Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
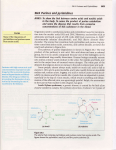
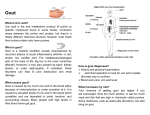
Gout - ‘The Disease of Kings’ By Dr John Pridgeon Hyperuricaemia is defined as an increased concentration of uric acid in the blood, may result in gout, a syndrome that may have 3 distinct manifestations: 1. The best known of these is gouty arthritis that follows the violent and profound inflammatory response that results from the formation of monosodium urate monohydrate crystals within a joint. Those who have had an acute attack of gout will know how painful this condition can be. The most commonly affected joint by far, is the hinge of the big toe, or the first metatarso-phalangeal joint. This is the joint in the body that works the hardest. Bio-mechanically this joint must be subjected to stresses up to five times the body weight every time we stride forward (and therefore is the joint most easily traumatised by normal routines). Trauma or previous joint damage may cause a particular joint to become painful. Gout may affect other weight-bearing joints – ankle, knee or hip, but any joint may be affected, and creaky joints may herald an attack. Typically the pain is relieved when weight bearing is stopped and the leg elevated. Attacks usually only last a day or two, but weeks of pain have been reported. An attack often follows overindulgence with either food or alcohol, and January is a common time for an attack to occur. Gouty arthritis affects about 1% of the population, and up to 10% of the Maori adult male population! 2. 15% of all kidney stones are made up of uric acid. Kidney stones are worth avoiding. Some women claim that giving birth to a child is less painful than producing a large stone. 3. The last form of gout is tophaceous gout. This is the name given to the build up and deposition of uric acid in the soft tissues. This resembles toothpaste or chalk. Usually this is a feature of longstanding and severe hyperuricaemia (greater than 10 years) People may be hyperuricaemic, and not develop any of these forms of gout. The higher uric acid levels becomes, the more the chance of developing signs and symptoms. An estimated 10% of people suffering from gouty arthritis do so with uric acid levels still within the normal reference range, for example Classically gout sufferers are described as either over-producers or under-excretors. Gout is often associated with obesity, heavy alcohol intake, and a meat rich diet – but this is not always the case. Gout most commonly affects males, and may occur at any age after the late teens, depending upon the victim’s dietary habit and genetic predisposition. Premenopausal women are rarely affected. Certain medicines, notably diuretics, may elevate urate levels. Gout is easily treated in most cases. People who suffer from repeated attacks do so because they simply fail to deal with the problem. Like overweight people with high blood pressure, high cholesterol and diabetes, gout is something that can easily and adequately be managed purely by lifestyle changes. Treatment: Wherever possible and reasonable, non-drug action should be taken. The response to therapy is judged by serial estimation of uric acid levels and response of signs and symptoms. The cornerstones of gout prevention are threefold: 1. Drink adequate amounts of filtered water: 30mls of water per kilogram body weight per day will allow the kidney to excrete the excess of urate more efficiently. 2. Alkalinise your urine with 2 teaspoons of urinary alkaliniser twice per day during acute attacks, and I teaspoon daily as a prophylactic measure. Uric acid is a weak acid, and as such alkalinisation of the urine promotes a more rapid and effective excretion by the kidney. 3. Alter your diet, and lose weight to a BMI (body mass index = height x height divided by your weight) of 25kg/metre squared. Rapid and sudden fasting may predispose to an acute attack. The victim and his doctor should aim for a urate level that is within normal limits and preferably somewhere at less than 60% of the upper limit. However, where the gout is seen to be severe, (frequent arthritic episodes, stones or tophi are present, or urate levels are very high) then drug therapy is probably indicated for at least a few months, and if the problem persists, then maintenance therapy for a long period may be indicated, so that uric acid stored in the soft tissues may be lost. The drug therapy modalities are three, inclusive of pain management. The main idea of maintenance therapy though, is to either slow down urate production, or to increase its rate of excretion by the kidney. It is likely that a substantial amount of uric acid has been deposited within the soft tissues of the body during the time that uric acid levels have remained high. The trick here is to reverse the storage/deposition tendency by creating a diametrically opposite concentration gradient – one where stored urate is converted back to blood uric acid (by a low blood concentration), and then excreted by the kidney. 1. The management of pain: Elevate the foot and do not weight bear in the acute phase of the arthritis. Any antiinflammatory will suffice. I have found an injection of high dose 150mg of diclofenac (‘Voltaren’) given by intramuscular injection is very effective. Probably the best pain relief is afforded by indomethacin (‘Arthrexin’)100mg suppositories given twice daily as required. Colchicine is a gout specific analgesic. It is given 2mg immediately, then 1mg every half hour until the pain is relieved. Unfortunately relief of pain is almost always accompanied by an impressive diarrhoea. If you do not get diarrhoea then you probably will not get any relief either as the does is too low. Other pain killers, e.g. paracetamol, codeine, caffeine etc. will assist but antiinflammatories are the mainstay of pain relief. 2. Decrease of uric acid production: Allopurinol is a xanthine oxidase inhibitor. This enzyme is employed twice in the chain reaction that converts purines (the dietary source of uric acid) to uric acid. Up to 900mg per day may be used in an attempt to normalise blood levels of urate, but usually 300 mg per day is more than enough to control uric acid production. 3. Increase uric acid excretion: Colchicine helps the kidneys excrete uric acid in low doses – 1mg daily; Benzbromarone 20 mg daily has the same effect; Probenecid 500mg – 2g daily Blood uric acid levels will show you if your treatment is effective or needs improving. Dietary restrictions: 1. Avoid foods that have a high purine content – Herring, fish roe, meat extracts. Sardines, yeast, anchovies, bacon, chicken soup, gravy, beef, mutton, game meat/birds, organ meat (brains, tripe, liver, kidneys), sausages, exotic seafoods and shellfish (mussels/oysters). Some vegetables are also high in purines, asparagus, dried beans and lentils, mushrooms and spinach. Tomatoes are often blamed for an attack. 2. Avoid alcohol as this delays uric acid excretion – red wine and beer seem to be the worst culprits. 3. Avoid food that causes heartburn or increased acidity – citrus, vinegar, garlic, tomatoes, pies and bread. 4. Smoking causes the overproduction of acid by the stomach, by a factor of 3500%! This causes your body to be acidic and predisposes to attacks. 5. High blood pressure medication may need changing too.