Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
West Nile fever wikipedia , lookup
Sarcocystis wikipedia , lookup
Oesophagostomum wikipedia , lookup
Rocky Mountain spotted fever wikipedia , lookup
Onchocerciasis wikipedia , lookup
Hepatitis B wikipedia , lookup
Eradication of infectious diseases wikipedia , lookup
Schistosomiasis wikipedia , lookup
Marburg virus disease wikipedia , lookup
African trypanosomiasis wikipedia , lookup
Brucellosis wikipedia , lookup
Middle East respiratory syndrome wikipedia , lookup
Coccidioidomycosis wikipedia , lookup
Infectious mononucleosis wikipedia , lookup
Leptospirosis wikipedia , lookup
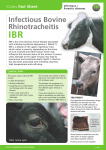
Infectious Bovine Rhinotracheitis (IBR) Phil Scott DVM&S, DipECBHM, CertCHP, DSHP, FRCVS Infectious bovine rhinotracheitis (IBR, BHV 1) Introduction IBR is a highly contagious and infectious viral disease that affects cattle of all ages. Infection occurs by inhalation and requires contact between animals spreading quickly through the group. The disease is characterised by severe inflammation of the upper respiratory tract. Bovine herpes virus 1 (BHV 1) also causes infectious pustular vulvovaginitis in the female, and infectious balanoposthitis in the male. Clinical signs Clinical signs generally first appear two to three weeks following transport, sale, housing or other stressful event such as calving. During an outbreak of IBR, the morbidity rate may be 100% but the mortality rate is generally less than 2%. The first two or three cattle affected often develop the most severe clinical signs. The conjunctivae are oedematous and there is partial prolapse of the third eyelid. Tear staining of the face, quickly turning purulent, can be pronounced. There may be small erosions on the nasal septum progressing to diphtheritic plaques. There are no oral lesions but there is drooling of saliva due to ruminal stasis. There is halitosis from pus in the larynx and trachea, and varying degrees of dyspnoea. Affected animals cough frequently and palpation of the larynx is resented. There is an increased respiratory rate but no abnormal lung sounds except sounds referred from the upper respiratory tract. After several days, inappetance leads to a shrunken rumen giving affected cattle a gaunt appearance. Body condition loss can be pronounced. Death is unusual but is caused by severe damage, necrosis and secondary bacterial infection of the trachea with accompanying inhalation pneumonia. Affected cattle lose their appetite, develop a high fever (41-42°C) with purulent ocular and nasal discharges. Severely affected animals are very depressed, slow to rise, and stand with the head held lowered. Purulent nasal discharge in a purchased steer with suspected IBR. Much milder clinical signs with conjunctivitis, occasional coughing and poor milk yield can occur. IBR virus enhances the pathogenicity of Moraxella bovis and severe infectious keratoconjunctivitis lesions can develop in calves. Differential diagnoses in individual cattle Suspected IBR in a recently purchased Charolais bull. The bull was febrile (41.5°C). The lungs were also scanned to check for chronic suppurative pneumonia. - Recrudescence of chronic suppurative pneumonia - Malignant catarrhal fever - Mucosal disease Copyright ©NADIS 2017 Recrudescence of chronic suppurative pneumonia in a dairy heifer two weeks after calving Foot and mouth disease Differential Diagnosis in a group of cattle - Bluetongue. - Foot and mouth disease Diagnosis Malignant catarrhal fever should be differentiated from IBR. Diagnosis can be established after careful inspection of all the animals in the group. Fluorescent antibody test (FAT) requires ocular swabs (rub vigorously as test needs cells) from affected febrile animals avoiding samples from cattle with purulent ocular discharges. If the veterinary laboratory is not local, make smears on glass slides and dry in air before posting. Note that false negatives are not uncommon. Copyright ©NADIS 2017 Necropsy findings of severe tracheitis in a beef steer that had died from IBR. MSD Animal Health At the start of an IBR control programme, measuring bulk milk antibody titres can be a very useful means of determining IBR status of the herd. However, a negative bulk milk result does not necessarily indicate that a herd is IBR-free as up to 20% of the milking herd can be latently infected with IBR before the bulk milk result will become positive, therefore blood testing is essential to confirm IBR-free status. Once the veterinary health plan is in place bulk milk antibody testing can be a simple means of confirming the absence or low prevalence of IBR. NADIS seeks to ensure that the information contained within this document is accurate at the time of printing. However, subject to the operation of law NADIS accepts no liability for loss, damage or injury howsoever caused or suffered directly or indirectly in relation to information and opinions contained in or omitted from this document. To see the full range of NADIS livestock health bulletins please visit www.nadis.org.uk Treatment Vaccinate all animals in the group immediately IBR is suspected on clinical findings. Sick animals should be treated daily for five to seven days with parenteral procaine penicillin. There is little benefit gained from administering much more expensive antibiotics. NSAIDs can be used as supportive therapy; never use corticosteroids. Management/Prevention/Control measures IBR vaccination is inexpensive, either by single intranasal or intramuscular injection and is incorporated into veterinary herd plans. Marker gE vaccines are available for more sophisticated control programmes. Purchased beef cattle of uncertain status should be vaccinated as soon as they arrive on farm, and are often turned out to pasture for three to six weeks in the autumn before housing. Purchased beef stores vaccinated against IBR and turned onto stubbles for several weeks before housing in November. Copyright ©NADIS 2017