at a rate of 5.5% per year
and (ii) the area of the corpus callosum decreased at a rate of 4.9%
per year. The course of cerebral atrophy in these patients was
related to prior inflammatory disease activity as indicated by the
presence of Gd-enhancing, T 1-weighted lesions at baseline. Analysis
of a subset of these patients (n=72) found a yearly decrease of
0.61% in their BPF, which translated to a yearly loss of
approximately 8 cc per year158.
There is some preliminary evidence to suggest that the rate of
atrophy in patients with RR-MS differs from that in patients with
SP-MS in a region-specific manner181; 182. For example, SP-MS
patients seem to have a significantly-faster rate of atrophy around
the ventricles than patients with RR-MS – suggesting a greater
relative volume change along the long projection tracts182. On the
other hand, the rate of spinal cord atrophy has been reported to be
faster in patients with RR-MS164. These findings suggest that CNS
atrophy may not be a uniform process and that different regions
may have distinct responses to disease progression.
4.1.1.3. Relationship of Atrophy to Other MRI Measures
As might be expected, CNS atrophy in patients with MS has
been shown to be related to many of the other MRI-measures that
we have reviewed in this chapter. For example, patients’
supratentorial brain volumes have been shown to be significantly
related to their load of hypointense lesions on T 1-weighted
imaging183; 184. Similarly, patients’ numbers of Gd-enhancing T 1weighted lesions have been shown to be well-correlated with an
increase in their ventricular size166; 185 – especially in patients with a
high proportion of ring-enhancing lesions185. Furthermore, in two
related longitudinal studies, Luks et al172 found that patients’ total
numbers of new Gd-enhancing lesions were related to their monthly
changes in ventricular volume, and Simon et al180 found that the
degree of cerebral atrophy observed over a two-year period (as
indicated by ventricular enlargement and callosal atrophy) was
greater for patients that had entered their trial with Gd-enhancing
lesions. It should be noted, however, that not all studies have found
a relationship between Gd-enhancement and atrophy 186.
The relationship of atrophy with T 2-weighted lesion load has
also been somewhat inconsistent. For example, whereas some
groups have found a significant relationship between their patients’
T 2-hyperintense lesion load and their (i) degree of ventricular
enlargement 162, (ii) callosal atrophy 162, and (iii) overall brain
volume90, others have been unable to find a significant relationship
with their patients’ supratentorial brain volumes 183; 184.
Page 10 of 18
The relationship between cerebral atrophy and the newer, nonconventional MRI measures seems to be more consistent. For
example, brain volume has been shown to correlate with both (i)
MTR values within normal-appearing brain tissue90 and (ii) D
values within the brain parenchyma115. Furthermore, Collins et al159
found that cerebral atrophy (as measured by BICCR values) was
correlated with periventricular axonal injury (as measured by
decreases in 1H-MRSI NA/Cr values) in their group of patients
with SP-MS. BICCR values in their group of mildly-disabled
patients with RR-MS were not reduced relative to their normal
control group, even though this group of patients did have
significantly reduced NA/Cr values. Together, these findings suggest
that microscopic and biochemical changes in the brains of patients
with MS are related to the decreases in brain volume that are found
in such individuals; importantly, however, there seems to be a
decoupling between axonal damage and atrophy in the very early
stages of the disease.
4.1.1.4. Caveats
It should be noted that current MRI analysis techniques allow
for the measurement of small changes in volume on the order of
0.2% of total brain volume – changes of magnitude that are much
smaller than those that can be identified on gross pathological
examination. Thus far, it has been tempting to (i) assume that these
small changes in brain volume have the same pathological
significance as gross atrophy post mortem and (ii) suggest that they
provide a measure of a specific pathological feature such as axonal
loss. Unfortunately, it is not clear that this is always the case: for
example, myelin loss, glial- and matrix-related changes, as well as
shifts in water distribution all occur in MS and may be associated
with volume changes of this magnitude. Although it is clear that
volume measurements must contribute in some way to estimating
the full extent of irreversible axonal damage in MS, further
investigations are required to understand the precise pathological
significance of atrophy and the mechanisms that contribute to its
progression.
5.
SUMMARY AND CONCLUSIONS
MS, consistent with the emerging view that the pathology in this
disease is relatively diffuse and not specifically tied to the white
matter. Importantly, the amount of such microscopic, pathological
change in any individual patient is highly related to their degree of
concurrent disability and is also related to future changes in their
disability. Second, certain pathological changes in NAWM can
foreshadow the appearance of the focal lesions that are classically
associated with MS. Third, there is significant cortico-functional
reorganization that takes place in the brains of patients with MS; a
reorganization that, at least at the early stages of the disease, seems
to have the potential to be functionally-adaptive and compensate
for some of the effects of the ongoing neuropathological processes
that are associated with the disease. Fourth, all of these changes are
occurring in parallel with the progressive CNS atrophy, even in the
early course of the disease.
Although findings from MRI have taught us much about the
MS disease process over the sixteen years since the publication of
the first edition of this volume, we still have much to learn about
the spatial and temporal dynamics of the lesional and non-lesional
pathological tissue that characterizes the MS brain. It is the hope
and goal of the present authors that a multimodal, multiparametric
approach to the analysis of longitudinal data obtained from a
combination of conventional and non-conventional imaging
techniques will become commonplace. Such an approach still has
much to teach us about the spatial and temporal characteristics of
the MS disease process, and the knowledge that it will provide us
with will undoubtedly lead to better methods of treating and
monitoring MS.
REFERENCES
1. Ormerod IEC, du Boulay GH, McDonald WI. Imaging of multiple
sclerosis. In McDonald WI, Silberberg DH (eds). Multiple
Sclerosis. Bodmin, Cornwall: Butterworth & Co. (Publishers),
1986.
2. Matthews PM, Arnold DL. Magnetic resonance imaging of multiple
sclerosis: new insights linking pathology to clinical evolution.
Curr Opin Neurol 2001; 14; 3: 279-87.
As we have seen, our understanding of the pathology and
pathophysiology of MS has been greatly advanced by information
obtained using MRI. For example, the conventional MRI techniques
that were described above have greatly increased the sensitivity
with which lesions can be detected. In addition, they have also
provided us with a great deal of in vivo information regarding the
spatial distribution, temporal dynamics, and clinical significance of
these lesions. Furthermore, the newer, non-conventional methods of
MR acquisition and analysis that were also described above have
allowed us to quantify in vivo the microscopic, molecular
pathology; the biochemical changes; the cortico-functional
adaptations; and the progressive atrophy that may occur in the
brain and spinal cord of patients with MS.
3. Miller DH, Grossman RI, Reingold SC, McFarland HF. The role of
magnetic resonance techniques in understanding and managing
multiple sclerosis. Brain 1998; 121; Pt 1: 3-24.
Based primarily on the findings from the non-conventional MRI
methods that were reviewed in this chapter, a number of important
insights regarding MS pathology and pathophysiology have become
evident. First, there are significant pathological changes in the
otherwise normal-appearing grey and white matter of patients with
7. Nyul LG, Udupa JK. MR image analysis in multiple sclerosis.
Neuroimaging Clin N Am 2000; 10; 4: 799-816 ,x.
4. Paty DW, Moore GRW. Magnetic resonance imaging changes as
living pathology in multiple sclerosis. In Paty DW, Ebers GC
(eds). Multiple Sclerosis. Philadelphia: F.A. Davis, 1998.
5. Barkhof F, van Walderveen M. Characterization of tissue damage in
multiple sclerosis by nuclear magnetic resonance. Philos Trans R
Soc Lond B Biol Sci 1999; 354; 1390: 1675-86.
6. Frank JA. Advances in Multiple Sclerosis. In Drayer BP (ed).
Neuroimaging Clinics of North America. Philadelphia: W. B.
Saunders Company, 2000; 10(4).
8. Filippi M. Non-conventional MR techniques to monitor the
evolution of multiple sclerosis. Neurol Sci 2001; 22; 2: 195-200.
Page 11 of 18
9. Rudick RA. Evolving concepts in the pathogenesis of multiple
sclerosis and their therapeutic implications. J Neuroophthalmol
2001; 21; 4: 279-83.
10. McDonald WI, Compston A, Edan G, Goodkin D, Hartung HP,
Lublin FD, McFarland HF, Paty DW, Polman CH, Reingold SC,
Sandberg-Wollheim M, Sibley W, Thompson A, van den Noort S,
Weinshenker BY, Wolinsky JS. Recommended diagnostic criteria
for multiple sclerosis: guidelines from the International Panel on
the diagnosis of multiple sclerosis. Ann Neurol 2001; 50; 1: 1217.
11. Ludwin SK. The neuropathology of multiple sclerosis.
Neuroimaging Clin N Am 2000; 10; 4: 625-48 ,vii.
12. Rieckmann P, Smith KJ. Multiple sclerosis: more than
inflammation and demyelination. Trends Neurosci 2001; 24; 8:
435-7.
13. Bjartmar C, Trapp BD. Axonal and neuronal degeneration in
multiple sclerosis: mechanisms and functional consequences. Curr
Opin Neurol 2001; 14; 3: 271-8.
14. Evangelou N, Esiri MM, Smith S, Palace J, Matthews PM.
Quantitative pathological evidence for axonal loss in normal
appearing white matter in multiple sclerosis. Ann Neurol 2000;
47; 3: 391-5.
15. Evangelou N, Konz D, Esiri MM, Smith S, Palace J, Matthews PM.
Regional axonal loss in the corpus callosum correlates with
cerebral white matter lesion volume and distribution in multiple
sclerosis. Brain 2000; 123; Pt 9: 1845-9.
16. Cercignani M, Bozzali M, Iannucci G, Comi G, Filippi M.
Magnetisation transfer ratio and mean diffusivity of normal
appearing white and grey matter from patients with multiple
sclerosis. J Neurol Neurosurg Psychiatry 2001; 70; 3: 311-317.
changes in multiple sclerosis: a serial diffusion MRI study. Brain
2000; 123; Pt 8: 1667-76.
23. Narayana PA, Doyle TJ, Lai D, Wolinsky JS. Serial proton
magnetic resonance spectroscopic imaging, contrast-enhanced
magnetic resonance imaging, and quantitative lesion volumetry in
multiple sclerosis. Ann Neurol 1998; 43; 1: 56-71.
24. Tartaglia MC, Narayanan S, Stefano ND, Arnaoutelis R, Antel SB,
Francis SJ, Santos AC, Lapierre Y, Arnold DL. Choline is
increased in pre-lesional normal appearing white matter in
multiple sclerosis. Neurology 2001; 56: Suppl 3, A460. (Abstr.)
25. Kidd D, Barkhof F, McConnell R, Algra PR, Allen IV, Revesz T .
Cortical lesions in multiple sclerosis. Brain 1999; 122; Pt 1: 1726.
26. Peterson JW, Bo L, Mork S, Chang A, Trapp BD. Transected
neurites, apoptotic neurons, and reduced inflammation in cortical
multiple sclerosis lesions. Ann Neurol 2001; 50; 3: 389-400.
27. Ge Y, Grossman RI, Udupa JK, Babb JS, Kolson DL, McGowan JC.
Magnetization transfer ratio histogram analysis of gray matter in
relapsing-remitting multiple sclerosis. AJNR Am J Neuroradiol
2001; 22; 3: 470-5.
28. Ge Y, Grossman RI, Udupa JK, Babb JS, Mannon LJ, McGowan JC.
Magnetization Transfer Ratio Histogram Analysis of NormalAppearing Gray Matter and Normal-Appearing White Matter in
Multiple Sclerosis. J Comput Assist Tomogr 2002; 26; 1: 62-68.
29. Ciccarelli O, Werring DJ, Wheeler-Kingshott CA, Barker GJ,
Parker GJ, Thompson AJ, Miller DH. Investigation of MS
normal-appearing brain using diffusion tensor MRI with clinical
correlations. Neurology 2001; 56; 7: 926-33.
17. Filippi M, Iannucci G, Cercignani M, Assunta Rocca M, Pratesi A,
Comi G. A quantitative study of water diffusion in multiple
sclerosis lesions and normal-appearing white matter using echoplanar imaging. Arch Neurol 2000; 57; 7: 1017-21.
30. Kapeller P, McLean MA, Griffin CM, Chard D, Parker GJ, Barker
GJ, Thompson AJ, Miller DH. Preliminary evidence for neuronal
damage in cortical grey matter and normal appearing white
matter in short duration relapsing-remitting multiple sclerosis: a
quantitative MR spectroscopic imaging study. J Neurol 2001;
248; 2: 131-8.
18. Filippi M, Cercignani M, Inglese M, Horsfield MA, Comi G.
Diffusion tensor magnetic resonance imaging in multiple
sclerosis. Neurology 2001; 56; 3: 304-11.
31. Sharma R, Narayana PA, Wolinsky JS. Grey matter abnormalities
in multiple sclerosis: proton magnetic resonance spectroscopic
imaging. Mult Scler 2001; 7; 4: 221-6.
19. Fu L, Matthews PM, De Stefano N, Worsley KJ, Narayanan S,
Francis GS, Antel JP, Wolfson C, Arnold DL. Imaging axonal
damage of normal-appearing white matter in multiple sclerosis.
Brain 1998; 121; Pt 1: 103-13.
32. Reddy H, Narayanan S, Matthews PM, Hoge RD, Pike GB,
Duquette P, Antel J, Arnold DL. Relating axonal injury to
functional recovery in MS. Neurology 2000; 54; 1: 236-9.
20. Caramanos Z, Campbell JSW, Narayanan S, Francis SJ, Antel SB,
Reddy H, Matthews PM, Sappey-Marinier D, Pike GB, Arnold
DL. Axonal integrity and fractional anisotropy in the normalappearing white matter of patients with multiple sclerosis:
Relationship to cerebro-functional reorganization and clinical
disability. Proc Int Soc Magn Reson Med Submitted; (Abstr.)
21. Pike GB, De Stefano N, Narayanan S, Worsley KJ, Pelletier D,
Francis GS, Antel JP, Arnold DL. Multiple sclerosis:
magnetization transfer MR imaging of white matter before lesion
appearance on T2-weighted images. Radiology 2000; 215; 3:
824-30.
22. Werring DJ, Brassat D, Droogan AG, Clark CA, Symms MR,
Barker GJ, MacManus DG, Thompson AJ, Miller DH. The
pathogenesis of lesions and normal-appearing white matter
33. Lee M, Reddy H, Johansen-Berg H, Pendlebury S, Jenkinson M,
Smith S, Palace J, Matthews PM. The motor cortex shows
adaptive functional changes to brain injury from multiple
sclerosis. Ann Neurol 2000; 47; 5: 606-13.
34. Rocca MA, Colombo B, Comi G, Filippi M. fMRI changes in
patients with relapsing-remitting MS and no clinical disability.
Proc Int Soc Magn Reson Med 2001; 9: 256. (Abstr.)
35. Simon JH. Brain and spinal cord atrophy in multiple sclerosis.
Neuroimaging Clin N Am 2000; 10; 4: 753-70 ,ix.
36. Gadian DG. NMR and its Applications to Living Systems, 2nd ed.
Oxford: Oxford University Press, 1996.
37. Li DK, Zhao G, Paty DW. T2 hyperintensities: findings and
significance. Neuroimaging Clin N Am 2000; 10; 4: 717-38 ,ix.
Page 12 of 18
38. Narayanan S, Fu L, Pioro E, De Stefano N, Collins DL, Francis GS,
Antel JP, Matthews PM, Arnold DL. Imaging of axonal damage
in multiple sclerosis: spatial distribution of magnetic resonance
imaging lesions. Ann Neurol 1997; 41; 3: 385-91.
39. De Groot CJ, Bergers E, Kamphorst W, Ravid R, Polman CH,
Barkhof F, van der Valk P. Post-mortem MRI-guided sampling of
multiple sclerosis brain lesions: increased yield of active
demyelinating and (p)reactive lesions. Brain 2001; 124; Pt 8:
1635-45.
multiple sclerosis: decreased signal in thalamus and putamen. Ann
Neurol 1987; 22; 4: 546-50.
52. Bakshi R, Dmochowski J, Shaikh ZA, Jacobs L. Gray matter T2
hypointensity is related to plaques and atrophy in the brains of
multiple sclerosis patients. J Neurol Sci 2001; 185; 1: 19-26.
53. Bakshi R, Shaikh ZA, Janardhan V. MRI T2 shortening ('black
T2') in multiple sclerosis: frequency, location, and clinical
correlation. Neuroreport 2000; 11; 1: 15-21.
40. Willoughby EW, Grochowski E, Li DK, Oger J, Kastrukoff LF,
Paty DW. Serial magnetic resonance scanning in multiple
sclerosis: a second prospective study in relapsing patients. Ann
Neurol 1989; 25; 1: 43-9.
54. Bakshi R, Benedict RH, Bermel RA, Caruthers SD, Puli SR, Tjoa
CW, Fabiano AJ, Jacobs L. T2 Hypointensity in the Deep Gray
Matter of Patients With Multiple Sclerosis: A Quantitative
Magnetic Resonance Imaging Study. Arch Neurol 2002; 59; 1:
62-68.
41. Isaac C, Li DK, Genton M, Jardine C, Grochowski E, Palmer M,
Kastrukoff LF, Oger J, Paty DW. Multiple sclerosis: a serial study
using MRI in relapsing patients. Neurology 1988; 38; 10: 15115.
55. Butman JA, Frank JA. Overview of imaging in multiple sclerosis
and white matter disease. Neuroimaging Clin N Am 2000; 10; 4:
669-687.
42. Schreiber K, Sorensen PS, Koch-Henriksen N, Wagner A,
Blinkenberg M, Svarer C, Petersen HC. Correlations of brain MRI
parameters to disability in multiple sclerosis. Acta Neurol Scand
2001; 104; 1: 24-30.
56. Gawne-Cain ML, O'Riordan JI, Thompson AJ, Moseley IF, Miller
DH. Multiple sclerosis lesion detection in the brain: a comparison
of fast fluid-attenuated inversion recovery and conventional T2weighted dual spin echo. Neurology 1997; 49; 2: 364-70.
43. Barkhof F. MRI in multiple sclerosis: correlation with expanded
disability status scale (EDSS). Mult Scler 1999; 5; 4: 283-6.
57. Bakshi R, Ariyaratana S, Benedict RH, Jacobs L. Fluid-attenuated
inversion recovery magnetic resonance imaging detects cortical
and juxtacortical multiple sclerosis lesions. Arch Neurol 2001;
58; 5: 742-8.
44. Brex PA, Ciccarelli O, O'Riordan JI, Sailer M, Thompson AJ,
Miller DH. A longitudinal study of abnormalities on MRI and
disability from multiple sclerosis. New England Journal of
Medicine 2002; 346; 3: 158-164.
45. Kurtzke JF. Rating neurologic impairment in multiple sclerosis: an
expanded disability status scale (EDSS). Neurology 1983; 33; 11:
1444-52.
46. Narayanan S, De Stefano N, Francis GS, Tartaglia MC, Arnaoutelis
R, Arnold DL. Disease duration influences the relationship
between brain axonal injury, spinal cord atrophy, and disability in
multiple sclerosis. Proc Int Soc Magn Reson Med 2000; 1: 297.
(Abstr.)
47. Riahi F, Zijdenbos A, Narayanan S, Arnold D, Francis G, Antel J,
Evans AC. Improved correlation between scores on the expanded
disability status scale and cerebral lesion load in relapsingremitting multiple sclerosis. Results of the application of new
imaging methods. Brain 1998; 121; Pt 7: 1305-12.
48. Zorzon M, Ukmar M, Bragadin LM, Zanier F, Antonello RM,
Cazzato G, Zivadinov R. Olfactory dysfunction and extent of
white matter abnormalities in multiple sclerosis: a clinical and
MR study. Mult Scler 2000; 6; 6: 386-90.
49. Sperling RA, Guttmann CR, Hohol MJ, Warfield SK, Jakab M,
Parente M, Diamond EL, Daffner KR, Olek MJ, Orav EJ, Kikinis
R, Jolesz FA, Weiner HL. Regional magnetic resonance imaging
lesion burden and cognitive function in multiple sclerosis: a
longitudinal study. Arch Neurol 2001; 58; 1: 115-21.
50. Caruana PA, Davies MB, Weatherby SJ, Williams R, Haq N, Foster
DH, Hawkins CP. Correlation of MRI lesions with visual
psychophysical deficit in secondary progressive multiple
sclerosis. Brain 2000; 123; Pt 7: 1471-80.
58. van Walderveen MA, Kamphorst W, Scheltens P, van Waesberghe
JH, Ravid R, Valk J, Polman CH, Barkhof F. Histopathologic
correlate of hypointense lesions on T1-weighted spin- echo MRI
in multiple sclerosis. Neurology 1998; 50; 5: 1282-8.
59. Barkhof F, Karas GB, van Walderveen MA. T1 hypointensities
and axonal loss. Neuroimaging Clin N Am 2000; 10; 4: 739-752.
60. van Waesberghe JH, Kamphorst W, De Groot CJ, van Walderveen
MA, Castelijns JA, Ravid R, Lycklama a Nijeholt GJ, van der
Valk P, Polman CH, Thompson AJ, Barkhof F. Axonal loss in
multiple sclerosis lesions: magnetic resonance imaging insights
into substrates of disability. Ann Neurol 1999; 46; 5: 747-54.
61. Truyen L, van Waesberghe JH, van Walderveen MA, van Oosten
BW, Polman CH, Hommes OR, Ader HJ, Barkhof F.
Accumulation of hypointense lesions ("black holes") on T1 spinecho MRI correlates with disease progression in multiple
sclerosis. Neurology 1996; 47; 6: 1469-76.
62. van Walderveen MA, Truyen L, van Oosten BW, Castelijns JA,
Lycklama a Nijeholt GJ, van Waesberghe JH, Polman C, Barkhof
F. Development of hypointense lesions on T1-weighted spinecho magnetic resonance images in multiple sclerosis: relation to
inflammatory activity. Arch Neurol 1999; 56; 3: 345-51.
63. Cid C, Alcazar A, Regidor I, Masjuan J, Salinas M, AlvarezCermeno JC. Neuronal apoptosis induced by cerebrospinal fluid
from multiple sclerosis patients correlates with hypointense
lesions on T1 magnetic resonance imaging. J Neurol Sci 2002;
193; 2: 103-9.
64. Rovaris M, Filippi M. Contrast enhancement and the acute lesion
in multiple sclerosis. Neuroimaging Clin N Am 2000; 10; 4: 70516 ,viii-ix.
51. Drayer BP, Burger P, Hurwitz B, Dawson D, Cain J, Leong J,
Herfkens R, Johnson GA. Magnetic resonance imaging in
Page 13 of 18
65. Rubin LL, Staddon JM. The cell biology of the blood-brain barrier.
Annu Rev Neurosci 1999; 22; 11-28.
66. Silver NC, Good CD, Barker GJ, MacManus DG, Thompson AJ,
Moseley IF, McDonald WI, Miller DH. Sensitivity of contrast
enhanced MRI in multiple sclerosis. Effects of gadolinium dose,
magnetization transfer contrast and delayed imaging. Brain
1997; 120; Pt 7: 1149-61.
67. Tofts PS, Kermode AG. Measurement of the blood-brain barrier
permeability and leakage space using dynamic MR imaging. 1.
Fundamental concepts. Magn Reson Med 1991; 17; 2: 357-67.
68. Tortorella C, Codella M, Rocca MA, Gasperini C, Capra R,
Bastianello S, Filippi M. Disease activity in multiple sclerosis
studied by weekly triple-dose magnetic resonance imaging. J
Neurol 1999; 246; 8: 689-92.
69. He J, Grossman RI, Ge Y, Mannon LJ. Enhancing patterns in
multiple sclerosis: evolution and persistence. AJNR Am J
Neuroradiol 2001; 22; 4: 664-9.
demyelination in primates: preliminary in vivo study with MR
and magnetization transfer. AJNR Am J Neuroradiol 1995; 16;
2: 225-31.
80. Dousset V, Grossman RI, Ramer KN, Schnall MD, Young LH,
Gonzalez-Scarano F, Lavi E, Cohen JA. Experimental allergic
encephalomyelitis and multiple sclerosis: lesion characterization
with magnetization transfer imaging. Radiology 1992; 182; 2:
483-91.
81. Dousset V, Armand JP, Lacoste D, Mieze S, Letenneur L,
Dartigues JF, Caill JM. Magnetization transfer study of HIV
encephalitis and progressive multifocal leukoencephalopathy.
Groupe d'Epidemiologie Clinique du SIDA en Aquitaine. AJNR Am
J Neuroradiol 1997; 18; 5: 895-901.
82. Silver NC, Barker GJ, MacManus DG, Miller DH, Thorpe JW,
Howard RS. Decreased magnetisation transfer ratio due to
demyelination: a case of central pontine myelinolysis. J Neurol
Neurosurg Psychiatry 1996; 61; 2: 208-9.
70. Morgen K, Jeffries NO, Stone R, Martin R, Richert ND, Frank JA,
McFarland HF. Ring-enchancement in multiple sclerosis: marker
of disease severity. Mult Scler 2001; 7; 3: 167-71.
83. Kimura H, Grossman RI, Lenkinski RE, Gonzalez-Scarano F.
Proton MR spectroscopy and magnetization transfer ratio in
multiple sclerosis: correlative findings of active versus irreversible
plaque disease. AJNR Am J Neuroradiol 1996; 17; 8: 1539-47.
71. Lee MA, Smith S, Palace J, Narayanan S, Silver N, Minicucci L,
Filippi M, Miller DH, Arnold DL, Matthews PM. Spatial mapping
of T2 and gadolinium-enhancing T1 lesion volumes in multiple
sclerosis: evidence for distinct mechanisms of lesion genesis?
Brain 1999; 122; Pt 7: 1261-70.
84. Loevner LA, Grossman RI, McGowan JC, Ramer KN, Cohen JA.
Characterization of multiple sclerosis plaques with T1-weighted
MR and quantitative magnetization transfer. AJNR Am J
Neuroradiol 1995; 16; 7: 1473-9.
72. McFarland HF, Frank JA, Albert PS, Smith ME, Martin R, Harris
JO, Patronas N, Maloni H, McFarlin DE. Using gadoliniumenhanced magnetic resonance imaging lesions to monitor disease
activity in multiple sclerosis. Ann Neurol 1992; 32; 6: 758-66.
85. Hiehle JF, Jr., Lenkinski RE, Grossman RI, Dousset V, Ramer KN,
Schnall MD, Cohen JA, Gonzalez-Scarano F. Correlation of
spectroscopy and magnetization transfer imaging in the
evaluation of demyelinating lesions and normal appearing white
matter in multiple sclerosis. Magn Reson Med 1994; 32; 3: 28593.
73. Miller DH, Barkhof F, Nauta JJ. Gadolinium enhancement
increases the sensitivity of MRI in detecting disease activity in
multiple sclerosis. Brain 1993; 116; Pt 5: 1077-94.
74. Kappos L, Moeri D, Radue EW, Schoetzau A, Schweikert K,
Barkhof F, Miller D, Guttmann CR, Weiner HL, Gasperini C,
Filippi M. Predictive value of gadolinium-enhanced magnetic
resonance imaging for relapse rate and changes in disability or
impairment in multiple sclerosis: a meta-analysis. Gadolinium
MRI Meta-analysis Group. Lancet 1999; 353; 9157: 964-9.
86. Filippi M, Rocca MA, Rizzo G, Horsfield MA, Rovaris M,
Minicucci L, Colombo B, Comi G. Magnetization transfer ratios
in multiple sclerosis lesions enhancing after different doses of
gadolinium. Neurology 1998; 50; 5: 1289-93.
87. Filippi M, Campi A, Dousset V, Baratti C, Martinelli V, Canal N,
Scotti G, Comi G. A magnetization transfer imaging study of
normal-appearing white matter in multiple sclerosis. Neurology
1995; 45; 3 Pt 1: 478-82.
75. Molyneux PD, Filippi M, Barkhof F, Gasperini C, Yousry TA,
Truyen L, Lai HM, Rocca MA, Moseley IF, Miller DH.
Correlations between monthly enhanced MRI lesion rate and
changes in T2 lesion volume in multiple sclerosis. Ann Neurol
1998; 43; 3: 332-9.
88. Loevner LA, Grossman RI, Cohen JA, Lexa FJ, Kessler D, Kolson
DL. Microscopic disease in normal-appearing white matter on
conventional MR images in patients with multiple sclerosis:
assessment with magnetization-transfer measurements.
Radiology 1995; 196; 2: 511-5.
76. Brex PA, O'Riordan JI, Miszkiel KA, Moseley IF, Thompson AJ,
Plant GT, Miller DH. Multisequence MRI in clinically isolated
syndromes and the early development of MS. Neurology 1999;
53; 6: 1184-90.
89. Rocca MA, Mastronardo G, Rodegher M, Comi G, Filippi M.
Long-term changes of magnetization transfer-derived measures
from patients with relapsing-remitting and secondary progressive
multiple sclerosis. AJNR Am J Neuroradiol 1999; 20; 5: 821-7.
77. van Buchem MA, Tofts PS. Magnetization transfer imaging.
Neuroimaging Clin N Am 2000; 10; 4: 771-788.
90. Tortorella C, Viti B, Bozzali M, Sormani MP, Rizzo G, Gilardi MF,
Comi G, Filippi M. A magnetization transfer histogram study of
normal-appearing brain tissue in MS. Neurology 2000; 54; 1:
186-93.
78. Fralix TA, Ceckler TL, Wolff SD, Simon SA, Balaban RS. Lipid
bilayer and water proton magnetization transfer: effect of
cholesterol. Magn Reson Med 1991; 18; 1: 214-23.
79. Dousset V, Brochet B, Vital A, Gross C, Benazzouz A, Boullerne A,
Bidabe AM, Gin AM, Caille JM. Lysolecithin-induced
91. Rovaris M, Bozzali M, Santuccio G, Iannucci G, Sormani MP,
Colombo B, Comi G, Filippi M. Relative contributions of brain
and cervical cord pathology to multiple sclerosis disability: a
Page 14 of 18
study with magnetisation transfer ratio histogram analysis. J
Neurol Neurosurg Psychiatry 2000; 69; 6: 723-7.
92. Filippi M, Inglese M, Rovaris M, Sormani MP, Horsfield P,
Iannucci PG, Colombo B, Comi G. Magnetization transfer
imaging to monitor the evolution of MS: a 1-year follow-up
study. Neurology 2000; 55; 7: 940-6.
93. Dehmeshki J, Ruto AC, Arridge S, Silver NC, Miller DH, Tofts PS.
Analysis of MTR histograms in multiple sclerosis using principal
components and multiple discriminant analysis. Magn Reson Med
2001; 46; 3: 600-9.
94. Rovaris M, Filippi M, Minicucci L, Iannucci G, Santuccio G, Possa
F, Comi G. Cortical/subcortical disease burden and cognitive
impairment in patients with multiple sclerosis. AJNR Am J
Neuroradiol 2000; 21; 2: 402-8.
95. Filippi M, Rocca MA, Martino G, Horsfield MA, Comi G.
Magnetization transfer changes in the normal appearing white
matter precede the appearance of enhancing lesions in patients
with multiple sclerosis. Ann Neurol 1998; 43; 6: 809-14.
96. Goodkin DE, Rooney WD, Sloan R, Bacchetti P, Gee L,
Vermathen M, Waubant E, Abundo M, Majumdar S, Nelson S,
Weiner MW. A serial study of new MS lesions and the white
matter from which they arise. Neurology 1998; 51; 6: 1689-97.
97. van Waesberghe JH, van Walderveen MA, Castelijns JA, Scheltens
P, Lycklama a Nijeholt GJ, Polman CH, Barkhof F. Patterns of
lesion development in multiple sclerosis: longitudinal
observations with T1-weighted spin-echo and magnetization
transfer MR. AJNR Am J Neuroradiol 1998; 19; 4: 675-83.
98. Dousset V, Gayou A, Brochet B, Caille JM. Early structural
changes in acute MS lesions assessed by serial magnetization
transfer studies. Neurology 1998; 51; 4: 1150-5.
106. Filippi M, Inglese M. Overview of diffusion-weighted magnetic
resonance studies in multiple sclerosis. J Neurol Sci 2001; 186;
Suppl 1: S37-43.
107. Larsson HB, Thomsen C, Frederiksen J, Stubgaard M, Henriksen
O. In vivo magnetic resonance diffusion measurement in the
brain of patients with multiple sclerosis. Magn Reson Imaging
1992; 10; 1: 7-12.
108. Christiansen P, Gideon P, Thomsen C, Stubgaard M, Henriksen
O, Larsson HB. Increased water self-diffusion in chronic plaques
and in apparently normal white matter in patients with multiple
sclerosis. Acta Neurol Scand 1993; 87; 3: 195-9.
109. Tievsky AL, Ptak T, Farkas J. Investigation of apparent
diffusion coefficient and diffusion tensor anisotrophy in acute
and chronic multiple sclerosis lesions. AJNR Am J Neuroradiol
1999; 20; 8: 1491-9.
110. Cercignani M, Iannucci G, Filippi M. Diffusion-weighted imaging
in multiple sclerosis. Ital J Neurol Sci 1999; 20; 5 Suppl: S246-9.
111. Werring DJ, Clark CA, Droogan AG, Barker GJ, Miller DH,
Thompson AJ. Water diffusion is elevated in widespread regions
of normal-appearing white matter in multiple sclerosis and
correlates with diffusion in focal lesions. Mult Scler 2001; 7; 2:
83-9.
112. Clark CA, Werring DJ, Miller DH. Diffusion imaging of the
spinal cord in vivo: estimation of the principal diffusivities and
application to multiple sclerosis. Magn Reson Med 2000; 43; 1:
133-8.
113. Cercignani M, Inglese M, Pagani E, Comi G, Filippi M. Mean
diffusivity and fractional anisotropy histograms of patients with
multiple sclerosis. AJNR Am J Neuroradiol 2001; 22; 5: 952-8.
99. Filippi M. Magnetization transfer imaging to monitor the
evolution of individual multiple sclerosis lesions. Neurology
1999; 53(5; Suppl 3): S18-22.
114. Tourbah A, Stievenart JL, Abanou A, Fontaine B, Cabanis EA,
Lyon-Caen O. Correlating multiple MRI parameters with clinical
features: an attempt to define a new strategy in multiple sclerosis.
Neuroradiology 2001; 43; 9: 712-20.
100. Santos AC, Narayanan S, De Stefano N, Tartaglia MC, Francis SJ,
Arnaoutelis R, Caramanos Z, Antel JP, Pike GB, Arnold DL.
Magnetization transfer can predict clinical evolution in patients
with multiple sclerosis. J Neurol In Press;
115. Wilson M, Morgan PS, Lin X, Turner BP, Blumhardt LD.
Quantitative diffusion weighted magnetic resonance imaging,
cerebral atrophy, and disability in multiple sclerosis. J Neurol
Neurosurg Psychiatry 2001; 70; 3: 318-22.
101. Iannucci G, Tortorella C, Rovaris M, Sormani MP, Comi G,
Filippi M. Prognostic value of MR and magnetization transfer
imaging findings in patients with clinically isolated syndromes
suggestive of multiple sclerosis at presentation. AJNR Am J
Neuroradiol 2000; 21; 6: 1034-8.
116. Castriota Scanderbeg A, Tomaiuolo F, Sabatini U, Nocentini U,
Grasso MG, Caltagirone C. Demyelinating plaques in relapsingremitting and secondary-progressive multiple sclerosis:
assessment with diffusion MR imaging. AJNR Am J Neuroradiol
2000; 21; 5: 862-8.
102. Brex PA, Leary SM, Plant GT, Thompson AJ, Miller DH.
Magnetization transfer imaging in patients with clinically isolated
syndromes suggestive of multiple sclerosis. AJNR Am J
Neuroradiol 2001; 22; 5: 947-51.
117. Nusbaum AO, Tang CY, Wei T, Buchsbaum MS, Atlas SW.
Whole-brain diffusion MR histograms differ between MS
subtypes. Neurology 2000; 54; 7: 1421-7.
103. Cercignani M, Horsfield MA. The physical basis of diffusionweighted MRI. J Neurol Sci 2001; 186; Suppl 1: S11-4.
104. Beaulieu C, Allen PS. Water diffusion in the giant axon of the
squid: implications for diffusion-weighted MRI of the nervous
system. Magn Reson Med 1994; 32; 5: 579-83.
105. Schaefer PW, Grant PE, Gonzalez RG. Diffusion-weighted MR
imaging of the brain. Radiology 2000; 217; 2: 331-45.
118. Roychowdhury S, Maldjian JA, Grossman RI. Multiple sclerosis:
comparison of trace apparent diffusion coefficients with MR
enhancement pattern of lesions. AJNR Am J Neuroradiol 2000;
21; 5: 869-74.
119. Cercignani M, Iannucci G, Rocca MA, Comi G, Horsfield MA,
Filippi M. Pathologic damage in MS assessed by diffusionweighted and magnetization transfer MRI. Neurology 2000; 54;
5: 1139-44.
Page 15 of 18
120. Hagberg G, Valancherry J, Fasano F, Nocentini U, Sabatini U,
Sanes J, Castriota-Scanderbeg A. Co-localization of changes in
ADC, T1 -relaxation time and 1 H-metabolite concentrations in
MS-lesions. Proc Int Soc Magn Reson Med 2001; 9: 153.
(Abstr.)
121. Rocca MA, Cercignani M, Iannucci G, Comi G, Filippi M.
Weekly diffusion-weighted imaging of normal-appearing white
matter in MS. Neurology 2000; 55; 6: 882-4.
spectra of active and chronic multiple sclerosis lesions. Magn
Reson Med 2000; 43; 1: 102-10.
135. Sarchielli P, Presciutti O, Pelliccioli GP, Tarducci R, Gobbi G,
Chiarini P, Alberti A, Vicinanza F, Gallai V. Absolute
quantification of brain metabolites by proton magnetic resonance
spectroscopy in normal-appearing white matter of multiple
sclerosis patients. Brain 1999; 122; Pt 3: 513-21.
122. De Stefano N, Narayanan S, Matthews PM, Francis GS, Antel JP,
Arnold DL. In vivo evidence for axonal dysfunction remote from
focal cerebral demyelination of the type seen in multiple
sclerosis. Brain 1999; 122; Pt 10: 1933-9.
136. van Walderveen MA, Barkhof F, Pouwels PJ, van Schijndel RA,
Polman CH, Castelijns JA. Neuronal damage in T1-hypointense
multiple sclerosis lesions demonstrated in vivo using proton
magnetic resonance spectroscopy. Ann Neurol 1999; 46; 1: 7987.
123. Basser PJ, Pierpaoli C. Microstructural and physiological features
of tissues elucidated by quantitative-diffusion-tensor MRI. J
Magn Reson B 1996; 111; 3: 209-19.
137. Provencher SW. Estimation of metabolite concentrations from
localized in vivo proton NMR spectra. Magn Reson Med 1993;
30; 6: 672-9.
124. Pierpaoli C, Basser PJ. Toward a quantitative assessment of
diffusion anisotropy. Magn Reson Med 1996; 36; 6: 893-906.
138. Pan JW, Twieg DB, Hetherington HP. Quantitative
spectroscopic imaging of the human brain. Magn Reson Med
1998; 40; 3: 363-9.
125. Shimony JS, McKinstry RC, Akbudak E, Aronovitz JA, Snyder
AZ, Lori NF, Cull TS, Conturo TE. Quantitative diffusion-tensor
anisotropy brain MR imaging: normative human data and
anatomic analysis. Radiology 1999; 212; 3: 770-84.
126. Bammer R, Augustin M, Strasser-Fuchs S, Seifert T, Kapeller P,
Stollberger R, Ebner F, Hartung HP, Fazekas F. Magnetic
resonance diffusion tensor imaging for characterizing diffuse and
focal white matter abnormalities in multiple sclerosis. Magn
Reson Med 2000; 44; 4: 583-91.
127. Werring DJ, Clark CA, Barker GJ, Thompson AJ, Miller DH.
Diffusion tensor imaging of lesions and normal-appearing white
matter in multiple sclerosis. Neurology 1999; 52; 8: 1626-32.
128. Iannucci G, Rovaris M, Giacomotti L, Comi G, Filippi M.
Correlation of multiple sclerosis measures derived from T2weighted, T1-weighted, magnetization transfer, and diffusion
tensor MR imaging. AJNR Am J Neuroradiol 2001; 22; 8: 14627.
129. Guo AC, Jewells VL, Provenzale JM. Analysis of normalappearing white matter in multiple sclerosis: comparison of
diffusion tensor MR imaging and magnetization transfer imaging.
AJNR Am J Neuroradiol 2001; 22; 10: 1893-900.
130. Griffin CM, Chard DT, Ciccarelli O, Kapoor B, Barker GJ,
Thompson AI, Miller DH. Diffusion tensor imaging in early
relapsing-remitting multiple sclerosis. Mult Scler 2001; 7; 5:
290-7.
131. Arnold DL, De Stefano N, Narayanan S, Matthews PM. Proton
MR spectroscopy in multiple sclerosis. Neuroimaging Clin N Am
2000; 10; 4: 789-798.
132. Ross B, Bluml S. Magnetic resonance spectroscopy of the human
brain. Anat Rec (New Anat) 2001; 265; 54-84.
133. De Stefano N, Matthews PM, Antel JP, Preul M, Francis G,
Arnold DL. Chemical pathology of acute demyelinating lesions
and its correlation with disability. Ann Neurol 1995; 38; 6: 9019.
134. Helms G, Stawiarz L, Kivisakk P, Link H. Regression analysis of
metabolite concentrations estimated from localized proton MR
139. Moffett JR, Namboodiri MA, Cangro CB, Neale JH.
Immunohistochemical localization of N-acetylaspartate in rat
brain. Neuroreport 1991; 2; 3: 131-4.
140. Simmons ML, Frondoza CG, Coyle JT. Immunocytochemical
localization of N-acetyl-aspartate with monoclonal antibodies.
Neuroscience 1991; 45; 1: 37-45.
141. Urenjak J, Williams SR, Gadian DG, Noble M. Specific expression
of N-acetylaspartate in neurons, oligodendrocyte-type-2
astrocyte progenitors, and immature oligodendrocytes in vitro. J
Neurochem 1992; 59; 1: 55-61.
142. Bhakoo KK, Pearce D. In vitro expression of N-acetyl aspartate
by oligodendrocytes: implications for proton magnetic resonance
spectroscopy signal in vivo. J Neurochem 2000; 74; 1: 254-62.
143. Bjartmar C, Battistuta J, Terada N, Dupree E, Trapp BD. Nacetylaspartate is an axon-specific marker of mature white
matter in vivo: A biochemical and immunohistochemical study
on the rat optic nerve. Ann Neurol 2002; 51; 1: 51-8.
144. Bitsch A, Bruhn H, Vougioukas V, Stringaris A, Lassmann H,
Frahm J, Bruck W. Inflammatory CNS demyelination:
histopathologic correlation with in vivo quantitative proton MR
spectroscopy. AJNR Am J Neuroradiol 1999; 20; 9: 1619-27.
145. Bjartmar C, Kidd G, Mork S, Rudick R, Trapp BD. Neurological
disability correlates with spinal cord axonal loss and reduced Nacetyl aspartate in chronic multiple sclerosis patients. Ann
Neurol 2000; 48; 6: 893-901.
146. Arnold DL, Matthews PM, Francis G, Antel J. Proton magnetic
resonance spectroscopy of human brain in vivo in the evaluation
of multiple sclerosis: assessment of the load of disease. Magn
Reson Med 1990; 14; 1: 154-9.
147. Matthews PM, Francis G, Antel J, Arnold DL. Proton magnetic
resonance spectroscopy for metabolic characterization of plaques
in multiple sclerosis. Neurology 1991; 41; 8: 1251-6.
148. Arnold DL, Matthews PM, Francis GS, O'Connor J, Antel JP.
Proton magnetic resonance spectroscopic imaging for metabolic
characterization of demyelinating plaques. Ann Neurol 1992; 31;
3: 235-41.
Page 16 of 18
149. De Stefano N, Narayanan S, Francis GS, Arnaoutelis R, Tartaglia
MC, Antel JP, Matthews PM, Arnold DL. Evidence of axonal
damage in the early stages of multiple sclerosis and its relevance
to disability. Arch Neurol 2001; 58; 1: 65-70.
150. Mainero C, De Stefano N, Iannucci G, Sormani MP, Guidi L,
Federico A, Bartolozzi ML, Comi G, Filippi M. Correlates of MS
disability assessed in vivo using aggregates of MR quantities.
Neurology 2001; 56; 10: 1331-4.
151. Pan JW, Krupp LB, Elkins LE, Coyle PK. Cognitive dysfunction
lateralizes with NAA in multiple sclerosis. Appl Neuropsychol
2001; 8; 3: 155-60.
152. Mader I, Roser W, Kappos L, Hagberg G, Seelig J, Radue EW,
Steinbrich W. Serial proton MR spectroscopy of contrastenhancing multiple sclerosis plaques: absolute metabolic values
over 2 years during a clinical pharmacological study. AJNR Am J
Neuroradiol 2000; 21; 7: 1220-7.
153. Mader I, Seeger U, Weissert R, Klose U, Naegele T, Melms A,
Grodd W. Proton MR spectroscopy with metabolite-nulling
reveals elevated macromolecules in acute multiple sclerosis. Brain
2001; 124; Pt 5: 953-61.
163. Losseff NA, Webb SL, O'Riordan JI, Page R, Wang L, Barker GJ,
Tofts PS, McDonald WI, Miller DH, Thompson AJ. Spinal cord
atrophy and disability in multiple sclerosis. A new reproducible
and sensitive MRI method with potential to monitor disease
progression. Brain 1996; 119; Pt 3: 701-8.
164. Stevenson VL, Leary SM, Losseff NA, Parker GJ, Barker GJ,
Husmani Y, Miller DH, Thompson AJ. Spinal cord atrophy and
disability in MS: a longitudinal study. Neurology 1998; 51; 1:
234-8.
165. Nijeholt GJ, van Walderveen MA, Castelijns JA, van Waesberghe
JH, Polman C, Scheltens P, Rosier PF, Jongen PJ, Barkhof F.
Brain and spinal cord abnormalities in multiple sclerosis.
Correlation between MRI parameters, clinical subtypes and
symptoms. Brain 1998; 121; Pt 4: 687-97.
166. Lin X, Blumhardt LD. Inflammation and atrophy in multiple
sclerosis: MRI associations with disease course. J Neurol Sci
2001; 189; 1-2: 99-104.
167. Filippi M, Colombo B, Rovaris M, Pereira C, Martinelli V, Comi
G. A longitudinal magnetic resonance imaging study of the
cervical cord in multiple sclerosis. J Neuroimaging 1997; 7; 2:
78-80.
154. Simone IL, Tortorella C, Federico F, Liguori M, Lucivero V,
Giannini P, Carrara D, Bellacosa A, Livrea P. Axonal damage in
multiple sclerosis plaques: a combined magnetic resonance
imaging and 1H-magnetic resonance spectroscopy study. J Neurol
Sci 2001; 182; 2: 143-50.
168. Huber SJ, Bornstein RA, Rammohan KW, Christy JA, Chakeres
DW, McGhee RB. Magnetic resonance imaging correlates of
neuropsychological impairment in multiple sclerosis. J
Neuropsychiatry Clin Neurosci 1992; 4; 2: 152-8.
155. Ogawa S, Lee TM, Kay AR, Tank DW. Brain magnetic resonance
imaging with contrast dependent on blood oxygenation. Proc
Natl Acad Sci U S A 1990; 87; 24: 9868-72.
169. Clark CM, James G, Li D, Oger J, Paty D, Klonoff H. Ventricular
size, cognitive function and depression in patients with multiple
sclerosis. Can J Neurol Sci 1992; 19; 3: 352-6.
156. Reddy H, Narayanan S, Arnoutelis R, Jenkinson M, Antel J,
Matthews PM, Arnold DL. Evidence for adaptive functional
changes in the cerebral cortex with axonal injury from multiple
sclerosis. Brain 2000; 123; Pt 11: 2314-20.
170. Comi G, Filippi M, Martinelli V, Sirabian G, Visciani A, Campi A,
Mammi S, Rovaris M, Canal N. Brain magnetic resonance
imaging correlates of cognitive impairment in multiple sclerosis.
J Neurol Sci 1993; 115; Suppl: S66-73.
157. Rocca MA, Pagani E, Comi G, Filippi M. Brain adaptive changes
following tissue damage in PPMS: a multiparametric study using
fMRI, MTI and DTI. Proc Int Soc Magn Reson Med 2001; 9:
151. (Abstr.)
171. Dastidar P, Heinonen T, Lehtimaki T, Ukkonen M, Peltola J,
Erila T, Laasonen E, Elovaara I. Volumes of brain atrophy and
plaques correlated with neurological disability in secondary
progressive multiple sclerosis. J Neurol Sci 1999; 165; 1: 36-42.
158. Rudick RA, Fisher E, Lee JC, Simon J, Jacobs L. Use of the brain
parenchymal fraction to measure whole brain atrophy in
relapsing-remitting MS. Multiple Sclerosis Collaborative Research
Group. Neurology 1999; 53; 8: 1698-704.
172. Luks TL, Goodkin DE, Nelson SJ, Majumdar S, Bacchetti P,
Portnoy D, Sloan R. A longitudinal study of ventricular volume
in early relapsing-remitting multiple sclerosis. Mult Scler 2000;
6; 5: 332-7.
159. Collins LD, Narayanan S, Caramanos Z, De Stefano N, Tartaglia
MC, Arnold DL. Relation of cerebral atrophy in multiple
sclerosis to severity of disease and axonal injury. Neurology
2000; 54: A17. (Abstr.)
173. Zivadinov R, Sepcic J, Nasuelli D, De Masi R, Bragadin LM,
Tommasi MA, Zambito-Marsala S, Moretti R, Bratina A, Ukmar
M, Pozzi-Mucelli RS, Grop A, Cazzato G, Zorzon M. A
longitudinal study of brain atrophy and cognitive disturbances in
the early phase of relapsing-remitting multiple sclerosis. J Neurol
Neurosurg Psychiatry 2001; 70; 6: 773-80.
160. Simon JH. Brain and spinal cord atrophy in multiple sclerosis:
role as a surrogate measure of disease progression. CNS Drugs
2001; 15; 6: 427-36.
161. Brex PA, Jenkins R, Fox NC, Crum WR, O'Riordan JI, Plant GT,
Miller DH. Detection of ventricular enlargement in patients at
the earliest clinical stage of MS. Neurology 2000; 54; 8: 168991.
162. Liu C, Edwards S, Gong Q, Roberts N, Blumhardt LD. Three
dimensional MRI estimates of brain and spinal cord atrophy in
multiple sclerosis. J Neurol Neurosurg Psychiatry 1999; 66; 3:
323-30.
174. Filippi M, Mastronardo G, Rocca MA, Pereira C, Comi G.
Quantitative volumetric analysis of brain magnetic resonance
imaging from patients with multiple sclerosis. J Neurol Sci 1998;
158; 2: 148-53.
175. Ge Y, Grossman RI, Udupa JK, Babb JS, Nyul LG, Kolson DL.
Brain atrophy in relapsing-remitting multiple sclerosis: fractional
volumetric analysis of gray matter and white matter. Radiology
2001; 220; 3: 606-10.
Page 17 of 18
176. Bakshi R, Czarnecki D, Shaikh ZA, Priore RL, Janardhan V,
Kaliszky Z, Kinkel PR. Brain MRI lesions and atrophy are related
to depression in multiple sclerosis. Neuroreport 2000; 11; 6:
1153-8.
177. Janardhan V, Bakshi R. Quality of life and its relationship to
brain lesions and atrophy on magnetic resonance images in 60
patients with multiple sclerosis. Arch Neurol 2000; 57; 10:
1485-91.
178. Edwards SG, Liu C, Blumhardt LD. Cognitive correlates of
supratentorial atrophy on MRI in multiple sclerosis. Acta Neurol
Scand 2001; 104; 4: 214-23.
179. Fox NC, Jenkins R, Leary SM, Stevenson VL, Losseff NA, Crum
WR, Harvey RJ, Rossor MN, Miller DH, Thompson AJ.
Progressive cerebral atrophy in MS: a serial study using registered,
volumetric MRI. Neurology 2000; 54; 4: 807-12.
180. Simon JH, Jacobs LD, Campion MK, Rudick RA, Cookfair DL,
Herndon RM, Richert JR, Salazar AM, Fischer JS, Goodkin DE,
Simonian N, Lajaunie M, Miller DE, Wende K, MartensDavidson A, Kinkel RP, Munschauer FE, 3rd, Brownscheidle CM.
A longitudinal study of brain atrophy in relapsing multiple
sclerosis. The Multiple Sclerosis Collaborative Research Group
(MSCRG). Neurology 1999; 53; 1: 139-48.
181. Bakshi R, Benedict RH, Bermel RA, Jacobs L. Regional brain
atrophy is associated with physical disability in multiple sclerosis:
semiquantitative magnetic resonance imaging and relationship to
clinical findings. J Neuroimaging 2001; 11; 2: 129-36.
182. Chen JT, Matthews PM, Arnold DL, Zhang Y, Smith SM.
Regional brain atrophy in multiple sclerosis: increasing sensitivity
to differences in relapsing-remitting and secondary-progressive
disease. Proc Int Soc Magn Reson Med 2001; 9: 265. (Abstr.)
183. Paolillo A, Pozzilli C, Gasperini C, Giugni E, Mainero C, Giuliani
S, Tomassini V, Millefiorini E, Bastianello S. Brain atrophy in
relapsing-remitting multiple sclerosis: relationship with 'black
holes', disease duration and clinical disability. J Neurol Sci 2000;
174; 2: 85-91.
184. Sailer M, Losseff NA, Wang L, Gawne-Cain ML, Thompson AJ,
Miller DH. T1 lesion load and cerebral atrophy as a marker for
clinical progression in patients with multiple sclerosis. A
prospective 18 months follow-up study. Eur J Neurol 2001; 8; 1:
37-42.
185. Leist TP, Gobbini MI, Frank JA, McFarland HF. Enhancing
magnetic resonance imaging lesions and cerebral atrophy in
patients with relapsing multiple sclerosis. Arch Neurol 2001; 58;
1: 57-60.
186. Saindane AM, Ge Y, Udupa JK, Babb JS, Mannon LJ, Grossman
RI. The effect of gadolinium-enhancing lesions on whole brain
atrophy in relapsing-remitting MS. Neurology 2000; 55; 1: 61-5.
Page 18 of 18