Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
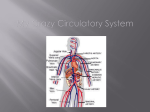
Circulation Except for the smallest, simplest multicellular animals, all organisms need a circulatory system of some sort. In those animals without a circulatory system, all cells must be close to the ‘surface’, so that simple diffusion can bring oxygen and food molecules to cells and carry wastes out. A jellyfish is a good example of an animal that can do without a circulatory system. Circulation occurs within the gastrovascular cavity. Flatworms similarly have an extensive gastric system that moves both food and wastes. In most species, no cell is more than a millimeter or so from the body surface to exchange gases (O2 in, CO2 out). For those that have circulatory systems, the simpler systems are open circulatory systems. Blood is pumped by a heart into vessels that are open to the body cavity at their ends. Blood is returned to the heart through ‘pores’. This is the way circulation works in insects. In a closed circulatory system (like ours) blood is pumped by a heart out to regions of the body in vessels called arteries, which divide into finer vessels called arterioles, then, in the immediate neighborhood of the cells served, cells in the blood move single-file through capillaries. The return of blood to the heart occurs by joining capillaries together into venioles, then combining them into larger vessels, the veins. In animals with low metabolic rates, the heart may be only two or three chambers (which mixes blood recently oxygenated with blood having little oxygen. That wouldn’t work for us. Warm-blooded animals (homeotherms) need to move far more oxygen and food into tissues, and have a 4-chambered heart to achieve that. frogs birds fish & mammals With a 4-chambered heart there are separate circuits that: a)oxygenate the blood by circulating the blood through the lungs (the pulmonary circuit) that occupies the right side of the heart, and b)move the blood to all other body organs (brain, digestive system, muscles, etc.) using the systemic circuit. Follow the numbers in the diagram to follow the movement of the blood. In this sequence circulation to the head and to the ‘lower’ body occurs in parallel, so that 7 and 8 are occurring at the same time, as are 9 and 10. The heart beats (the muscle contracts) to move blood through the system. There is significant pressure in the system as the heart muscle contracts (systole). Arteries have smooth muscle in their walls to tolerate this pressure, then to ‘recover’ during the phase of the heartbeat when the heart muscle is relaxed (diastole). Veins also have smooth muscle in their walls, but the thickness of the muscle layer is much smaller, since the pressure in veins is lower. Heart muscle contraction rate (your pulse rate) is regulated by both the nervous system and by hormones. The sympathetic nervous system can affect heart rate by accelerating pulse rate. The sympathetic system has two ‘parts’, commonly named by their actions: a) feeding and f___ing – don’t accelerate heart rate b) fighting or fleeing – these do produce an acceleration of heart rate – epinephrine is released c) There is also a CO2 sensor in the brain that accelerates heart rate when exercise increases blood CO2 level. The heartbeat is initiated by a natural pacemaker, a batch of nerve cells located in the sino-atrial node that fire automatically at a basal rate. You can’t have the whole heart contracting at once. Instead, like squeezing toothpaste from a tube, contraction has to squeeze the blood out by: 1)beginning contraction of the atria at the top, moving the blood into the ventricles, then 2)beginning contraction of the ventricles at the bottom, to move blood into the pulmonary artery and the aorta. That pattern is logical for the atria, but to get the ventricles to begin at the bottom there are special muscle fibers, called the bundle of His, that carry the excitation from the atria down to the base of the heart, then spread over the ventricles as Purkinje fibers. bundle of His The electrical activity of heart muscle cells is evident at the skin, and is recorded in an EKG (an electrocardiogram by doctors (the K comes from the original German). Changes in the shape of the wave are indicators of change in heart function, e.g. a heart attack. Heart muscle cells die. Why do heart attacks occur? Because blockage occurs in an artery supplying the heart muscle. The blockage may develop in the cardiac artery itself, due to buildup of atherosclerotic plaque, or may be a clot formed within the vessel. The picture shows both in the same artery: We all have some plaque in our arteries. The object is to limit the amount of buildup, e.g. through a low cholesterol diet and exercise. The same sort of blockage, preventing blood flow to a part of the brain, is what we call a stroke. A different problem can result if blood pressure rises to high enough pressures that arteries fail, and the rupture leaks blood into surrounding tissues. The set of problems that result from circulatory problems are collectively called cardiovascular disease, and accounts for ~40% of deaths in North America. Normal blood pressure for a healthy young adult averages about 120/80 (a systolic pressure of 120 mm Hg, and a diastolic pressure of 80 mm Hg). Systolic pressures from 130 to 140 are now called “high normal”. Blood pressures above 140 systolic or above 90 diastolic are high. Essential hypertension can be treated by: 1) Increasing kidney output, draining fluid from the system 2) Adjusting the strength of the heartbeat with drugs called “blockers” Blood pressure varies quite a bit over the course of a day, by as much as 20-30 mm Hg without any obvious cause, and by more under stress. The occurrence of hypertension also varies. Factors such as: 1) sex (men at younger age and women at higher age more frequently show hypertension) 2) race (blacks have a higher frequency of hypertension than other races) 3) genetics (the propensity for hypertension seems to run in families) 4) lifestyle (sedentary jobs/lifestyle are more prone to hypertension) Blood moves through the circulatory system in blood vessels (arteries, arterioles, capillaries, venioles, veins) in what we call a closed system. How, then, do gases, food, and waste get exchanged between tissue cells and the circulatory system? The answer comes from: a) designed-in leakiness and b) the balance between blood pressure and osmotic pressure Leakiness – water, salts and sugar simply leak out into the tissue fluid through the clefts between cells. The gases (O2 and CO2) simply diffuse through the capillary walls. There are, however, two other components to substance movement… Some molecules too large to pass through the gaps between capillary wall cells are moved actively from the lumen of the capillary into cells forming the epithelial wall by endocytosis (engulfed into a vesicle of the cell), then moved out into tissue fluid by exocytosis (emptied out of the vesicle when it ‘joins’ the outside cell membrane). The balance between blood and osmotic pressure also moves materials. At the arterial end of a capillary, blood pressure is higher than osmotic pressure, so materials are ‘pushed’ out. At the venous end, osmotic pressure is greater than blood pressure, and the net movement is inwards. Not all fluid leaving capillaries can be recollected by this pressure difference. A second system of vessels, called the lymphatic system, also returns fluid to circulation by joining the large veins (particularly the superior and inferior vena cava) near the heart. There are four major components of blood: 1) plasma 2) red blood cells (erythrocytes) 3) white blood cells (leukocytes) 4) platelets Both plasma and leukocytes are more complex than a single term suggests. 1) plasma – constitutes slightly more than ½ of normal blood volume. A measure called the hematocrit tells you what fraction of blood is (mostly) red blood cells. If you donate blood, you will remember having your finger poked and a droplet of blood tested. If your hematocrit is too low, you won’t be allowed to donate. Plasma contains water, a number of salts and ions, proteins characteristic of blood, and substances being transported. 2) erythrocytes – these cells are unique, in that they have no nucleus or mitochondria. Since they can’t repair themselves, they have a limited lifespan (~100 – 120 days). Defective cells are broken down in the liver and spleen. The heme (iron) is mostly recycled back into bone marrow to build new erythrocytes. The oxygen-carrying molecule is hemoglobin. It’s a protein in 4 subunits (2 and 2 β chains) with a heme in the middle. To maximize surface area for gas exchange, each cell looks like a doughnut from which the hole hasn’t been completely punched out. 3) leukocytes – there are at least five types of white blood cells, with different functions established for four of them. Polymorphonuclear leukocyte = neutrophil a. basophils – fight infection by releasing chemicals (e.g. histamine) that are part of the inflammation process b.neutrophils and monocytes – both types move out of the capillaries and act as phagocytes, engulfing (eating) foreign bacteria and proteins that have entered through wounds. They die in the process. c.lymphocytes – are the key cells in the immune response (next lecture). d.eosinophil – gets its name from staining with eosin, but its functions are not well understood. They seem to be released when parasitic infection occurs, and release chemicals that kill the invaders. Blood clotting Assuming you’ve been injured and have a bleeding wound, there are two basic parts to the initial healing: 1) initially stopping the flow of blood by plugging the hole 2) constructing a longer lasting clot (a scab). Phase 1 is a response of the platelets when connective tissue (collagen) is exposed. The platelets at the site of injury adhere to the collagen and release clotting factors that cause more platelets to become sticky and together form a plug. In phase 2 the clotting factors initiate a chain of reactions that result in a clot. The key clotting factor (which is in circulation in the tissue fluid, as well released by platelets) is thromboplastin. Thromboplastin (with Ca++) acts as a catalyst for the conversion of prothrombin to thrombin. Thrombin, in turn, acts as a catalyst in the conversion of fibrinogen to fibrin (whose name suggests what it is like – fibers that trap erythrocytes, other cells, and debris to form the clot (scab). Here’s what the process looks like graphically and as a series of enzymatic steps: