Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
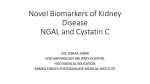
THE ANATOMICAL RECORD 293:1855–1863 (2010) Expressions of Neutrophil GelatinaseAssociated Lipocalin in Gastric Cancer: A Potential Biomarker for Prognosis and an Ancillary Diagnostic Test HUI-JU WANG,1 XU-JUN HE,1 YING-YU MA,1 XIAO-TING JIANG,2 YING-JIE XIA,1 ZAI-YUAN YE,1 ZHONG-SHENG ZHAO,3 AND HOU-QUAN TAO1* 1 Key Laboratory of Gastroenterology of Zhejiang Province, Hangzhou, China 2 Clinical Laboratory, Zhejiang Provincial People’s Hospital, Hangzhou, China 3 Department of Pathology, Zhejiang Provincial People’s Hospital, Hangzhou, China ABSTRACT The aim of this study was to explore the clinical significance of neutrophil gelatinase-associated lipocalin (NGAL) in the development and prognosis of gastric cancer. NGAL tumor levels were determined in 333 GC patients by immunohistochemistry. NGAL in blood samples from 63 healthy donors and 60 gastric cancer patients were also determined by enzyme-linked immunosorbent assay. Rate of NGAL expression was correlated with the size of tumor (69.3% in >4 cm tumors vs. 46.1% in 4 cm tumors), Lauren’s classification (84.3% in diffuse type vs. 28.2% in intestinal type), lymph node metastasis (75.6% vs. 16.4% with no metastasis), vascular invasion (74.9% vs. 26.8% with no invasion), distant metastasis (94.3% vs. 50.3% with no distant metastasis), and TNM stage (81.8% in TNM IIIþIV vs. 20.5% in TNM IþII). NGAL expression can be used as an independent prognostic factor in gastric cancer as indicated by multivariate analysis. Positivity for serum NGAL was higher than that for carbohydrate antigen determinant, CA19-9 (38.1% vs. 12.5%) in TNM I, and higher than that for carcinoembryonic antigen, CEA (58.3% vs. 8.3%) and CA19-9 (58.3% vs. 8.3%) in TNM II. In conclusion, serum NGAL has great potential to be used as an ancillary test for diagnosis of gastric cancer. Increased expression of NGAL in tumors suggests gastric cancer is likely to be at an advanced stage with invasion and metastasis, and also poor C 2010 Wiley-Liss, Inc. prognosis. Anat Rec, 293:1855–1863, 2010. V Key words: NGAL; gastric cancer; neoplasm neoplasm metastasis; diagnosis INTRODUCTION Gastric cancer is one of the most common cancers of the digestive system and its incidence varies significantly in different countries and regions. China is one of the country with a high number of gastric cancer cases (third in the world) (Pavlick et al., 1997) and the main causes appear to be related to environmental, genetic and dietary factors. Based on a survey in the year 2000 (Parkin et al., 2001), the mortality attributed to gastric cancer was 734,000 deaths annually worldwide, which was the second most common cause of cancer mortality, and the incidence of gastric cancer has been increasing year on year. Biomarkers have been widely used for C 2010 WILEY-LISS, INC. V invasiveness; Additional supporting information can found in the online version of this article. Grant sponsor: Zhejiang Province Nature Science Foundation of China; Grant number: Y207763; Grant sponsor: Zhejiang Provincial Program for the Cultivation of High-level Innovative Health Talents. *Correspondence to: Hou-Quan Tao, Key Laboratory of Gastroenterology of Zhejiang Province, Hangzhou 310014, Zhejiang, China. Fax: 0086-571-85131448. E-mail: [email protected] Hui-Ju Wang, Xu-Jun He, and Ying-Yu Ma contributed equally to this work. Received 24 February 2010; Accepted 9 June 2010 DOI 10.1002/ar.21230 Published online 20 August 2010 in Wiley Online Library (wileyonlinelibrary.com). 1856 WANG ET AL. screening and early detection of gastric cancer for many years, and can be relatively specific such as serum prostate-specific antigen for prostatic cancer (Brawer et al., 1993; Catalona et al., 1993), serum carcinoembryonic antigen (CEA) with high specificity but insufficient sensitivity for detection of colorectal cancer (CRC) recurrence in isolation (Tan et al., 2009), and carbohydrate antigen determinant 19-9 (CA19-9) for pancreatic/bile duct cancers (Wu et al., 2006). However, there is no adequate marker that has been developed and proven to be useful clinically for diagnosis and prognosis of gastric cancer and the lack of such biomarker(s) may have contributed to the high mortality of gastric cancer in all cancer cases. As in other cancers, the stage of the tumor (depth of invasion and metastasis) is the key factor in prognosis and often determines the overall survival rate. The process of tumor invasion and metastasis involves multiple steps, although these are not yet fully understood, including tumor cell adhesion, interaction with the surrounding matrix and migration. A biomarker that is biologically associated with the process and is linked functionally with later cancer stage would allow us to predict high risk of invasion and metastasis, and would be of great value. Neutrophil gelatinase-associated lipocalin (NGAL), a member of the lipocalin family, was originally identified as a protein stored in specific granules of human neutrophils (Kjeldsen et al., 1993). It was observed to form a complex with the gelatinase, matrix metalloproteinase-9 (MMP-9), and is composed of 178 amino acids (Kjeldsen et al., 1993). It belongs to the lipocalin family (Flower, 1996) which comprises more than 50 known members, all of which are characterized by their low molecular weight and their ability to bind to and transport a group of small lipophilic substances. NGAL exists as a 25 kDa monomer, a 46 kDa disulfide-linked homodimer, and a 135 kDa disulfide-linked heterodimer with neutrophil gelatinase (Kjeldsen et al., 1994). A cell type-specific pattern of expression was seen in bronchus, stomach, small intestine, pancreas, kidney, prostate gland, and thymus (Friedl et al., 1999). In recent years, NGAL was found abnormal expression in many malignant tumors such as esophageal cancer (Zhang et al., 2007), ovarian cancer (Lim et al., 2007), and pancreatic cancer (Furutani et al., 1998). Because its expression was often associated with a later stage of cancer, a role in tumor invasion and metastasis was, therefore, proposed, and it was also considered an independent indicator of poor prognosis for some of the tumors (Bauer et al., 2008). The characteristics of NGAL expression in gastric cancer are still largely unknown. In this article, we studied neoplasm expression of NGAL in 333 cases of gastric cancers using immunohistochemical staining, serum levels of NGAL in 60 patients using sandwich enzymelinked immunosorbent assay (ELISA) and NGAL expression in five gastric cancer cell lines using reverse transcription-polymerase chain reaction (RT-PCR) and Western blot analysis. The correlation between NGAL expression and tumor invasion and metastasis, and the significance of serum NGAL levels were analyzed. tiation), SGC-7901 (moderate differentiation), BGC-823 (poor differentiation), AGS (poor differentiation), KatoIII (poor differentiation) were kindly provided by the Digestive Surgery Institution, Ruijin Hospital of Shanghai (Shanghai, China). They were cultured in RPMI 1640 supplemented with 10% fetal bovine serum and antibiotics (100 U/mL streptomycin and 100 U/mL penicillin) and maintained at 37 C with 5% CO2. Cells were passaged at 80% confluency using 1 mmol/L EDTA0.025% trypsin for 3–5 minutes. Tissue Samples Paraffinized specimens of tumors from 333 gastric cancer patients who underwent curative gastrectomy between 1995 and 2003 at the Department of Surgery (Zhejiang Provincial People’s Hospital, Hangzhou, China) were included. Written informed consent for experimental immunohistochemistry was obtained from all patients before analysis. The gastric cancer patients were aged between 17 and 80 years old and had not received radiotherapy or chemotherapy before surgery. All of the cases were classified according to the WHO Pathological Classification of Tumors, including 7 cases of high differentiation, 101 cases of moderate differentiation, and 225 cases of poor differentiation. Fourteen cases of papillary adenocarcinoma, 248 cases of tubular adenocarcinoma, 23 cases of mucinous adenocarcinoma, and 48 cases of signet-ring cell carcinoma according to the histological classification. One-hundred seventy-four cases of intestinal type and 159 cases of diffuse type according to the Lauren classification. Two-hundred seventeen cases with lymph node metastasis and 116 cases without lymph node metastasis. Seventy-three cases at TNM stage I, 73 cases at TNM stage II, 138 cases at TNM stage III, and 49 cases at TNM stage IV. Full follow-up data over 5 years, until December 2008, were recorded for all patients. In addition, 53 non-neoplastic paraffinized specimens from normal gastric mucosa (n ¼ 26), gastritis (n ¼ 8), and dysplasia (n ¼ 10) obtained by endoscopic biopsies, and gastric ulcer (n ¼ 9) obtained by surgery, were examined after obtaining appropriate consent. Blood Samples and Isolation of Serum Blood samples from 60 among the 333 gastric cancer patients above (42 males and 18 females, mean age 56.1 years, range, 27–70) were also obtained. Sera from 63 healthy donors (35 males and 28 females, mean age 41.9 years, range, 25–65) were collected from October 2007 to February 2008. Whole blood was transferred from an anticoagulant citrate dextrose solution formula A-capped tube to a conical tube. Samples were centrifuged for 10 min at 1,500g in a swing bucket rotor at 4 C, and the serum was stored in cryovials at 80 C. The project was approved by the ethics committee of Zhejiang Provincial People’s Hospital. RNA Isolation and RT-PCR Analysis MATERIALS AND METHODS Cell Lines Five gastric adenocarcinoma cell lines at different levels of differentiation including MKN45 (poor differen- Total RNA from cell lines was isolated by Trizol (Invitrogen). A total of 2 lg RNA was reverse-transcribed using the SuperScript II RNase-Reverse Transcriptase System (Invitrogen). The cDNA was then subjected to NGAL IN GC DIAGNOSIS AND PROGNOSIS PCR with 1.5 mM magnesium chloride, 2.5U Taq polymerase in a total volume of 25 lL and specific primers for NGAL. After 4 min initial denaturation at 94 C, 30 cycles of amplification (94 C for 30 s, 51 C for 30 s, 72 C for 30 s) were performed. Beta-actin was used as an internal control. The PCR products were electrophoretically resolved on 1% agarose gels stained with ethidium bromide. Photographs were taken under ultraviolet light, using the FluorChem software system (Alpha Innotech). The primers of the forward and reverse for NGAL (accession number: NM_005564.3) are 50 -GCA CCA ACT ACA ACC AGC AT-30 and 50 -TTG GGA CAG GGA AGA CGA T-30 (Invitrogen), respectively. The DNA markers were bought from Beijing Dingguo Biotechnology Company, China. 1857 (provided by the manufacturer), sample (gastric cancer, or healthy control serum sample), or sample diluent alone (blank) was rapidly added to a 96-well plate precoated with NGAL antibody and incubated in 37 C for 120 min. Thereafter, 100 lL biotin-antibody working solution was added to each well and incubated in 37 C for 60 min and 100 lL horseradish peroxidase-avidin working solution was added to each well. After incubated at 37 C for 60 min, the contents of the microwell were aspirated and replaced with 90 lL of the chromogenic peroxidase substrate tetramethylbenzidine. The plate was incubated for 30 min at 37 C (protected from light), then the reaction was stopped by adding 50 lL ‘‘stop solution,’’ and the absorbance at 450 nm was read with a microplate reader. Cell Lysates and Western Blot Cells were lysed in modified RIPA buffer (50 mM TrisHCl, pH 7.4, 0.25% Na deoxycholate, 150 mM NaCl, 1% NP-40, 1 mM EDTA). Total cellular proteins were extracted on ice for 30 min and centrifugated at 16,000g for 10 min. The supernatant was collected and stored at 80 C until further use. Samples were run on 10% sodium dodecyl sulfate-polyacrylamide gels and transfered onto polyvinylidene difluoride membranes. The membranes were blocked in 5% bovine serum albumin and subsequently exposed to primary antibodies specific for NGAL (rat monoclonal anti-NGAL antibody, R&D systems, 1 lg/lL in PBS). After incubation with the appropriate secondary antibody, the membranes were treated with ECL reagent (Generay, China) and exposed to autoradiographic films. Beta-actin was also detected as an internal control. Immunohistochemical Staining Briefly, each tissue section was deparaffinized, rehydrated and then incubated with fresh 3% hydrogen peroxide for 10 min. After rinsing with PBS, high pressure antigen retrieval from the tissue was carried out in 0.01 M citrate buffer (pH 6.0). Next, sections were incubated with 10% normal goat serum for 15 min at room temperature. After rinsing with PBS, slides were incubated with rat anti-human NGAL monoclonal antibody (1:60 dilution in PBS, R&D Systems) overnight at 4 C. After rinsing with PBS, tissue sections were incubated for 20 min at room temperature with biotin-labeled secondary antibody. After rinsing with PBS, tissue sections were incubated for 20 min at room temperature with horseradish peroxidase polymer conjugate (Zymed). Subsequently, they were stained with 3,3-diaminobenzidine, counterstained with hematoxylin, dehydrated and mounted. Meanwhile, primary antibody replaced by PBS was used as negative control. Determination of Serum NGAL Levels by Sandwich ELISA The concentration of NGAL in the serum of patients was determined using the NGAL ELISA Kit (Cusabio Biotech). Serum samples from 60 patients with gastric cancer were tested. Sera from 63 healthy donors were used as control. A volume of 100 lL each of the standard Measurement of Serum CEA and CA19-9 CEA and CA19-9 were measured with a commercially available automated immunoassay method (Modular Analytics, Roche Diagnostics) according to the manufacturer’s instructions. The upper limits of normal for this method are 5.0 ng/mL for CEA and 37 U/mL for CA19-9. Statistical Analysis All slides were observed under a Nikon Light Microscope and representative photographs were taken. The intensity of immunoreactivity of NGAL was scored. The staining intensity was graded on a scale of 0 to 3þ (0 for no staining, 1þ for weak immunoreactivity, 2þ for moderate immunoreactivity, and 3þ for strong immunoreactivity). The percentage of cells that showed positive NGAL staining within the normal/cancerous region of a section was scored as follows: 1: 0%–25% of cells positive, 2: 26%–50% positive, 3: 51%–75% positive, and 4: 76%–100% positive for NGAL. The staining intensity score and the percent immunoreactivity score were then multiplied to obtain a composite score. The values of the composite score ranged from a minimum of 0 to a maximum of 12, and 0 to 3 was defined as negative, 4 was defined as positive. Statistical analyses of the data were performed with SPSS V13.0 software. With regard to immunohistochemistry results provided by categorical scoring system, Mann-Whitney U test was employed to compare two groups of unpaired values, whereas for comparisons between groups of more than two unpaired values, we performed the Kruskal-Wallis H-test. The two independent sample t test was used to compare the mean serum NGAL value between normal and gastric cancer samples. Correlations between TNM stage and serum NGAL, CEA, CA19-9 were estimated by McNemar paired-sample v2 test. The correlation of NGAL expression between serum and tissue was reported as Spearman’s product–moment correlation coefficients (rs). Survival curves were constructed using the method of Kaplan and Meier, including the Log-rank test. The Cox proportional hazards model for multivariate survival analysis was used to assess predictors related to survival. All statistical tests were two-tailed, differences were considered significant when P < 0.05. 1858 WANG ET AL. RESULTS NGAL Expression in Gastric Cancer Cell Lines As shown in Fig. 1A, all five levels of differentiated gastric cancer cell lines expressed NGAL. To confirm this result, cell lysates from these cells were subjected to Western blotting with anti-NGAL antibodies (Fig. 1B). Consistent with the RT-PCR results, MKN-45, SGC7901, BGC-823, and AGS cells had high levels of NGAL protein expression. However, the expression of NGAL was dramatically lower in Kato-III cells than in any other cells. Immunohistochemical Staining Analysis Fig. 1. (A) Reverse transcription-polymerase chain reaction for neutrophil gelatinase-associated lipocalin (NGAL) expression by using NGAL-specific primers with beta-actin as an internal control. (B) NGAL expression was determined by Western blot analyses of protein lysates from gastric cancer cells with beta-actin as an internal control. Fig. 2. Results of NGAL immunohistochemistry, original magnification 200, the insert panes show the sections indicated by the arrows at a magnification of 400. (A) Hematoxylin-eosin (HE) staining in poorly-differentiated adenocarcinoma. (B) Immunostaining of NGAL (yellow-brown granules, mainly in the cytoplasm) in poorly-differentiated adenocarcinoma. (C) HE staining in moderately-differentiated adenocarcinoma. (D) Immunostaining of NGAL in moderately-differentiated adenocarcinoma. (E) HE staining at the edge of the adenocarcinoma with tumor invasion. (F) Immunostaining of NGAL at the edge of the adenocarcinoma with tumor invasion. (G) HE staining in a lymph Specimens from a total of 333 gastric cancer patients with positive staining for NGAL showed cytoplasmic yellow-brown granules (Fig. 2B,D) with appropriate negative control (Fig. 2L, PBS replacing primary antibody against NGAL). The NGAL-positive detection rate was 55.0% (183/333) in the gastric carcinoma specimens, and the NGAL detection rate was statistically correlated with the tumor size, Lauren classification, lymph node node with metastasis in poorly-differentiated gastric adenocarcinoma. (H) Immunostaining of NGAL in a lymph node with metastasis in poorly-differentiated gastric adenocarcinoma. (I) HE staining in a lymph node with metastasis in moderately-differentiated gastric adenocarcinoma. (J) Immunostaining of NGAL in a lymph node with metastasis in moderately-differentiated gastric adenocarcinoma. (K) HE staining in gastric adenocarcinoma. (L) Negative control for immunostaining of NGAL, with phosphate-buffered saline replacing primary antibody against NGAL. 1859 NGAL IN GC DIAGNOSIS AND PROGNOSIS TABLE 1. Correlation of NGAL expression and clinicopathological features of 333 gastric cancers NGAL expression Characteristics Sex Male Female Tumor diameter 4 cm >4 cm Lauren classification Diffuse type Intestinal type Differentiation Well Moderate Poor Histology type Papillary adenocarcinoma Tubular adenocarcinoma Mucinous adenocarcinoma Signet-ring cell carcinoma Lymph node metastasis No Yes Vascular invasion No Yes Distance metastasis No Yes TNM stage I þ II III þ IV Negative Positive P value 116 34 121 (51.1%) 62 (64.6%) 0.025 111 39 95 (46.1%) 88 (69.3%) 0.000 25 125 134 (84.3%) 49 (28.2%) 0.000 5 43 102 2 (28.6%) 58 (57.4%) 123 (54.7%) 0.329 6 115 6 23 8 133 17 25 (57.1%) (53.6%) (73.9%) (52.1%) 0.295 97 53 19 (16.4%) 164 (75.6%) 0.000 101 49 37 (26.8%) 146 (74.9%) 0.000 148 2 150 (50.3%) 33 (94.3%) 0.000 116 34 30 (20.5%) 153 (81.8%) 0.000 metastasis, vascular invasion, distant metastasis, and TNM stage (Table 1). The detection rate of NGAL was 69.3% (88/127) in gastric carcinoma specimens of tumor size >4 cm, which was higher than that in specimens of tumor size 4 cm (46.1%, 95/206, P < 0.001). The frequency of NGAL positivity in samples from patients with diffuse histological type (84.3%, 134/159) was significantly higher than that in patients with intestinal histological type (28.2%, 49/174, P < 0.001). NGAL was detected in 75.6% (164/217) of gastric cancer specimens with lymph node metastasis, which was higher than in specimens without lymph node metastasis (16.4%, 19/ 116, P < 0.001). The detection rates of NGAL were 74.9% (146/195) and 94.3% (33/35) in specimens with vascular invasion and distant metastasis, which were higher than in specimens without vascular invasion (26.8%, 37/138, P < 0.001) or distant metastasis (50.3%, 150/298, P < 0.001). NGAL was detected in 20.5% (30/ 146) of TNM stage IþII samples, which was lower than in TNM stage IIIþIV samples where it was detected in 81.8% (153/187, P < 0.001). NGAL expression appeared to be greater in infiltrating tumor cells bordering the adjacent normal tissue (Fig. 2F) and metastatic foci in the lymph nodes were often positive (Fig. 2H,J), which was consistent with the proposition that NGAL is involved in tumor invasion and metastasis. The mean survival time in patients positive for NGAL was 35.58 1.16 months, which was significantly lower than in patients negative for NGAL (54.37 0.71 months, P < 0.001). The 5-year survival rate in patients Fig. 3. Kaplan-Meier survival curve of gastric cancer patients positive and negative for NGAL expression. TABLE 2. Multivariate analysis as determined by Cox regression analysis in 333 gastric cancer patients 95% Confidential interval Clinicopathological parameters Lower Upper Hazard ratio P value Lauren classification Vascular invasion TNM stage NGAL expression 1.571 1.176 1.048 1.217 3.466 2.766 2.625 2.788 2.334 1.804 1.659 1.842 0.000 0.007 0.031 0.004 with NGAL expression was significantly lower (20.8%) than in patients without NGAL expression (66%, P < 0.001) (Fig. 3). Cox multivariate analysis showed that survival was independently correlated with Lauren classification, vascular invasion, TNM stage and NGAL expression (Table 2). To evaluate the profile of NGAL in the carcinogenesis of gastric cancer, we separately characterized the pattern of expression of NGAL in non-neoplastic gastric tissues. In normal gastric mucosa, NGAL staining was observed in neutrophils which invaded glands of the lamina propria in gastritis, however, no NGAL expression was detected in normal gastric epithelial cells. In gastric ulcers, NGAL staining was only detected in neutrophils of necrosis foci. All the dysplasia was positive for NGAL expression (Fig. 4). This suggested that the expression of NGAL was up-regulated in the early stages of gastric carcinogenesis. Quantitative ELISA for NGAL Levels in Serum The serum levels of NGAL in normal versus gastric cancer samples were analyzed by the two independent sample t test. It showed that the NGAL level was high in gastric cancer patients, but very low in healthy donors (P < 0.001, Supporting Information Table 1). A 1860 WANG ET AL. Fig. 4. NGAL staining analysis in tissue of normal and gastric dysplasia. (A) HE staining in normal gastric tissue. (B) NGAL expression in normal tissue was negative. (C) HE staining in tissue of chronic gastritis in the active phase. (D) NGAL staining was detected in neutrophilic granulocytes when they invaded lamina propria glands in chronic gastritis in the active phase. (E) HE staining in gastric ulcer. (F) NGAL positive staining was detected in neutrophilic granulocytes of necrosis foci in the gastric ulcer, but was negative in any other location. (G) HE staining in tissue of gastric dysplasia. (H) NGAL expression was positive in tissue of gastric dysplasia. receiver operating characteristic (ROC) curve analysis revealed that the area under the curve was 0.927, suggesting that the test was fairly accurate in classifying cases as ‘cancer’ or ‘‘noncancer’’ (Fig. 5). Relation of NGAL Expression Between Serum and Tissue When considering the relationship of NGAL expression between serum and tissue, a direct correlation was observed between serum NGAL levels and NGAL expression in gastric cancer. Twenty of the 26 cases with an increased level of serum NGAL showed strong positive immunostaining of tumor cells, while only 13 of the 34 cases with normal serum levels of NGAL exhibited positivity (R ¼ 0.385, P ¼ 0.002, Spearman’s q-test). Relation Between Serum Concentrations of NGAL, CEA, CA19-9, and TNM Stage Simultaneously, we analyzed serum levels of CEA and CA19-9 in the 60 gastric caner patients, and the data of serum NGAL, CEA, and CA19-9 were listed in Supporting Information Table 2. Using an established cutoff for healthy individuals of 14.31 ng/mL (the mean level þ 2 standard deviations in healthy controls), the detection rate of serum NGAL reached 43.3% in the gastric cancer samples. In contrast to serum levels of CEA and CA19-9 (CEA level >5 ng/mL and CA19-9 level >37 U/mL were considered positive), the positive rate of serum NGAL (38.1%) was significantly higher than serum CA19-9 (12.5%, P ¼ 0.016) in TNM stage I, and was significantly higher than serum CEA (58.3% vs. 8.3%, P ¼ 0.031) and CA19-9 (58.3% vs. 8.3%, P ¼ 0.031) in TNM stage II (Table 3). DISCUSSION Proteins secreted by malignant cells that degrade the extracellular matrix often play a key role in tumor inva- Fig. 5. Receiver operating characteristic (ROC) curve analysis of diagnostic sensitivity and specificity of the serum NGAL enzymelinked immunosorbent assay. The performance of the assay in discriminating patients with gastric cancer from normal subjects was evaluated. The area under the curve was 0.927, suggesting that the test was fairly accurate in distinguishing between the two groups. sion and metastasis. MMP is one of the most important proteins associated with tumor invasion and metastasis, and can not only degrade the basement membrane and matrix to promote tumor invasion and metastasis, but also promote tumor growth and proliferation by angiogenesis. NGAL was originally found as a protein stored 1861 NGAL IN GC DIAGNOSIS AND PROGNOSIS TABLE 3. Correlation between TNM stage and serum NGAL, CEA, CA19–9 in 60 gastric cancers TNM stage I II III IV Rate of expression positive for NGAL 38.1% 58.3% 41.2% 40.0% (8/21) (7/12) (7/17) (4/10) Rate of expression positive for CEA 14.3% 8.3% 17.6% 50.0% (3/21) (1/12) (3/17) (5/10) Rate of expression positive for CA199 12.5% 8.3% 23.5% 10.0% (1/21) (1/12) (4/17) (1/10) P1 value P2 value 0.227 0.031 0.289 1.000 0.016 0.031 0.508 0.375 Using an established cutoff for healthy individuals (14.31 ng/ml), 14.31 ng/ml was positive for NGAL; and 5 ng/ml was positive for CEA, 37 U/ml was positive for CA19–9; P1: NGAL versus CEA; P2: NGAL versus CA19–9. in specific granules of human neutrophils (Elneihoum et al., 1996), and can bind and mediate the activity of MMP-9 (Yan et al., 2001). It can also bind bacterial siderophores, preventing bacteria from retrieving iron from this source (Goetz et al., 2002; Yang et al., 2002). Elevated NGAL expression was also observed in human cancers such as colorectal, breast, pancreatic and ovarian cancers (Furutani et al., 1998; Friedl et al., 1999; Lim et al., 2007; Zhang et al., 2007), may participate in tumor invasion and is associated with poor differentiation of cancer cells (Kubben et al., 2007; Bauer et al., 2008). NGAL could act as a biomarker for the early stages of pancreatic cancer, as evidenced by the fact that well to moderately differentiated pancreatic cancer cells had very high levels of NGAL expression, whereas NGAL expression in poorly differentiated pancreatic cancer cell lines was undetectable (Moniaux et al., 2008; Tong et al., 2008). Interestingly, NGAL overexpression in this case actually reduced pancreatic cancer cell adhesion and, therefore, invasion in vitro and in vivo (Tong et al., 2008). To support this idea, Lee et al. (2006) reported that the overexpression of NGAL blocked human colon cancer KM12SM cell invasion and liver metastasis. In contrast, Li et al. (2003) reported the downregulation of NGAL by antisense suppressed human esophageal carcinoma SHEEC cell invasion in vivo. These apparently conflicting observations could be result from distinct functions of NGAL in different cell types. Our current study demonstrated that NGAL was expressed in most of the gastric cancer cell lines, indicating that NGAL is expressed universally in cancers originally from gastric epithelium. No significant differences of NGAL expression were observed in MKN45, SGC-7901, BGC-823, AGS and Kato-III cell lines. The results indicated that NGAL expression was not correlated with the degree of differentiation of gastric cancer. The expression of NGAL has been demonstrated in several other types of cancer, such as carcinoma of lung (Friedl et al., 1999), gastric cancer (Kubben et al., 2007), breast cancer (Stoesz et al., 1998), colon cancer (Nielsen et al., 1996), pancreatic cancer (Argani et al., 2001; Han et al., 2002), and ovarian cancer (Bartsch and Tschesche, 1995). However, no expression was detected in lymphoma and thymic carcinoma (Friedl et al., 1999). Our study found that NGAL expression was significantly higher in gastric cancer than that in normal tissue, suggesting that the expression of NGAL in cancer has tissue specificity. Findings of research on esophageal squamous cell carcinoma (ESCC) suggested that NGAL was involved in the differentiation pathway and invasive progression of ESCC (Zhang et al., 2007), but another study found that the NGAL expression was not only suppressing the ability of colon carcinoma cells to invade Matrigel in vitro, but also substantially inhibited liver metastasis in an experimental animal model (Lee et al., 2006). Our study found that the NGAL detection rate was statistically correlated with tumor size, Lauren classification, lymph node metastasis, vascular invasion, distant metastasis, and TNM stage. The frequency of positivity for NGAL in cases with tumor size >4 cm was higher than in tumors 4 cm, and was higher in cases with diffuse histological type (84.3%) than those with intestinal histological type (28.2%), and was also higher in cases with lymph node metastasis (75.6%), vascular invasion (74.9%), and distant metastasis (94.3%) and TNM IIIþIV staging (81.8%) than in those without lymph node metastasis (16.4%), vascular invasion (26.8%) or distant metastasis (50.3%) and with TNM IþII staging (20.5%). Therefore, NGAL may play an important role in invasion and metastasis of gastric cancer. In recent years, the MMP family has been found to play an important role in tumor invasion, metastasis and recurrence (Takahashi et al., 2002; Masaki et al., 2003; Curran et al., 2004). Collagen IV, which is a major component of basement membrane, also acts as a natural barrier of cancer infiltration, and MMP-9 is one of the IV collagenases. In vitro experiments suggested a possible role for NGAL in the protection of MMP-9 against autolysis. In vivo data showed that enhanced levels of MMP-9/NGAL complexes were significantly correlated with the classifications of Lauren, and highly associated with worse survival in gastric cancer (Kubben et al., 2007). Although this article did not measure MMP-9 levels in samples, we also have reason to believe, in light of Bubben’s previous work, that overexpression of NGAL in gastric cancer may be associated with the activity of MMP-9, thereby promoting the invasion and metastasis of gastric cancer. NGAL overexpression was significantly correlated with poor prognosis, suggesting that NGAL may participate in the progression of gastric cancer, and may be an indicator for poor prognosis of gastric cancer patients. We also found that NGAL expression was negative in normal gastric glands, apart from neutrophils in gastritis and gastric ulcer. However, all the gastric dysplasias were positive for NGAL expression. Our results indicate that NGAL is upregulated in the early stage of gastric carcinogenesis and may play an important role in the early development of gastric cancer. The results also suggest that NGAL could serve as an early diagnostic marker for gastric cancer especially in fine needle aspirates or endoscopically-obtained biopsies. Serum NGAL level has been shown to be elevated early in acute renal injury (Mishra et al., 2005; Dent et al., 2007) and ovarian borderline cancer (Lim et al., 1862 WANG ET AL. 2007). The NGAL-MMP level was significantly higher in the urine of breast cancer patients than in normal subjects, and the detection rate was nearly 84% (Fernandez et al., 2005). Studies (Moniaux et al., 2008) have also suggested that the serum NGAL level could be explored as a possible diagnostic marker in pancreatic cancer in the appropriate clinical context. Our research found that serum NGAL levels in gastric cancer patients was higher than that in healthy donors indicating that serum NGAL was associated with gastric cancer and can be a significant index for diagnosis. To confirm that the serum NGAL detected by our ELISA was derived from tumor cells, we performed immunohistochemical analysis in all 60 gastric cancer specimens from patients whose serum NGAL was tested. Summarizing the correlation between serum NGAL levels and NGAL expression in gastric cancer, 20 of the 26 cases with an increased level of serum NGAL also showed strong positive immunostaining of tumor cells, while only 13 of the 34 cases with normal serum levels of NGAL exhibited positivity. A significant correlation was observed between serum NGAL level and NGAL expression in tumor cells (P < 0.05), suggesting that the serum NGAL levels could be derived from tumor cells. Although serum markers such as CA19-9 and CEA were highly elevated in a few patients with advanced gastric cancer, these conventional markers are usually not elevated in earlystage gastric cancer, and thus are not useful for detecting such cancers. ROC curve analysis revealed that the area under the curve was 0.927 indicating our test was fairly accurate in classifying cases as ‘cancer’ or ‘noncancer’. Since serum NGAL behaves in a different manner from CA19-9 or CEA, serum NGAL is likely to be more effective than serum CA19-9 or CEA in distinguishing between patients with gastric cancer from healthy controls. Notably, the present study showed that the rate of positive serum NGAL expression was significantly higher than for serum CA19-9 in TNM stage I, and was significantly higher than for serum CEA and CA19-9 in TNM stage II. This suggests that serum NGAL might have some potential to help detect early gastric cancer. However, to clearly determine this, further studies analyzing a large number of patients with early-stage gastric cancer are required. In conclusion, measurement of serum NGAL has great potential as an ancillary test for diagnosis of gastric cancer, and high expression of NGAL in gastric cancer tissues indicates tumor metastasis and poor prognosis. Therefore, NGAL can be used as an indicator of invasion, metastasis and poor prognosis of gastric cancer. The specific role of NGAL requires further elucidation in future studies. LITERATURE CITED Argani P, Rosty C, Reiter RE, Wilentz RE, Murugesan SR, Leach SD, Ryu B, Skinner HG, Goggins M, Jaffee EM, Yeo CJ, Cameron JL, Kern SE, Hruban RH. 2001. Discovery of new markers of cancer through serial analysis of gene expression: prostate stem cell antigen is overexpressed in pancreatic adenocarcinoma. Cancer Res 61:4320–4324. Bartsch S, Tschesche H. 1995. Cloning and expression of human neutrophil lipocalin cDNA derived from bone marrow and ovarian cancer cells. FEBS Lett 357:255–259. Bauer M, Eickhoff JC, Gould MN, Mundhenke C, Maass N, Friedl A. 2008. Neutrophil gelatinase-associated lipocalin (NGAL) is a predictor of poor prognosis in human primary breast cancer. Breast Cancer Res Treat 108:389–397. Brawer MK, Beatie J, Wener MH, Vessella RL, Preston SD, Lange PH. 1993. Screening for prostatic carcinoma with prostate specific antigen: results of the second year. J Urol 150:106–109. Catalona WJ, Smith DS, Ratliff TL, Basler JW. 1993. Detection of organ-confined prostate cancer is increased through prostatespecific antigen-based screening. JAMA 270:948–954. Curran S, Dundas SR, Buxton J, Leeman MF, Ramsay R, Murray GI. 2004. Matrix metalloproteinase/tissue inhibitors of matrix metalloproteinase phenotype identifies poor prognosis colorectal cancers. Clin Cancer Res 10:8229–8234. Dent CL, Ma Q, Dastrala S, Bennett M, Mitsnefes MM, Barasch J, Devarajan P. 2007. Plasma neutrophil gelatinase-associated lipocalin predicts acute kidney injury, morbidity and mortality after pediatric cardiac surgery: a prospective uncontrolled cohort study. Crit Care 11:R127. Elneihoum AM, Falke P, Axelsson L, Lundberg E, Lindgarde F, Ohlsson K. 1996. Leukocyte activation detected by increased plasma levels of inflammatory mediators in patients with ischemic cerebrovascular diseases. Stroke 27:1734–1738. Fernandez CA, Yan L, Louis G, Yang J, Kutok JL, Moses MA. 2005. The matrix metalloproteinase-9/neutrophil gelatinase-associated lipocalin complex plays a role in breast tumor growth and is present in the urine of breast cancer patients. Clin Cancer Res 11: 5390–5395. Flower DR. 1996. The lipocalin protein family: structure and function. Biochem J 318 (Part 1):1–14. Friedl A, Stoesz SP, Buckley P, Gould MN. 1999. Neutrophil gelatinase-associated lipocalin in normal and neoplastic human tissues. Cell type-specific pattern of expression. Histochem J 31:433–441. Furutani M, Arii S, Mizumoto M, Kato M, Imamura M. 1998. Identification of a neutrophil gelatinase-associated lipocalin mRNA in human pancreatic cancers using a modified signal sequence trap method. Cancer Lett 122:209–214. Goetz DH, Holmes MA, Borregaard N, Bluhm ME, Raymond KN, Strong RK. 2002. The neutrophil lipocalin NGAL is a bacteriostatic agent that interferes with siderophore-mediated iron acquisition. Mol Cell 10:1033–1043. Han H, Bearss DJ, Browne LW, Calaluce R, Nagle RB, Von Hoff DD. 2002. Identification of differentially expressed genes in pancreatic cancer cells using cDNA microarray. Cancer Res 62:2890–2896. Kjeldsen L, Bainton DF, Sengelov H, Borregaard N. 1994. Identification of neutrophil gelatinase-associated lipocalin as a novel matrix protein of specific granules in human neutrophils. Blood 83: 799–807. Kjeldsen L, Johnsen AH, Sengelov H, Borregaard N. 1993. Isolation and primary structure of NGAL, a novel protein associated with human neutrophil gelatinase. J Biol Chem 268:10425–10432. Kubben FJ, Sier CF, Hawinkels LJ, Tschesche H, van Duijn W, Zuidwijk K, van der Reijden JJ, Hanemaaijer R, Griffioen G, Lamers CB, Verspaget HW. 2007. Clinical evidence for a protective role of lipocalin-2 against MMP-9 autodegradation and the impact for gastric cancer. Eur J Cancer 43:1869–1876. Lee HJ, Lee EK, Lee KJ, Hong SW, Yoon Y, Kim JS. 2006. Ectopic expression of neutrophil gelatinase-associated lipocalin suppresses the invasion and liver metastasis of colon cancer cells. Int J Cancer 118:2490–2497. Li EM, Xu LY, Cai WJ, Xiong HQ, Shen ZY, Zeng Y. 2003. [Functions of neutrophil gelatinase-associated lipocalin in the esophageal carcinoma cell line SHEEC]. Sheng Wu Hua Xue Yu Sheng Wu Wu Li Xue Bao (Shanghai) 35:247–254. Lim R, Ahmed N, Borregaard N, Riley C, Wafai R, Thompson EW, Quinn MA, Rice GE. 2007. Neutrophil gelatinase-associated lipocalin (NGAL) an early-screening biomarker for ovarian cancer: NGAL is associated with epidermal growth factor-induced epithelio-mesenchymal transition. Int J Cancer 120:2426–2434. Masaki T, Sugiyama M, Matsuoka H, Abe N, Izumisato Y, Sakamoto A, Atomi Y. 2003. Matrix metalloproteinases may contribute compensationally to tumor invasion in T1 colorectal carcinomas. Anticancer Res 23:4169–4173. NGAL IN GC DIAGNOSIS AND PROGNOSIS Mishra J, Dent C, Tarabishi R, Mitsnefes MM, Ma Q, Kelly C, Ruff SM, Zahedi K, Shao M, Bean J, Mori K, Barasch J, Devarajan P. 2005. Neutrophil gelatinase-associated lipocalin (NGAL) as a biomarker for acute renal injury after cardiac surgery. Lancet 365:1231–1238. Moniaux N, Chakraborty S, Yalniz M, Gonzalez J, Shostrom VK, Standop J, Lele SM, Ouellette M, Pour PM, Sasson AR, Brand RE, Hollingsworth MA, Jain M, Batra SK. 2008. Early diagnosis of pancreatic cancer: neutrophil gelatinase-associated lipocalin as a marker of pancreatic intraepithelial neoplasia. Br J Cancer 98:1540–1547. Nielsen BS, Borregaard N, Bundgaard JR, Timshel S, Sehested M, Kjeldsen L. 1996. Induction of NGAL synthesis in epithelial cells of human colorectal neoplasia and inflammatory bowel diseases. Gut 38:414–420. Parkin DM, Bray FI, Devesa SS. 2001. Cancer burden in the year 2000. The global picture. Eur J Cancer 37 (Suppl 8):S4–S66. Pavlick AC, Gerdes H, Portlock CS. 1997. Endoscopic ultrasound in the evaluation of gastric small lymphocytic mucosa-associated lymphoid tumors. J Clin Oncol 15:1761–1766. Stoesz SP, Friedl A, Haag JD, Lindstrom MJ, Clark GM, Gould MN. 1998. Heterogeneous expression of the lipocalin NGAL in primary breast cancers. Int J Cancer 79:565–572. Takahashi Y, Kitadai Y, Ellis LM, Bucana CD, Fidler IJ, Mai M. 2002. Multiparametric in situ mRNA hybridization analysis of gastric biopsies predicts lymph node metastasis in patients with gastric carcinoma. Jpn J Cancer Res 93:1258–1265. 1863 Tan E, Gouvas N, Nicholls RJ, Ziprin P, Xynos E, Tekkis PP. 2009. Diagnostic precision of carcinoembryonic antigen in the detection of recurrence of colorectal cancer. Surg Oncol 18:15–24. Tong Z, Kunnumakkara AB, Wang H, Matsuo Y, Diagaradjane P, Harikumar KB, Ramachandran V, Sung B, Chakraborty A, Bresalier RS, Logsdon C, Aggarwal BB, Krishnan S, Guha S. 2008. Neutrophil gelatinase-associated lipocalin: a novel suppressor of invasion and angiogenesis in pancreatic cancer. Cancer Res 68:6100–6108. Wu X, Lu XH, Xu T, Qian JM, Zhao P, Guo XZ, Yang XO, Jiang WJ. 2006. Evaluation of the diagnostic value of serum tumor markers, and fecal k-ras and p53 gene mutations for pancreatic cancer. Chin J Dig Dis 7:170–174. Yan L, Borregaard N, Kjeldsen L, Moses MA. 2001. The high molecular weight urinary matrix metalloproteinase (MMP) activity is a complex of gelatinase B/MMP-9 and neutrophil gelatinase-associated lipocalin (NGAL). Modulation of MMP-9 activity by NGAL. J Biol Chem 276:37258–37265. Yang J, Goetz D, Li JY, Wang W, Mori K, Setlik D, Du T, Erdjument-Bromage H, Tempst P, Strong R, Barasch J. 2002. An iron delivery pathway mediated by a lipocalin. Mol Cell 10:1045– 1056. Zhang H, Xu L, Xiao D, Xie J, Zeng H, Wang Z, Zhang X, Niu Y, Shen Z, Shen J, Wu X, Li E. 2007. Upregulation of neutrophil gelatinase-associated lipocalin in oesophageal squamous cell carcinoma: significant correlation with cell differentiation and tumour invasion. J Clin Pathol 60:555–561.