Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Catalytic triad wikipedia , lookup
Genetic code wikipedia , lookup
Metalloprotein wikipedia , lookup
Fatty acid metabolism wikipedia , lookup
Point mutation wikipedia , lookup
Peptide synthesis wikipedia , lookup
Citric acid cycle wikipedia , lookup
Amino acid synthesis wikipedia , lookup
Fatty acid synthesis wikipedia , lookup
Biochemistry wikipedia , lookup
Nucleic acid analogue wikipedia , lookup
15-Hydroxyeicosatetraenoic acid wikipedia , lookup
Butyric acid wikipedia , lookup
Specialized pro-resolving mediators wikipedia , lookup
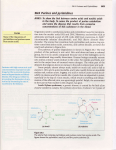
URIC ACID METABOLISM AND MEDICATIONS I’m here to talk about uric acid and so it’s in the context of gout and what we are going to be considering is what is uric acid? How does it lead to gouty arthritis and, for that matter, how does uric acid also lead to kidney stones otherwise known as renal calculi? Where does uric acid come from? And we’ll see, actually, that it’s the tail end of biochemical pathway linked to purines; purine nucleotides, nucleocides and even just the straight purine bases. So it’s right at the tail end of breakdown of DNA / RNA, for example. And we’ll see that can be clinically very important, particularly in a situation where you have a patient with a malignancy that is treated with an anti-cancer drug and the malignancy, the malignant cells, respond in a dramatic way. If you think just for a moment about all the DNA and all those dividing cells, what happens when those cells die? Suddenly you’ve got a big load of biochemical substrate and we’ll see that, at least we’ll consider, the consequences of all of the DNA and RNA in those cells breaking down to purines and the load that that then creates in terms of uric acid production. We’ll also consider a couple of pathways for purine nucleocide synthesis. One is how do you make a purine nucleocide from scratch and what’s its relevance to uric acid production? And we’ll also consider a so-called salvage pathway mechanism which is a rather neat way of retrieving some purine bases before they get converted to uric acid and, in that way of course, you potentially can reduce the amount of uric acid production but, of course, there are also some economies involved in this in terms of retrieving those purine bases and returning them back into the nucleotide… nucleocide, nucleotide pool, remembering that a nucleocide is essentially a purine or a pyrimadine attached to a ribose, to sugar; a nucleotide is a purine or pyrimadine base attached to a sugar attached to phosphates and, of course, its in that phosphorylated form, that phosphated acid form, that DNA and RNA can be made. 1 URIC ACID METABOLISM AND MEDICATIONS All right: so let’s get going. I’m not going to say a lot about the aetiology of gout, partly because I’m not a pathologist, partly because I’m not a rheumatologist and partly because not all that much is known about it either, but the basic point seems to be that the crystallisation of uric acid in the joints acts as the trigger for an acute inflammatory reaction and that acute inflammation involves the recruitment of neutrophils and the attempt by the neutrophils to engulf uric acid crystal. If you like, it treats the uric acid crystal as it would a bacteria. It tries to phagocytose and it tries to kill it. The only problem is it’s not a living organism. It’s a crystal and one of the consequences of that is that the neutrophils are not particularly effective because the crystals actually survive the action of the neutrophils, so that means more neutrophils tend to get recruited and, as a consequence of that, you get this vicious cycle whilst you get the release locally of the enzymes and the oxygen metabolites that the neutrophil is trying to use to kill the crystals and, as a consequence of that, you get local joint damage. I think I have said all those things there. Notice that I’ve also used the term sodium urate and they can, to some extent, be used interchangeably. Uric acid; urate. What’s uric acid? How are its levels for influence? And we’ll see some of the main influences on that as this lecture unfolds. Here we have the structures of uric acid in at least one of its forms on the left and urate on the right so you can see that, essentially, there’s an equilibrium between uric acid form and the urate form. It’s a ph-dependent equilibrium, as 2 URIC ACID METABOLISM AND MEDICATIONS you would expect for an acid. The ph at which you have equal concentrations of the acid form and the anion form is, as you can see there, around 5.8, so it’s actually below the normal serum ph. So that means that, under normal conditions with, essentially, anions accumulating at pHs above 5.8 and acids accumulating, at least the proteinated forms, accumulating at pHs below that pKa value 5.8, but normal neutral ph around 7.4. The predominant form is urate, right? It’s predominantly up to that right hand side. Many of you who are familiar with this ph equilibrium will see that immediately. So, under normal circumstances then, in a joint, its sodium urate, its crystals of sodium urate, typically monosodium urate since sodium is the primary cationic species of blood plasma that crystallises and causes the problem. Of course, if the ph equilibrium is disturbed in the joint, then things can change. In the kidney where you get calculi formed from uric acid/urate crystals, then there probably is, in fact, more uric acid because the ph in the renal tubules, as many of you will be aware, progressively acidifies as you head down from the glomerulus where the blood is first filtered down to the collecting tubules where it will ultimately enter the pelvis of the kidney to transfer to the bladder. So we have to deal with these two different terms – uric acid and urate. I think you can see, for all intents and purposes, the names are interchangeable when we’re talking about this among colleagues and, indeed, among patients that there are some specific theoretical points that relate to what is the major species in a certain location under certain conditions? I think I’ve said this already. Uric acid is a purine base. So if we have nucleocides being either purines or pyrimadines, then we’re talking about the purine half of the nucleotide metabolism here. And here are three of the main purines, adenine and guanine, we’ve talked a lot about in different contexts. 3 URIC ACID METABOLISM AND MEDICATIONS They are, of course, the “A’s” and “G’s” in DNA and RNA. Hypoxanthine is a close relative. I think you can see in structural terms and it’s an important member in the pathway. This slide seeks to make the global point that it doesn’t matter whether we’re talking nucleotides with the sugars and phosphates, or nucleocides just with the sugars, or just the purine bases themselves. Just those two rings fused together, the six-membered ring, the five-membered ring with the nitrogens. When we come to consider the breakdown of these species, there is a final common pathway. Its essentially nucleotide, remove the phosphates, nucleocide – now remove nucleocides, now remove the sugars, purine bases on to uric acid. Serum uric acid or, I should say urate concentrations in men and women, are roughly the same. As you can see, they tend to be slightly higher in males than in females. The curious thing about this is that the solubility of urate in solution is extremely close to its actual concentration in plasma, so much so that its probably true that there are not particularly well-defined substances in the plasma which act to limit the crystallisation of the uric acid so you can imagine a situation where a biochemical inhibitor of crystallization, if its levels can be adjusted either up or down, can have a potential impact on whether or not crystals form. Why are uric acid levels so high in humans? It’s curious. Humans, amongst primates and other mammals, are unusual in not converting uric acid to another much more water soluble product known as allantoin – a-l-l-a-n-t-o-i-n, allantoin. Now just imagine that six-membered ring of the purines opening up from uric acid or from the purine and essentially you’ve got the idea; there is an enzyme in all those other species which converts uric acid or urate, converts it 4 URIC ACID METABOLISM AND MEDICATIONS to allantoin. Allantoin is much more water-soluble and readily excreted, doesn’t tend to crystallize, and doesn’t tend to cause gout or cause kidney stones – renal calculi. So what are the concentrations so high in humans? There’s one line of argument - there are a couple of different lines of argument – the one there about promoting salt retention under low salt conditions, I’m not sure just how robust that idea is. The one above that relating to a possible role of uric acid as an anti-oxidant I think does need to be taken seriously because it can be shown in vitro in the test tube that, in fact, it does have anti-oxidant effects and those anti-oxidant effects are quite impressive. It seems to be in many cases more powerful as an anti-oxidant than Vitamin C, even in school days. So there is a serious view, and this needs to be taken seriously, that uric acid has a role as a biological anti-oxidant in humans and that this may actually have some protective effect. It makes it very difficult when you look at a patient who may have a number of metabolic problems, including an increase in uric acid concentration, to try to dissect out what is cause and effect but one view is that the uric acid is actually … its levels are increasing as a response to a pro-inflammatory situation with a view to suppressing the damage that arises from oxidation. Here is some data of the type we are just talking about. So we’re looking at the percent remaining of different species. So here we have uric acid as you can see in the presence of… In this case it’s a radical oxygen known as singlet oxygen. It’s rather an unusual form of oxygen in which the unpaired electrons end up in an excited state and it turns out to be quite a reactive form of oxygen, or superoxide or hydroxyl radicals and so on. 5 URIC ACID METABOLISM AND MEDICATIONS You can see that in the presence of, in this case, singlet oxygen that uric acid rapidly gets degraded. This is a sign that it’s actually interacting with and detoxifying, if you like, the singlet oxygen. Ascorbate also works, all right, in his assay. Interestingly, so does deoxyguanine, but none of the other purines or pyrimadines that were tried here actually had any effect or were able to interact with these radicals. This table is from a different study basically showing the same kind of thing. You can see here… What’s happening here essentially is that either ascorbate or uric acid is acting to interact or inhibit the formation of radical cations so, in fact, that’s what we’re seeing here is that inhibitory effect. Now you can see that, at a concentration of around a plasma-like concentration of uric acid, there’s actually quite a powerful effect here. The concentration of ascorbate on supplements is around about 100 to 200 mmol/L. You can see that, in fact, the effect of uric acid is much greater in this assay system than the effect of ascorbate than concentrations that would be achieved under normal circumstances in plasma. There’s also a refinement here: human serum albumen also interacts with the system and does have an effect as well. So, those of you who would like to pursue this and there are some more recent papers asking the question whether, under some circumstances, uric acid may be anti-oxidant in its effects and, in other circumstances, may be pro-oxidant in its effects. For those of you who would like to pursue these issues, here are some of the papers that are relevant to the anti-oxidant case and I would be very happy to send you any references related to possible pro-oxidant effects as well, if you’re interested. 6 URIC ACID METABOLISM AND MEDICATIONS How do we eliminate uric acid? Essentially via the kidneys and so there’s filtration across the glomeruli, it’s a small molecule, certainly small enough to cross the filtration barrier of the glomeruli. It then gets secreted and reabsorbed. Now the reabsorption, as you can see, is not entirely designed to eliminate uric acid and has the effect of putting a brake on elimination. And so you can boost the elimination of uric acid by blocking that reabsorption mechanism and we’ll look at a couple of drugs a little later that actually do that. Does diet have an effect on serum uric acid levels? The answer to that does seem to be yes, and so although uric acid sits at the bottom end of the metabolic pathway that is essentially breaking down purines and so therefore the rate of endogenous breakdown of purines is, perhaps, the primary determinant of what uric acid levels will, ultimately, be. It is a partially open-ended system and we are consuming foods that are rich or not rich in purines and they can have an effect so foods that are high in purines include seafoods, meat, alcoholic beverages, especially beer. Foods that are low in purines are fruits, grains, vegetables and a few other things that are listed there. So, the ultimate level of uric acid in serum is dependent then on quite a number of different factors: Purine nucleotide synthesis, simply because if you don’t have purines you can’t break them down and make uric acid, so how fast are purine nucleocides being made? That will have an impact, ultimately, on how much uric acid is ultimately produced. What is the rate of puric breakdown? What is the rate of puric intake and how fast is the uric acid being excreted by the kidneys? Now, we are going to have a look at the mechanism of purine nucleotide synthesis – the so-called salvage pathways that I mentioned right at the very beginning of the lecture and how they interact with one another to determine uric acid production rates. Don’t be scared by these pathways. 7 URIC ACID METABOLISM AND MEDICATIONS Down here we’ve got urate. Here are the nucleotides’, nucleocides’ purine bases. We have just been talking about that. This little branch here is essentially talking about the production of purine nucleotides starting with a sugar phosphate, ribose phosphate. Remember that we, in the last lecture, considered the mechanism of synthesis of ribose, ribose 5-phosphate via the pentose phosphate pathway so we have glycolysis, glucose entering the cell, its converted to glucose 6-phosphate, is trapped, and then potentially can be shunted out through the pentose phosphate pathway to make ribose, right? Okay. So here’s ribose. Here’s the ribose 5-phosphate. This intermediate gets generated. We’ll have a look at its structure in just a minute. It sounds terrible – it’s not so terrible - and then amino acids are also required but, essentially, it can then make the nucleotides. They can then be used to make nucleic acids or they can be a source of energy for biochemical pathways. Notice that the diet largely provides nucleocides or purine bases. Here are the so-called salvage pathways. So free purine bases can either be converted to urates, in which case they need to be excreted, or via the salvage pathways they can be converted back to nucleotides, in which case they can return to the pore, they can be used in the synthesis of DNA and RNA and so on. So, in terms of the fluxes, then, through this overall mechanism, we have got a dietary input, we’ve got an input from the synthesis of purine nucleotides and then we’ve got this salvage pathway mechanism. So let’s just have a slightly closer look at these different inputs. I think that just having looked at… seen that diagram, I think you’ll probably agree with me that the de novo pathway promotes uric acid production. It’s seen to be providing substrates. The salvage pathways inhibit uric acid production. 8 URIC ACID METABOLISM AND MEDICATIONS We’re at the top end of the de novo purine nucleotide synthesis pathway here. With ribose phosphate being converted to this metabolite, phosphoribosyl pyrophosphate. Now here’s ribosyl phosphate over here, here’s our sugar, here’s our phosphate and here’s the dotted line, and the dotted line ultimately, as the purine nucleotide gets synthesized, will take on the familiar shape, the double ring shape. But it has to be built up in sequences, in specific biochemical reactions, and it starts with two phosphates joined together sitting here “just like an activated intermediate” would be the way a biochemist would refer to this. And so you can see then that ribosyl phosphate gets converted to PRPP, so we have our two phosphates attached at this point and then pyrophosphate is often also used as a source of energy and it’s useful in this context as well for a source of energy for driving the reaction forward. The next thing that happens essentially is that the pyrophosphate, those two phosphates, are knocked off and replaced by an amino group. And then it gets built up, first of all to IMP which is a hypoxanthine-base attached to ribose attached to a phosphate. And then, from there, down to ATP and GTP and off you go with DNA and RNA synthesis and so on. There’s another point that the slide seeks to make, and that is that not only is PRPP, so this nucleus with these two additional phosphates added to it are substrate, it also has an influence on the pathway and so his red arrow here with the plus sign beside it is intended to get across the point that the level of phosphoribosyl pyrophosphate (PRPP) also has an impact on the rate at which the pathway proceeds. If you like it can activate the enzyme, not just be a substrate for the enzyme, it can actually switch the enzyme on. That suggests there is a second site on the enzyme, one that’s involved in the catalytic pathway, another one which is actually influencing the rate at which the enzyme works. 9 URIC ACID METABOLISM AND MEDICATIONS Now, when we consider the salvage pathways and what happens when you block those, we’ll see that in fact PRPP can accumulate in a way that is not to the advantage of the system because it can, inappropriately, drive… purine nucleotide synthesis can switch it on really powerfully. So it’s worthwhile just noting that – the text there and the plus sign in red. What about salvage pathways? Basically controlled by two enzymes and here is the basic point I think I’ve now tried to make a couple of times is to take a purine base, right? Ribose is not there, the phosphates are not there and convert it back to a nucleotide with the ribose with the phosphate. And so that’s what we’re seeing here in the case of adenine and what we’re seeing in the case of guanine and hypoxanthine. Notice that PRPP, that we’ve just met, also participates in these salvage pathways. If they work, they’re a neat way of returning the purine bases back to the nucleotide pool for biochemical uses. If they don’t work, then the adenine, the guanine, the hypoxanthine are going to be broken down and converted to uric acid. So the existence of the salvage pathways then provides a brake potentially on uric acid production. So, the roles of salvage pathway enzymes to minimise uric acid production recover purine bases for use as purine nucleotides. It’s interesting. In certain tissues the levels of the salvage enzymes are extremely high - much higher than in other tissues. They brain is one site where they are particularly high. The levels are something like 10 to 20 times higher so that’s a sign that in the brain the pathways are orientated in such a way as to be extremely efficient in the purine nucleotide economy. Purine nucleotides are required as a source of energy. They are also required in certain biosynthetic pathways. You can see here; I’ve made the point that GTP is required for the synthesis of tetrahydrobiopterin. We’ve actually metabolic tetrahydrobiopterin before. Can anybody remember where? 10 URIC ACID METABOLISM AND MEDICATIONS Is anybody going to help me? I’ve just had a mental blank. Well, if I had just had a mental blank, nobody’s helping me! I remember as a first year intern I am assisting at an operation and I’ve got the Registrar beside me, I’ve got the surgeon on the other side; I’m holding my (inaudible ) – I think it’s a (inaudible ) – which is supposed to be holding the liver back and I feel as though I’m doing a really good job and, after a little while of this, the Registrar turns to me and says: “Help him! Help him! He needs help!”. Then I was taking much more interest in the operation, trying to put instruments in the right spot and not get in the way and so on. I guess you guys are not ready to be interns, right? (wry laugh) Tetrahydrobiopterin – we met it when we considered the pathway to convert phenylalanine to tyrosine in (inaudible 0:34:45.9). It’s a co-enzyme for that pathway. It turns out that BH4 is also a co-enzyme for the next step in the pathway which converts tyrosine to dopa which is just in front of the synthesis of the important neurotransmitter, dopamine. So, GTP is required for the synthesis of tetrahydrobiopterin and thus dopamine, a neurotransmitter in the brain. So that’s one reason why the brain actually goes to the trouble of making substantial amount of these salvage enzymes to hold on to these purine nucleotides. What we’re considering here is an X-linked condition, so it’s mainly boys, in which there’s a deficiency of the hypoxanthine/guanine phosphoribosyl transferase enzyme – one of these salvage enzymes we’ve just met. It’s a condition known as the Lesch Nyhan Syndrome. Here’s the reaction that should be catalysed so hypoxanthine or guanine in the presence of PRPP is converted either, in the case of hypoxanthine, to IMP or guanine and in the case of guanine to GMP. If there’s a block in this enzyme, if the enzyme doesn’t work or its seriously deficient as in Lesch Nyhan Syndrome, then you don’t make IMP or GMP; the salvage 11 URIC ACID METABOLISM AND MEDICATIONS pathway doesn’t work and, instead, hypoxanthine and guanine are converted to xanthine and, in turn, uric acid. So, you would expect that in these people they would have gout, which is to say high levels of uric acid in the blood, and if this pathway is really important for the metabolism, for the synthesis of neurotransmitters in the brain, there may be a problem in CNS function. Now, in fact, that turns out to be true. They do get serious CNS effects and here are some of the individuals affected; they’re mainly boys there. Mental retardation, self-mutilation, growth retardation, choreoathetosis, jerky movements of the body along with sinuous snake-like movements so the “choreo” is the jerking fast kind of movement; “athetosis” is the snake-like movement, so combinations of those – spacicity – and the effects do indeed arise from disturbed neurotransmitter synthesis in the brain. So, unfortunately, in neurons they don’t have a really robust mechanism for making purine nucleotides by the de novo pathway so the salvage pathway becomes important. And different cell types then have different levels of de novo purine synthesis enzymes. The liver has particularly high levels of those enzymes. Other cells, including neurons in the brain, have particularly high levels of salvage pathway enzymes. Since a lot of metabolic processing occurs through the liver, the fact that the salvage enzyme pathways are relatively low in the liver means that if there is a substantial drive to purine nucleotide synthesis, then there can be also a substantial drive to uric acid production. Let me just go back for a moment. Notice that, if we block this pathway, in addition to hypoxanthine/guanine now being substrate uric acid production, there’s also an increase in PRPP. So that, in certain tissues, where the purine nucleotide synthesis, the de novo synthesis pathway is available, you’ll get 12 URIC ACID METABOLISM AND MEDICATIONS enhanced drive for that pathway and, again, potentially enhanced drive of uric acid production. I think most of you are aware that, at least it’s a conversational point, that there’s an interaction between ethanol. Traditionally, it was the idea of champagne, I think, or port or sherry, and uric acid production but there does appear to be a real link between ethanol and uric acid production and we’ll just have a look at one way in which that works in just a moment. Just before we do that, just to remind you that in the pathway of ethanol oxidation, acetic acid or acetate, because the proton comes off here, is the primary product of the breakdown pathway and that’s irrespective of whether it goes via ADH, alcohol dehydrogenase, or via the cytochrome P450 system; you end up with acetate. Now when we last talked about this, we made the point that acetate can be converted to Acetyl CoA and that has some implications in terms of the caloric value of ethanol. Here’s the actual mechanism by which this occurs. Here we have ethanol being converted to acetate again, acetate being converted to Acetyl CoA. Notice that that enzyme requires ATP and that, in the process of Acetyl CoA production, AMP gets generated. RO phosphate comes off so the two terminal phosphates of ATP come off – it’s a source of energy for the reaction but AMP then gets generated. Now that AMP can be, as you can see, a source of purines in the production of uric acid so in acute experiments where this has been looked at carefully, you need to take the serum ethanol concentration up to around about 20 mV/L and you may recall that we made the point that at 0.05g percent, so the cut-off for 13 URIC ACID METABOLISM AND MEDICATIONS what the police would consider the cut-off for safe drinking and driving, the concentration is 10 mM - .05%, so we’re double that here and above so, around about .1% and above, at those levels you actually can see an impact on serum uric acid levels and they can go up by as much as 10%, 20% even 30% and since the uric acid concentration, even under normal circumstances, sits right on that knife-edge between crystallization and not crystallizing. The 10% or 20% increase, although it doesn’t sound like much, can be enough to predispose the individual to hyperuricemia and gout. So the clinical effects then of hyperuricemia: gouty arthritis, as you know or as we have been talking about, tophi - basically subcutaneous deposits of uric acid. Imagine a big lump on the top of my ear stuffed full of monosodium urate crystals – that’s a tophis, you know? That’s one of the common sites around joints. There’s another common site – renal calculi, kidney stones. So, clinical context in which it’s desirable to lower uric acid levels? If you would like to prevent acute attacks, you’ve got somebody who is having recurrent, acute attacks of gouty arthritis, one satisfactory approach is to lower the serum uric acid level. You might want to eliminate tophi. That can be painful. They’re certainly disfiguring and the cosmetic effect, as you can imagine, can be quite unpleasant. Suppress uric acid levels in the context of Tumor Lysis Syndrome. I mentioned this right back at the start. If you have a patient with a malignancy that happens to be a malignancy that is particularly sensitive to chemotherapy, as you know many leukaemias and lymphomas fall into that bracket. People go into hospital, have the regime of chemotherapy, the tumour melts away. As it does so, uric acid gets generated in large quantities along with a number of other biochemical by-products. 14 URIC ACID METABOLISM AND MEDICATIONS Since you’re producing such a large load of uric acid in this Tumor Lysis Syndrome, the chances of attacks of acute gout, of uric acid crystallizing in subcutaneous sites and, indeed, renal calculi are expected to become a serious problem and so its now very standard in anti-cancer regimens in this scenario to actually not only manage but to seek to prevent the consequences of the Tumor Lysis Syndrome in terms of marked increases in serum uric acid level and it would be very appropriate, and it is very appropriate, to monitor the uric acid level on a daily basis in these patients to make sure that you are actually controlling the situation, that the uric acid level does remain at around .4mM/L and doesn’t go up to .5, .6 and so on. Here are some examples of gouty tophi around the joints of the hands. That one has clearly been around for a while. Okay. Approaches to treating acute gout generally relate to trying to suppress the acute inflammation and so non-steroidal anti-inflammatory drugs, colchicines, which inhibits phagocytosis, and so therefore inhibits the neutrophil response, Cox-2 inhibitors, so the primary target in the case of acute gouty arthritis is, in fact, to control the inflammation, not to control the uric acid levels and, in a strange way that is not well understood, if you try to control acute gout or somebody who is having quite frequent attacks of acute gout, the agents that lower the serum uric acid level will often make the attack worse, prolong it and even trigger it so, in the acute attack, controlling the inflammation is essentially what you’re trying to do. Subsequently, once the acute attack is over, then it’s appropriate to seek to reduce the serum uric acid level with a view to preventing subsequent attacks and that strategy seems to work quite well. 15 URIC ACID METABOLISM AND MEDICATIONS So prevent attacks or treat tophi might be two of the aims of the management of gout. In terms of how do you go about lowering the serum uric acid levels, one is essentially the idea is trying to block uric acid synthesis and we’ll have a look at the drug that many of you are probably familiar with already, Allopurinol, how it does that, in just a moment, or stimulate its conversion to allantoin which is a relatively new approach, or promote urinary excretion of uric acid. Now, I think you can see that there is one potential problem of promoting urinary excretion of uric acid and that is that you can potentially induce the production of calculi. You can actually make your patient develop kidney stones and so, as a consequence of that, most of the strategies of lowering uric acid do not involve promoting urinary excretion. Nevertheless there is a drug, Probenecid, and we’ll look at it in just a moment, that is occasionally used for this purpose. Here’s the tail end of the pathway now. So the nucleotides have gone. The nucleocides have gone. We are down into the base territory. Here’s hypoxanthine, here’s xanthine, here’s uric acid. The red star there, or asterisk, basically is the site of action of the enzyme xanthine oxidase, and that’s the enzyme that the drug Allipurinol targets. Okay, we’ll spell Allipurinol in a moment. I think you’ve got it in your notes. Notice it doesn’t really matter whether the purines are coming from the adenine pathway, AMP adenosine, or from IMP or GMP; they all ultimately converge onto it with the production of uric acid. So xanthine oxidase then is a useful therapeutic target and this then is the at least part of the mechanism by which 16 URIC ACID METABOLISM AND MEDICATIONS Allipurinol works. Notice that in, in fact, Allipurinol is itself a purine. It’s got the six-membered ring, it’s got the five-membered ring, and it’s got the nitrogens. It’s an analog of the purines and, indeed, it actually gets acted upon via xanthine oxidase and, in the process, this compound, alloxanthine, is generated. Now it turns out that alloxanthine binds really tightly, in fact I think there’s even a covalent bond between alloxanthine and the binding site, the substrate binding site in xanthine oxidase. This is a form of so-called suicide inhibition and, as a consequence of that, Allipurinol is quite specific in its effects and it’s very powerful in its effects and it’s a great drug. This is some information on xanthine oxidase. Maybe the main point to make from this slide, which otherwise is kind of useful background information while we’re thinking about how Allipurinol works, is that its mainly in hepatacytes where we’re seeking to block it clinically and in the hepatacytes in the cytomplasmic enzyme. Here’s a new xanthine oxidase inhibitor. It’s not on the market in this country. I don’t know… I think there’ll be some resistance to this drug coming onto the market simply because Allipurinol is so successful and relatively cheap and there are generic forms of it and so on. Here’s Febuxostat; this new one that we’re just talking about, and here’s Allipurinol. Allipurinol is a purine and you can see that Febuxostat is not a purine. Nevertheless, its binds very tightly in the substrate binding site for xanthine oxidase and blocks it. Alternative approaches to lowering uric acid levels: the so-called uricosurics are the agents which promote excretion of uric acid in the kidney. They do so by blocking re-absorption in the proximal tubule of the kidney but they do have 17 URIC ACID METABOLISM AND MEDICATIONS this side-effect of promoting uric acid delivery into the fluid of the renal tubules and therefore promoting renal calculus formation. This drug, Benzbromerone, is a new version – here it is again here – of these uricosurics; Probenecid is the one that’s on the market here at present. You will, occasionally see it being used but I think, in general, I would think it would be a good idea to avoid this drug, at least in the first instance, and start with Allopurinol in terms of trying to lower serum uric acid levels. There’s a potential advantage of Benzbromerone that it is effective in the context of renal failure so if the patient has renal failure, there is a need to try to promote or boost uric acid excretion. Probenecid is not to work in patients with renal failure. Benzbromerone, on the other hand, does seem to be effective in that context. We said right back at the start of the lecture it seems odd that humans, unlike other primates, other mammals, lack the enzyme uricase, the enzyme that converts uric acid to allantoin, the water-soluble metabolite. So, on the other hand, if you deliver uricase to a patient, for example in the form of Rasburicase, which is on the market here for the specific case of trying to cope with the Tumor Lysis Syndrome, then you can convert uric acid to the water-soluble form, allantoin, and promote its elimination. So it’s highly effective in mobilising uric acid from tophi and in the context of the Tumor Lysis Syndrome. So there are situations in which this approach can be very powerful. It wouldn’t normally be used just for somebody with recurrent attacks of gouty arthritis. 18 URIC ACID METABOLISM AND MEDICATIONS It’s for the special case where you want to try to mobilize uric acid from subcutaneous deposits associated with tophi. You need to lower the serum uric acid levels substantially to be able to start to mobilize uric acid under those circumstances from those subcutaneous deposits; also in the situation in which the purine load is really massive as in the acute Tumor Lysis Syndrome. And this table then seeks to just contrast the potential benefits and potential downsides of different types of therapy. In terms of drugs that are currently on the Australian market, Allanpurinol is there sort of blocking uric acid synthesis via blocking xanthine oxidase, Probenecid is there to promote uric acid excretion by blocking re-absorption in the kidney and uricase is there for the dissolution of tophi or, perhaps more commonly, in the Tumor Lysis Syndrome. Okay, so we’ve reached the end. Gout is a crystal arthopathy so it’s an acute form of arthritis. It tends to be one joint at a time and its due to the local formation of crystals and the local inflammatory response to those crystals in the joints mediated by neutrophils. Uric acid is derived from the breakdown of purines and we’ve seen both the impact of the de novo synthesis pathway to promote uric acid production and the role of the salvage pathways particularly in certain tissues to recover purine bases back into the purine nucleotype core and, as a consequence of that, suppress uric acid synthesis. Uric acid levels will rise if the de novo pathway synthesis is switched on, or of the salvage pathway is switched off and the most dramatic example of salvage pathways being switched off is in the Lesch Nyhan Syndrome where, in fact, 19 URIC ACID METABOLISM AND MEDICATIONS the enzyme that’s responsible for catalyzing that particular salvage pathway, which is hypozanthine or guanine, was not available. There’s also a dietary impact on uric acid levels and we considered the way in which ethanol can have an impact on uric acid via that process whereby acetate gets converted to Acetyl CoA, acetate being at the bottom of the ethanol oxidation pathway. Ethanol, acid aldehye, acetate, in the mechanism in the process of acetate being converted to Acetyl CoA, we saw that ATP was needed and that ATP being converted to AMP can then serve as a source of additional purines for the production of uric acid. It doesn’t look like a particularly impressive pathway; how can it happen? I think one thing we need to remember is that the ethanol concentration in those that use it are actually quite high. Remember we made the point in the ethanol lecture that ethanol is a weak drug. The levels actually have to be quite high to achieve any effect and, as a consequence of that, the levels get quite high inside the cells and therefore there’s a substantial impact on purine nucleotide metabolism inside the cells as well. So it’s about load. What concentrations of purines are actually being generated inside the cell to fuel uric acid production? We’ve seen the treatment of acute gout focuses on suppressing inflammation but that its also useful to treat hyperuricemia, either with a view to preventing subsequent attacks of acute gout or to mobilize uric acid in tophi or to control uric acid production in the Tumor Lysis Syndrome. Are there any question? Yes? Okay, Ben? (INAUDIBLE QUESTION FROM BEN IN AUDITORIUM) 20 URIC ACID METABOLISM AND MEDICATIONS So the question is why in treating acute gout with an agent that lowers the serum uric acid level, in some way worsen the acute attack? It’s not understood, Ben. Whether it means that there are sudden shifts in uric acid levels that can lead to crystallization or whether there is some other biochemical factor is not known. So its hand waving at the moment. We’ve got a question here but there’s one over here first. So the question is if you lose weight quickly, can that have an impact on the uric acid level? And I guess the implication is that it could rise. So, just as in the case of the Tumor Lysis Syndrome providing a large amount of biochemistry substrate for uric acid production, I would think that in sudden loss of weight it could have the same effect. (INAUDIBLE QUESTION FROM AUDITORIUM) Yes, potentially exercise… It depends… I guess the key question is whether there is a fairly rapid mobilization of nucleotides out of DNA or RNA because there’s a substantial load potentially of purine nucleotides in those biochemical substances. Yes? (INAUDIBLE QUESTION FROM AUDITORIUM) So the question is why is it in particular the hallux joint of the great toe, you know, the great toe is often one? I can’t explain to you about why it should be that particular joint other than to say I suppose that one of the key questions here is what is actually leading to the formation of the crystals in the first place and if there’s, say, local damage in a particular joint? Of course the hallux, you 21 URIC ACID METABOLISM AND MEDICATIONS know, the great toe is exposed to repetitive minor injury on a daily basis. It’s possible that that environment makes it more likely for crystals to actually form. Any other questions? Right, if not, thank you. [APPLAUSE] 22