Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Treatment of Parkinson's disease
Parkinsonism: - {paralysis agitans, shaking palsy}
•
•
•
•
•
•
•
•
•
Is a general term includes both the disease (Parkinson's disease) and the drug-induced state.
Definition:A progressive, neurological disorder of muscle movement (extra-pyramidal motor disorder)
including:Resting tremor (pill-rolling).
Cog wheel rigidity( increase stiffness & resistance).
Bradykinesia (slowness in initiating and carrying out voluntary movements).
Masked face.
Postural and gait abnormalities.
Incidence: - ≈ 1 in 100 individuals, usually over 65 years of age.
• Pathophysiology: Two balanced systems are important in the extra-pyramidal control of motor activity at the level
of corpus striatum and substantianigra.
substantianigra is the source of dopaminergic neurons that terminate in neostriatum, secreting
the inhibitory neurotransmitter dopamine (DA).
The neostriatum is connected to substantianigra by neurons secreting the inhibitory transmitter
GABA.
And containing neurons that secrete the excitatory transmitter Ach.
DA and Ach in basal ganglia control the motor activity of extra-pyramidal system.
DA present in medulla → nausea and vomiting by stimulation of CRTZ.
DA present in hypothalamus → inhibition of prolactin release.
DA present in certain paths → cerebral cortex.
In Parkinson's disease → progressive degeneration of DA neurons in substantianigra and
nigrostriatal tissue → imbalance between the inhibitory DA and the excitatory Ach. Cell
death → less DA release in neostriatum. As well as accumulation of proteins in Lewy bodies
in neurons
•
Classification:A-Idiopathic (mostly)
B-Secondary:1-Disease – induced: Viral encephalitis.
Atherosclerosis.
Wilson disease (rare).
2-Drug – induced:a-DA blockers: Phenothiazine.
Haloperidol.
Metoclopramide.
b-DA (depletory) → reserpine.
c-Drugs ↑ cholinergic activity → anticholinesterases.
d--MPTP → meperidine analog → DA neuron degeneration(frozen addict syndrome).
3-Exposure to some unrecognized neurotoxins and to occurrence of oxidation reaction
and generation of free – radicals(pesticides)
C-Genetic factorsyoung onsetPD
• Drugs used in Parkinson's disease
•
•
The available drugs offer temporary relief and don’t arrest or reverse the degeneration.
Try to restore dopaminergic / cholinergic balance by:1-Reduce cholinergic activity by:
Antimuscarinic → effective in Rx of tremor and rigidity (even if the later caused by DA
antagonists).
2-Enhance DA activity:By dopaminergic drugs which is effective in Rx of hypokinesia, rigidity, less effective in Rx
of tremor.
a- Replenish neuronal DA by
. E.gLevo – dopa.
b- DA – agonists as: Bromocriptine, Pergolidecabergoline, Apomorphine.
c- prolong DA action by selective inhibition of DA metabolism. E.g. selegiline, entacapone.
d- Release DA from stores and inhibit re-uptake. amantadine.
e- Vit. E and C, nicotine, aspirin, antidepressant.
G- Glutamate antagonist, norepinephrine precursor. Both approaches are effective and
may usefully be combined.
• Dopaminergic drugs:-.
•
•
1.
2.
•
•
•
Relief with L – dopa is symptomatic and lasts only while drug is present in the body.
DA can not be used because:Rapidly metabolized in gut, blood, liver by MAO and COMT enzymes.
DA is insufficiently lipid soluble → don’t cross BBB.
Levodopa and dopa – decarboxylase inhibitors:Replenish the DA neurons with dopamine.
Readily absorbed from upper small intestine by active transport and cross BBB → C.N.S. by
the same mechanism. It is a natural precursor of DA (prodrug).
Extensively metabolized by decarboxylase → DA in peripheral tissues and only ≈ 1 – 5%
of the oral dose → C.N.S., so large doses of L-dopa are required which lead to:-
1. Peripheral side effects as:Nausea and vomiting, arrhythmias, postural hypotension.
2. ↑ Dose of L-dopa → inhibit gastric emptying and erratic absorption.
• Addition of DOPA – decarboxylase inhibitors lead to:1. ↓ The metabolism of L-dopa in G.I.T. and peripherally, ↑ the availability of L-dopa to the CNS.
2. Lowers the dose of L-dopa to the 4th.
3. ↓ Severity of side effects of peripherally formed DA. (Mainly nausea and vomiting 80% → 15%
and less).
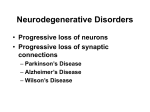
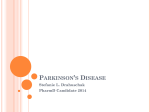
• Synthesis of dopamine from levodopa in the absence and presence of carbidopa,an inhibitor of
dopamine decarboxylase in the peripheral tissues.
•
• Formulations comprising a decarboxylase inhibit L-dopa:1. L-dopa + Carbidopa → Sinemet.
2. L-dopa + Benseazide → Madopar.
Actions: CNS.• Improves rigidity, hypokinesia first, later tremor.
• Secondary symptoms → posture, gait, handwriting, facial expression, mood, self care, speech,
interest in life are normalized.
• Behavioral excitement and even frank psychosis.
CVS:• Tachycardia, ↑ force of contraction → DA stimulates β-receptors.
• Postural hypotension → centrally mediated ↓ sympathetic outflow (tolerance could occur).
Endocrine: - control prolactin release (inhibition).
•
•
•
•
•
•
Absorption:Rapidly absorbed (active transport) → upper GIT.
T1/2 is 1 – 2 hours → fluctuation in plasma concentration → fluctuation in motor response on –
off phenomenon → relapse (with chronic use)
High protein diet (meals) → interferes with transport of L-dopa into CNS.
Large neutral a.a. compete with L-dopa for absorption and transport to CNS.
L-dopa should be taken on empty stomach,30- 45 minutes before a meal.
• Adverse effects (frequent, troublesome):• Peripheral effects:– Anorexia, nausea and vomiting (dose-dependent)
– → stimulation of emetic center (DA acts as excitatory transmitter in CTZ, D2 receptors in the
gut).
– Cyclizine, domoperidone used as antiemetic, 30 minutes before Rx with L-dopa.
– Nausea maybe a limiting factor if the dose ↑ rapidly, start with lowdose of L-dopa and ↑
gradually as tolerance developed.
–
• CVS:– Tachycardia, Ventricular extrasystole, arrhythmias, by stimulation of β-receptors.
– Exacerbate angina.
– Postural hypotension.
• Mydriasis → adrenergic action on iris. Glaucoma → ↑ I.O.P. (intra ocular pressure).
• Blood dyscrasies and +ve coombs reaction.
• Brownish discoloration of saliva and urine due to catecholamine oxidation which produce
melanin pigment.
•
–
–
–
–
•
•
•
•
CNS effects:Reflection over activity of DA at receptors in basal ganglia.
Visual, auditory hallucination.
Abnormal involuntary movement → dyskinesia.
Mental changes:Depression, Rx by T.C.A.
Anxiety, agitation, psychosis.
On – off effects → progression of dis. and improv. due to fluctuation of L-dopa plasma
concentration.
Avoid sudden discontinuation of L-dopa.
• Interactions:•
Vit B6 (pyridoxine), Dopa decarboxylase is B6 dependent enzyme → ↑ peripheral break
down.
• L-dopa and MAO inhibitors → hypertensive crises
Non selective MAO inhibitors protect DA from metabolism → accumulate → noradrenaline →
hypertensive crises.
But with selective MAO-B inhibitor e.g. selegiline → therapeutic value, T.C.A are safe.
• L-dopa exacerbates psychotic illness.
• Antihypertensive → enhances the hypotension.
• High protein diet and a.a.
• Antipsychotics are contraindicated in Parkinson's disease; they (Antipsychotics) block DA
receptors → exacerbation Parkinson's symptoms.
• Drugs that prolong DA action:1.
•
•
•
•
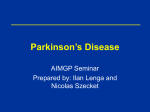
Selegiline:Selective irreversible inhibitor of MAO-B(which metabolizes DA).
Doesn't inhibit MAO-A (which metabolizes norepinephrine and serotonin).
Therefore ↓ metabolism of DA, ↑ DA level in brain.
It enhances and prolongs the action of L-dopa, and reduces the required dose of L-dopa.
Dopamine -------→
•
•
MAO-B ---------→
↑_
metabolites
Selegiline
May reduce mild on – off or end of dose fluctuation to L-dopa.
At recommended doses, selegiline has little potential for causing hypertensive crises (cheese
reaction), {MAO-A is available to metabolize norepinephrine, serotonin and even tyramine}.
•
•
•
•
•
•
At high doses, the selectivity is lost → risk of severe hypertension.
Early use of selegiline will retard severe symptoms set by 50% may be by reducing free
radicals formation(antioxidative therapy).
Used in mild cases, may combined L-dopa (has a minor therapeutic effect alone).
Cause insomnia→ give it during the day.
Interacts with pethidine → respiratory depression.
Contraindicated in patients taking meperidene, TCA, SRI → toxic interaction.
•
•
•
•
2-Rasagiline:Irreversible and selective inhibitor of brain MAO type B
More potent that selegiline in preventing MPTP – induced Parkinson's disease.
Under study as neuroprotective agent.
Not cause insomnia
Catecholamine – o – methyl transferase inhibitor
3-Entacapone
• Reversibly Inhibits COMT enzyme that metabolizes Levodopa.
• Prolongs L-dopa action.
• Effective in patients with early end – of –dose deteriorationand allows them to take L-dopa at 3
– 4h .
S.E.:• ↑Dyskinesia usually seen in late stages, sleep disorder.
4-Tolcapone:• reversibleCOMT inhibitor (central &peripheral) effect.
• Longer duration of action .why?
• Hepatic function monitoring is needed.Most seriously, fulminating hepatic necrosis is
associated with tolcapone use.
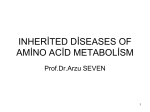
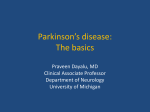
• Entacapone does not exhibit this toxicity and has largely replaced tolcapone.
• Effect of entacapone on dopa concentration in the central nervous system COMT =catechol-Omethyltransferase.
• Both drugs extensively bound to plasma protein 98%
• Dopamine receptor agonists:•
•
•
•
•
•
•
•
•
Ergot derivative.
Bromocriptine (parlodel):D2 receptor agonist with vasoconstrictor activity.
Commonly used with L-dopa in patients responding to L dopa Rx and in Parkinson's disease
complicated by motor fluctuation &dyskinasia.
Rapidly absorbed, T1/2 ≈ 5 hours, its action is similar to L-dopa but smoother than it which can
be an advantage in patients with end – of – dose deterioration with L-dopa.
Dosing ↑ gradually during a period of 2 – 3 months (weekly intervals) according to clinical
response.
The S.E. are severely limit the utility of DA agonist.
Nausea and vomiting are the commonest which respond to domperidone, tolerance can occur.
Postural hypotension → dizziness and syncope.
↑ doses → confusion, delusions, hallucination → worsen → mental condition in psychotic
patient.
.Serious cardiac problems may develop particularly in patients with M.I. Prolong use→ pleural
effusion and retroperitoneal fibrosis.
Contraindication → peripheral vascular disease,.,I HD,
psychosis
Uses of bromocriptine:1. Parkinson's disease, acromegaly.
2. Premenstrual tension syndrome.
3. Hyper prolactinemia.
4.Neuroleptic malignant hyperthermia
•
•
•
Lysuride → like bromocriptine action.
Pergolide → D1, D2 agonist, T1/2 ≈ 6 hours.
Cabergoline → T1/2 ≈ 80 hours.
•
•
•
•
Non – ergot drugs (newer) e.g. pramipexole,ropinirole androtigotine.
Effective in patients who have never been treated with L-dopa
In early Parkinson's disease they delay the need for L-dopa
-patients with advanced Parkinson's disease taking L-dopa ,they may ↓ L-dopa dose. Do not
exacerbate peripheral vasospasm.
Not cause fibrosis
S/E nausea, hallucination, insomnia or orthostatic hypotension.
Dyskinesia is less prominent than L-dopa.
Prevent prolactin release from anterior pituitary gland.
Rotigotine is available as transdermal delivery system
Cimetidine inhibits renal tubular secretion of organic bases ,so increase the half life of
pramipexole by 40%
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
-Apomorphine:Morphine divertive, similar structure to DA.
Full agonist at D1 and D2 receptors.
Given by injection (S.C.).
Useful in Parkinson's disease to treat:
difficulty in emptying the urinary bladder,
in young patients with severe motor fluctuation on- off phenomenon and dyskinesia, and
in refractory (resistant) cases.
Need to be accompanied by antiemetic which do not cross BBB (domperidone).
Over dose → respiratory depression which antagonized by naloxone.
The rapid onset of action after S.C. dose, enable the on – off – component of the on – off
phenomenon with L-dopa to be aborted without the patient waiting 45 – 60 minutes to absorb
another oral dose of L-dopa.
•
Drugs that release DA from stores and inhibit its re-uptake:-
•
1-Amantadine:Antiviral drug, effective against influenza A viral infection.
Mechanism of action:1. ↑synthesis, release of DA from surviving neurons and ↓ neuronal re-uptake.
2. Blockading cholinergic receptors.
3. Inhibit N – methyl – D – aspartate (NMDA) type of glutamate receptors which is the primary
action of amantadine in therapeutic concentration.
• If dopamine release is already at a maximum,amantadine has no effect
•
•
•
•
Over stimulation of NMDA receptors → excitotoxic effect on neurons → degeneration process
→ Parkinson's disease and Alzheimer disease
Amantadine is less effective than L-dopa, if combined together → slight enhancement of Ldopa action.
More effective than antimuscarinic
If combined with antimuscarinic → additive actionand less effect on tremor
•
•
•
Advantage: - once daily used and ↑ to 2,3 times / day.
Relative freedom from S.E. of L-dopa.
S.E.:CNS → restlessness, agitation, confusion, hallucination, insomnia, rarely fits.
Ankle odema (local effect on blood vessels)
Postural hypotension, urinary retention, dry mouth.
2-Memantine:Amantadine derivative.
Inhibit NMDA receptor.
Used for Rx of Alzheimer disease.
•
•
•
•
•
•
•
•
Antimuscarinic drugs:Used in simple cases with mild symptoms.
Modest improvement in tremor, rigidity, sialorrhoea, muscle stiffness and leg cramps.
Little improvement in hypokinesia.
Given orally, I.M., I.V. in acute drug induced dyskinesia.
Mechanism of action:Block Ach receptors in CNS, ↓ the imbalance created by ↓ DA activity.
Types:-Benzhexol, Benztopine, Biperiden, Procyclidine, orphenadrine.
S.E.:Mood changes → hallucination, memory defect, psychosis ….
Xerostomia, blurred vision, urine retention, constipation.
C.I.Glaucoma, pyloric stenosis, prostate hypertrophy, psychosis.
•
•
•
•
•
•
•
•
Fluctuation in response:Fluctuation in response to L-dopa occurs with increasing frequency as Rx continues.
Occurs after 3 – 5 years of Rx.
In some patients, these fluctuations related to the timing of L-dopa intake called end – of dose
deterioration or wearing – off reactions.
• In others, fluctuations in clinical state are unrelated to the timing of dose (on – off –
phenomenon).
• And usually occurs in patients who respond well to Rx initially, (no exact mechanism).
• And in new patients, the therapeutic response to L-dopa is consisted, but with time, the
number of neurons ↓ and fewer cells are capable of taking up exogenously administered Ldopa and converting it to DA, → motor control fluctuation develops.
Rx:• More frequent and smaller doses (once hourly).
• Using dopamine agonist with L-dopa e.g. bromocriptine.
• Use selegiline or entacapone with L-dopa.
• Apomorphine.
• Sustained released L-dopa preparation like sinemet and madopar to Rx end – of dose
deterioration.
DRUGS USED IN ALZHEIMER’S DISEASE
Dementia of the Alzheimer type has three distinguishing features:
1)accumulation of senile plaques (β-amyloid accumulations),
2) formation of numerous neurofibrillary tangles, and
3) loss of cortical neurons,particularly cholinergic neurons.
•
•
•
Current therapies aim to either:improve cholinergic transmission within the CNS or
prevent excitotoxic actions resulting from over stimulation of NMDA-glutamate receptors in
selected areas of the brain
•
•
A. Acetylcholinesterase inhibitors
inhibition of acetylcholinesterase (AChE) within the CNS will improve cholinergic transmission,
at least at still functioning neurons
. The reversible AChE inhibitors approved for the treatment of mild to moderate Alzheimer’s
disease include
donepezil ,Galantamine( may also augment the action of acetylcholine at nicotinic receptors
in the CNS) and rivastigmine
Rivastigmine is the only agent approved for the management of dementia associated with
Parkinson’s disease and also the only AChE inhibitor available as a transdermal formulation.
Common adverse effects include nausea, diarrhea, vomiting anorexia, tremors, bradycardia,
and muscle cramps
•
•
•
•
•
•
•
•
•
•
•
•
•
•
B. NMDA receptor antagonist
Stimulation of glutamate receptors in the CNS appears to be critical for the formation of certain
memories.
However, over stimulation of glutamate receptors, particularly of the NMDA type, may result
inexcitotoxiceffects on neurons and is suggested as a mechanism for
neurodegenerative or apoptotic (programmed cell death) processes.
Binding of glutamate to the NMDA receptor assists in the opening of an ion channel that allows
Ca2+ to enter the neuron. Excess intracellular Ca2+ can activate a number of processes that
ultimately damage neurons and lead to apoptosis.
Memantine
indicated for moderate to severe Alzheimer’s disease.
It acts by blocking the NMDA receptor and limiting Ca2+ influx into the neuron, such that
toxic intracellular levels are not achieved
Memantine is well tolerated with few dose-dependent adverse events.
Expected side effects, such as confusion, agitation, and restlessness, are indistinguishable
from the symptoms of Alzheimer’s disease has possible neuroprotective effects,memantin is
often given in combination with an AChE inhibitor
•