Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Cardiac contractility modulation wikipedia , lookup
Coronary artery disease wikipedia , lookup
Remote ischemic conditioning wikipedia , lookup
Echocardiography wikipedia , lookup
Hypertrophic cardiomyopathy wikipedia , lookup
Lutembacher's syndrome wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
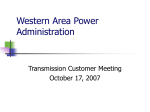
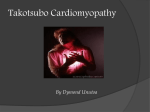
Mechanisms of Acute Mitral Regurgitation in Patients With Takotsubo Cardiomyopathy An Echocardiographic Study Masaki Izumo, MD, PhD; Smruti Nalawadi, MD; Maiko Shiota, MD; Jayanta Das, MD; Suhail Dohad, MD; Eiji Kuwahara, MD, PhD; Yoko Fukuoka, MD; Robert J. Siegel, MD; Takahiro Shiota, MD, PhD Downloaded from http://circimaging.ahajournals.org/ by guest on May 10, 2017 Background—Recent studies have suggested acute mitral regurgitation (MR) as a potentially serious complication of takotsubo cardiomyopathy (TTC); however, the mechanism of acute MR in TTC remains unclear. The aim of this study was to elucidate the mechanisms of acute MR in patients with TTC. Methods and Results—Echocardiography was used to assess the mitral valve and left ventricular outflow tract (LVOT) pressure gradient in 47 patients with TTC confirmed by coronary angiography and left ventriculography. Mitral valve assessment included coaptation distance, tenting area at mid systole in the long-axis view, and systolic anterior motion of the mitral valve (SAM). Of the study patients, 12 (25.5%) had significant (moderate or severe) acute MR. In patients with acute MR versus those without acute MR, we found lower ejection fraction (31.3⫾6.2% versus 41.5⫾10.6%, P⫽0.001) and higher systolic pulmonary artery pressure (49.3⫾7.4 versus 35.5⫾8.9 mm Hg, P⬍0.001). Moreover, 6 of the 12 patients with acute MR had SAM, with peak LVOT pressure gradient ⬎20 mm Hg (average peak LVOT pressure gradient, 81.3⫾35.8 mm Hg). The remaining 6 patients with acute MR revealed significantly greater mitral valve coaptation distance (10.9⫾1.6 versus 7.8⫾1.4 mm, P⬍0.001) and tenting area (2.1⫾0.4 versus 0.95⫾0.25 cm2, P⬍0.001) than those without acute MR. A multivariate analysis revealed that SAM and tenting area were independent predictors of acute MR in patients with TTC (all P⬍0.001). Conclusions—SAM and tethering of the mitral valve are independent mechanisms with differing pathophysiology that can lead to acute MR in patients with TTC. (Circ Cardiovasc Imaging. 2011;4:392-398.) Key Words: cardiomyopathy 䡲 mitral valve insufficiency 䡲 echocardiography T akotsubo cardiomyopathy (TTC), which also is called apical ballooning syndrome or stress cardiomyopathy, is recognized as transient left ventricular (LV) apical ballooning and electrocardiographic changes that mimic acute myocardial infarction in the absence of obstructive coronary artery disease.1–3 This syndrome generally has a favorable outcome; however, some complications may occur in the acute phase.4 – 6 Management of such patients remains difficult.4 – 6 Two recent studies suggested acute mitral regurgitation (MR) as a potentially serious complication of TTC, which accounts for 19% to 21% of patients with TTC.7,8 Both studies concluded that the systolic anterior motion of the mitral valve (SAM) plays a crucial role in the mechanism of acute MR in patients with TTC, although only one third to one half of the patients with acute MR had SAM. The mechanism of acute MR without SAM is unclear. The aim of this study was to elucidate the mechanisms of acute MR in patients with TTC. Clinical Perspective on p 398 Methods Study Population This study reviewed 48 consecutive patients with chest pain or dyspnea and changes on ECGs who underwent coronary angiography and left ventriculography to confirm TTC in the Cedars-Sinai Medical Center between October 2006 and May 2009. The inclusion criteria were (1) balloon-like LV with apical akinesis or dyskinesis on initial left ventriculography or echocardiogram, (2) ST-segment or T-wave abnormalities on ECG and increases in blood concentrations of cardiac troponin level, (3) no significant coronary artery stenosis confirmed by coronary angiography, and (4) absence of pheochromocytoma and myocarditis.9 One patient with TTC who had significant MR due to organic mitral valve disease was excluded; thus, a total of 47 patients were included. All patients were given a diagnosis of TTC by consensus of 2 experienced cardiologists. This study was approved by the institutional review board of Cedars-Sinai Medical Center. Received November 3, 2010; accepted April 11, 2011. From Cedars-Sinai Heart Institute, Cedars-Sinai Medical Center and UCLA, Los Angeles, CA. Correspondence to Takahiro Shiota, MD, PhD, Cedars-Sinai Heart Institute, Cedars-Sinai Medical Center and UCLA, 8700 Beverly Blvd, Los Angeles, CA 90048. E-mail [email protected] © 2011 American Heart Association, Inc. Circ Cardiovasc Imaging is available at http://circimaging.ahajournals.org 392 DOI: 10.1161/CIRCIMAGING.110.962845 Izumo et al Downloaded from http://circimaging.ahajournals.org/ by guest on May 10, 2017 Figure 1. Mitral leaflet configurations in the parasternal longaxis echocardiogram. Cardiac Catheterization and Blood Test All patients underwent coronary angiography and left ventriculography within 24 hours after symptom onset. Left ventriculography was used to calculate LV ejection fraction (EF) and LV volume using the Simpson method. Venous blood was collected every 3 hours to measure the troponin I concentration in the acute phase and continued until a peak value was observed. Echocardiographic Examination All patients with TTC underwent 2D and Doppler echocardiographic examinations with an iE-33 system (Philips Medical Systems; Andover, MA) within 24 hours of admission. Follow-up echocardiography was performed within 4 weeks (range, 1 to 4 weeks) after initial presentation. The LV wall motion score index (WMSI) was calculated on the basis of a 16-segment model recommended by the American Society of Echocardiography.10 Mitral valve configuration at mid systole was assessed in a parasternal long-axis view. Mitral valve coaptation distance was defined as the distance from the mitral annular plane to mitral leaflet coaptation point. The mitral valve tenting area was measured by the area enclosed between the annular plane and mitral leaflets (Figure 1).11 MR was quantitated by measuring the vena contracta (narrowest jet origin) in a long-axis view perpendicular to the coaptation line averaged in 3 cardiac cycles. Additionally, MR jet area and left atrial (LA) area at mid systole was measured by area trace method on the 4-chamber view, and their ratio (MR jet area/LA area) was calculated as previously reported.12 Vena contracta width (VCW) ⱖ0.3 cm and MR jet area/LA area ⱖ20% were considered as moderate in degree.13 All parameters of mitral deformation were obtained at mid systole. LV outflow tract (LVOT) pressure gradients were measured by continuous-wave Doppler echocardiography through the LVOT. A dynamic gradient was considered significant if peak LVOT pressure gradient was ⬎20 mm Hg by continuous-wave Doppler echocardiography based on the modified Bernoulli equation. 4 With continuous-wave Doppler echocardiography, the maximum peak tricuspid regurgitant velocity recorded from any view was used to determine the pulmonary artery systolic pressure (PASP) with the simplified Bernoulli equation [PASP⫽4(peak velocity)2⫹mean right atrial pressure]14; mean right atrial pressure was estimated based on the most recent American Society of Echocardiography recommendation.15 Statistical Analysis All values are expressed as mean⫾SD. An unpaired t test was used to compare the continuous variables between the patients with MR Acute MR in Takotsubo Cardiomyopathy 393 and those without MR, and the 2 and Fisher exact test were used for the categorical variables. A paired t test was used to compare initial and follow-up measurements. Univariate logistic regressions were used to relate clinical and echocardiographic variables to prevalence of MR. Multivariate logistic regression was performed to identify factors associated with prevalence of MR. Significant variables on univariate analysis entered into models were peak LVOT pressure gradient, PASP, and WMSI on clinical and echocardiographic parameters in patients with TTC MR with SAM and LVEF, LV end-systolic volume, tenting area, coaptation distance, mitral annular dimension, and PASP on clinical and echocardiographic parameters in patients with TTC MR without SAM. Differences were considered significant if P⬍0.05. Both intraobserver and interobserver variabilities for measurements of mitral valve tenting area, coaptation distance, VCW, and MR jet area/LA area were obtained by analysis of 10 random images by 2 independent, blinded observers and by the same observers at 2 different times. The results were analyzed by both the intraclass correlation coefficient and the Bland-Altman method.16 Statistical analyses were performed using SPSS version 17.0 (SPSS, Inc; Chicago, IL) software. Results Of 47 patients with TTC (mean age, 68.5⫾15.4 years; range, 28 to 89 years), 44 (93.6%) were women. Physical stressors such as pneumonia, asthma attack, traffic accident, hematemesis, and overwork were identified in 22 (46.8%) patients, and emotional stressors were also identified in 9 (19.1%) patients. On ECG, ST-segment elevation was present in 24 (51.0%) patients, ST depression in 5 (10.6%), and T-wave inversion in 18 (38.3%). Twelve (25.5%) patients had significant (moderate or severe) acute MR on presentation (mean VCW, 0.60⫾0.19 cm; MR jet area/LA area, 53.2⫾10.9%). Of these, 10 (83.3%) patients with MR were women, and 6 (50%) had a peak LVOT pressure gradient ⬎20 mm Hg (average peak LVOT pressure gradient, 81.3⫾35.8 mm Hg) and SAM. Comparison of Clinical and Echocardiographic Characteristics Comparison of clinical and echocardiographic characteristics between patients with TTC with MR and those without MR are listed in Table 1. Age, sex, and troponin I levels did not significantly differ between the 2 groups. We found lower LVEF (P⫽0.006) and higher mitral tenting area, peak LVOT pressure gradient, and PASP (all P⬍0.001) in patients with TTC with MR. The ratio of patients with TTC who presented with shortness of breath on admission also was greater in those with MR than in those without MR (75.0% versus 28.5%, P⫽0.003). Moreover, we stratified 12 patients with MR into 2 groups based on the presence or absence of a peak LVOT pressure gradient ⬎20 mm Hg. All 6 patients with increased LVOT pressure gradients had SAM, and the remaining 6 patients had significantly higher mitral valve coaptation distance (10.9⫾1.6 versus 6.8⫾0.6 mm, P⬍0.001) and tenting area (2.1⫾0.4 versus 1.0⫾0.1 cm2, P⬍0.001), larger LV end-systolic volume (61.8⫾17.2 versus 49.1⫾4.9 mL, P⫽0.035), and lower EF (28.0⫾6.9 versus 34.8⫾2.9, P⫽0.001) than patients with TTC with MR due to SAM. All patients with MR are listed in Table 2. 394 Circ Cardiovasc Imaging Table 1. July 2011 Patient Characteristics Patients With Significant MR Patients Without Significant MR (n⫽35) Age, y All (n⫽12) 68.5⫾15.4 Female, % 71.6⫾8.8 97.1 Troponin I, g/L With SAM (n⫽6) 71.6⫾7.3 83.3 Without SAM (n⫽6) 71.5⫾10.7 83.3 83.3 4.2⫾5.7 5.1⫾3.1 6.6⫾3.7 4.1⫾1.5 LVEF, % 41.5⫾10.6 31.3⫾6.2* 34.8⫾2.9* 28.0⫾6.9*† LVEDV, mL 89.5⫾15.4 84.9⫾14.9 81.3⫾9.3 86.0⫾18.9 LVESV, mL 50.4⫾12.4 56.0⫾14.2 49.1⫾4.9 61.8⫾17.2*† MR VCW, cm 0.02⫾0.08 0.60⫾0.19* 0.70⫾0.14* 0.52⫾0.20* MR jet area/LA area, % 1.2⫾4.0 53.2⫾10.9* 56.0⫾10.1* 50.5⫾11.8* Peak LVOT pressure gradient, mm Hg 9.7⫾13.3 43.0⫾46.8* 81.3⫾35.8*† 4.7⫾1.9 0.95⫾0.25 1.5⫾0.6* 1.0⫾0.1 2.1⫾0.4*† 7.8⫾1.4 9.0⫾2.4 6.8⫾0.6 10.9⫾1.6*† Mitral annular dimension, mm 26.6⫾3.6 30.2⫾3.5* 29.3⫾3.2 31.2⫾3.7* PASP, mm Hg 35.5⫾8.9 49.3⫾7.4* 50.3⫾9.6* 48.2⫾5.9* 1.9⫾0.1 2.2⫾0.2* 2.1⫾0.2* Tenting area, cm2 Downloaded from http://circimaging.ahajournals.org/ by guest on May 10, 2017 Coaptation distance, mm WMSI 2.3⫾0.2*† Data are presented as mean⫾SD, unless otherwise indicated. LA indicates left atrium; LVEDV, left ventricular end-diastolic volume; LVEF, left ventricular ejection fraction; LVESV, left ventricular end-systolic volume; LVOT, left ventricular outflow tract; MR, mitral regurgitation; PASP, pulmonary artery systolic pressure; VCW, vena contracta width; WMSI, wall motion score index. *Significant difference (P⬍0.05) patients without MR vs each group. †Significant difference (P⬍0.05) patients with SAM vs without SAM. Relationship Between Clinical and Echocardiographic Findings and Acute MR in TTC significant variables obtained by the univariate analysis, resulting in peak LVOT pressure gradient and mitral valve tenting area (all P⬍0.001) as independent predictors of acute MR in patients with TTC (Tables 3 and 4). Univariate analysis was performed in patients with TTC MR with SAM (versus patients without MR) and those without SAM (versus patients without MR) (Tables 3 and 4). The results of the univariate analysis demonstrated that the occurrence of acute MR in patients with TTC was significantly associated with LV ejection fraction, peak LVOT pressure gradient, mitral valve tenting area, PASP, and WMSI, respectively. The multivariate analysis also was performed to assess Table 2. Patient No. Follow-Up Echocardiographic Findings Follow-up echocardiography was performed in 39 patients with TTC (83.0%) within 4 weeks after initial presentation. Figures 2 and 3 show 2D echocardiograms obtained at initial presentation and at follow-up in 2 typical patients with TTC with MR due to SAM and tethering. LVEF, WMSI, VCW, Characteristics of 12 Patients With TTC MR Age/Sex, y Triggered Event ECG on Admission LVEF, % Peak LVOT Pressure Gradient, mm Hg SAM Tenting Area, cm2 Coaptation Distance, mm PASP, mm Hg 1 70/F Physical stress (overwork) ST depression 35 104 ⫹ 0.99 6.1 43 2 76/F Emotional stress ST elevation 32 5 ⫺ 1.75 9.1 40 3 79/F Unknown ST elevation 35 84 ⫹ 0.91 7.5 56 4 75/F Emotional stress ST elevation 33 114 ⫹ 1.01 6.6 50 5 66/F Physical stress (pneumonia) T inversion 40 83 ⫹ 1.22 7.4 43 6 66/M Physical stress (chemotherapy) ST elevation 20 4 ⫺ 2.5 12.3 52 7 61/F Physical stress (hematemesis) T inversion 22 3 ⫺ 2.52 12.4 45 8 86/F Unknown T inversion 30 8 ⫺ 1.92 9.1 45 9 80/F Unknown T inversion 34 3 ⫺ 1.8 6.8 44 10 60/F Unknown ST elevation 32 5 ⫺ 1.84 10.2 43 11 61/F Physical stress (overwork) ST elevation 32 45 ⫹ 0.93 10.2 65 79/M Physical stress (colitis) T inversion 34 38 ⫹ 1 6.3 40 12 ECG indicates electrocardiography; SAM, systolic anterior motion of the mitral valve; TTC, takotsubo cardiomyopathy. Other abbreviations as in Table 1. Izumo et al Acute MR in Takotsubo Cardiomyopathy 395 Table 3. Analysis of Clinical and Echocardiographic Parameters in Patients With TTC MR With SAM Univariate Analysis OR (95% CI) Multivariate Analysis P Age, y 1.14 (0.82–1.72) 0.078 LVEF, % 0.91 (0.80–1.04) 0.107 LVEDV, mL 0.71 (0.39–1.27) 0.238 LVESV, mL 0.988 (0.87–1.12) 0.967 3.64 (1.64–8.07) ⬍0.001 Peak LVOT pressure gradient, mm Hg 2 OR (95% CI) P 3.16 (1.26–7.92) ⬍0.001 Tenting area, cm 1.02 (0.98–1.05) 0.496 Coaptation distance, mm 1.16 (0.79–1.76) 0.695 Mitral annular dimension, mm 1.10 (0.99–1.24) 0.087 PASP, mm Hg 1.44 (1.06–1.95) 0.004 1.56 (0.92–2.02) 0.065 WMSI 1.71 (1.17–2.52) 0.003 1.14 (0.24–3.21) 0.805 OR indicates odds ratio. Other abbreviations as in Tables 1 and 2. Downloaded from http://circimaging.ahajournals.org/ by guest on May 10, 2017 and MR jet area/LA area values were significantly improved at follow-up compared with initial presentation (LVEF, 41.2⫾11.7% versus 58.3⫾11.3%; WMSI, 2.0⫾0.2 versus 1.1⫾0.2; VCW, 0.60⫾0.19 versus 0.1⫾0.05 cm; MR jet area/LA area, 53.2⫾10.9% versus 8.2⫾2.5%; all P⬍0.001). Recovery in LV systolic function was similar in patients with and without MR (58.4⫾6.7% versus 59.4⫾11.9%, P⫽0.845). No abnormal LVOT pressure gradients were observed at follow-up. In patients with MR without SAM, coaptation distance and tenting area significantly decreased at follow-up compared to initial presentation (coaptation distance, 10.9⫾1.6 versus 7.9⫾0.5 mm; tenting area, 2.1⫾0.4 versus 1.1⫾0.2 cm2; all P⬍0.001). No other significant echocardiographic changes were detected by 2D and Doppler echocardiography. During the mean follow-up period of 25.5⫾6.7 months, no patients had recurrence of TTC. Reproducibility of Echocardiographic Measurements The intraobserver variability as assessed by intraclass coefficient were 0.91 (95% CI, 0.75 to 0.97) for mitral valve tenting area, 0.87 (95% CI, 0.72 to 0.94) for mitral valve coaptation distance, 0.88 (95% CI, 0.78 to 0.93) for VCW, and 0.90 (95% CI, 0.77 to 0.96) for MR jet area/LA area. The interobserver variability on these measurements were 0.89 (95% CI, 0.48 to 0.99), 0.84 (95% CI, 0.36 to 0.94), 0.88 (95% CI, 0.41 to 0.98), and 0.89 (95% CI, 0.48 to 0.97), respectively. The Bland-Altman method showed that intraobserver and interobserver variabilities, respectively, were 0.17 and 0.17 cm2 for mitral valve tenting area, 0.5 and 0.6 mm for mitral valve coaptation distance, 0.05 and 0.06 cm for VCW, and 3.2% and 4.1% for MR jet area/LA area. Discussion To our knowledge, this study is the first to demonstrate that (1) there are 2 entirely different mechanisms responsible for acute MR in patients with TTC and (2) PASP is significantly higher in patients with TTC with MR than in those without MR. In patients with TTC, complications may occur in the acute phase.4 – 6 Heart failure with or without pulmonary edema is the most common clinical complication.17 In the Table 4. Analysis of Clinical and Echocardiographic Parameters in Patients With TTC MR Without SAM Univariate Analysis OR (95% CI) Multivariate Analysis P Age, y 0.98 (0.96 –1.00) 0.706 LVEF, % 1.49 (1.02–2.17) 0.048 LVEDV, mL 0.97 (0.55–1.72) 0.846 LVESV, mL 1.04 (1.02–1.12) 0.047 Peak LVOT pressure gradient, mm Hg 0.80 (0.55–1.16) 0.288 Tenting area, cm2 5.46 (2.54–9.62) Coaptation distance, mm 3.67 (1.11–12.1) Mitral annular dimension, mm OR (95% CI) P 0.60 (0.13–2.78) 0.563 0.80 (0.47–1.37) 0.476 ⬍0.001 3.17 (1.04–8.62) ⬍0.001 0.013 1.69 (0.91–3.17) 0.212 1.44 (1.05–2.06) 0.023 0.97 (0.55–1.77) 0.328 PASP, mm Hg 1.44 (1.06–1.95) 0.029 1.27 (0.91–1.76) 0.363 WMSI 1.30 (0.86–1.93) 0.288 OR indicates odds ratio. Other abbreviations as in Tables 1 and 2. 396 Circ Cardiovasc Imaging July 2011 Downloaded from http://circimaging.ahajournals.org/ by guest on May 10, 2017 Figure 2. Two-dimensional transthoracic echocardiography in patients with mitral regurgitation (MR) due to systolic anterior motion of the mitral valve (SAM). A, Severe MR at initial presentation. B, Mitral valve SAM at initial presentation. C, Only trivial MR was found at follow-up. D, Mitral valve SAM was not found at follow-up. Note that all 4 images are from apical long-axis views. LA indicates left atrium; LV, left ventricle. present study, we found that ⬇25% of the patients with TTC had acute MR, which supported the results of earlier studies.7,8 Approximately one fifth of patients with TTC have clinically significant acute MR. Despite the favorable outcome of TTC, the associated presence of significant acute MR increases the risks of acute deterioration and adverse outcome in patients with TTC.8,18 In the present study, acute MR was identified in patients with TTC with lower EF; PASP was higher in patients with TTC with MR than in those without MR. The number of patients who presented with shortness of breath was greater in those with MR than in those without MR. Therefore, special attention should be paid to the hemodynamics in the acute phase of TTC, which often correspond to New York Heart Association class III heart failure.19 Earlier studies indicated that SAM was regarded as 1 of the causes of significant MR.7,20 Parodi et al7 reported that approximately one third of patients with TTC with significant MR had SAM. It is well-known that in patients with hypertrophic cardiomyopathy, SAM is associated with significant MR.21,22 Some case reports also demonstrated LVOT obstruction with SAM and acute MR in TTC.23,24 In the present study, 12% of all patients with TTC, 50% of the patients with TTC with significant MR, had SAM, which was identified as 1 of the predictors of acute MR in patients with TTC by multivariate analysis. However, we found another independent factor of acute MR in patients with TTC: mitral valve tenting area. Severe Figure 3. Two-dimensional transthoracic echocardiography in patients with mitral regurgitation (MR) due to apical displacement of the mitral valve. A, Severe MR at initial presentation. B, Apical displacement of the mitral leaflets was found at initial presentation. C, Only trivial MR was found at follow-up. D, Normal mitral leaflets close at the annular level at follow-up. Note that all 4 images are from the apical 4-chamber view. Abbreviations as in Figure 2. mitral valve tenting is known as an important cause of ischemic MR.25–27 Ischemic MR, a relatively common complication of coronary artery disease, occasionally occurs in the acute or chronic phase.27 Leaflet tethering by papillary muscle displacement due to regional or global LV dysfunction has been suggested as the main mechanism of chronic ischemic MR.25–27 In the present study, patients with MR without SAM had lower EF and higher WMSI and end-systolic volume than those with MR due to SAM. These findings suggest the presence of LV systolic dysfunction and LV enlargement in patients with MR without SAM rather than in those with MR due to SAM. This finding is consistent with previous explanations for the etiology of ischemic MR.25–27 Our finding of simultaneous improvement of mitral valve tethering and MR severity in patients with TTC is particularly important for the understanding of the mechanism of acute MR. Of note, another study suggested papillary muscle dysfunction or displacement as a potential cause of MR in patients with TTC without any quantitative data.8 Clinical Implication The present study observations imply that TTC should be kept in mind as a potential cause of acute MR. Early detection is important for proper management of patients with this condition. Recognition of the difference in mitral geometry gives new insight into the mechanisms of acute MR in TTC. The current American College of Cardiology/American Heart Izumo et al Association guidelines recommend mitral valve surgery in symptomatic patients with severe acute MR28; however, our results support the idea that aggressive medical treatment of TTC would be the first priority because acute MR in TTC is reversible. Study Limitations Because this study was retrospective, the timing of follow-up echocardiography varied. However, LV function and wall motion and MR were improved at follow-up as expected. The logistic regressions are not necessarily representative of the population given the relatively low number of subjects versus the number of predictors. We could not conduct a large-scale study because of the low prevalence of the condition. Further prospective investigation with a larger population is warranted. Downloaded from http://circimaging.ahajournals.org/ by guest on May 10, 2017 Conclusions SAM and tethering of the mitral valve are independent mechanisms with differing pathophysiology that can lead to acute MR in patients with TTC. These findings imply that echocardiography should be performed systematically in patients with TTC to identify whether MR is present as well as to assess its mechanism. Acknowledgments We would like to thank Dr. and Mrs. Paul I. Terasaki for their kind support and encouragement. Disclosures None. References 1. Akashi YJ, Goldstein DS, Barbaro G, Ueyama T. Takotsubo cardiomyopathy: a new form of acute, reversible heart failure. Circulation. 2008; 118:2754 –2762. 2. Tsuchihashi K, Ueshima K, Uchida T, Oh-mura N, Kimura K, Owa M, Yoshiyama M, Miyazaki S, Haze K, Ogawa H, Honda T, Hase M, Kai R, Morii I; Angina Pectoris-Myocardial Infarction Investigations in Japan. Transient left ventricular apical ballooning without coronary artery stenosis: a novel heart syndrome mimicking acute myocardial infarction. J Am Coll Cardiol. 2001;38:11–18. 3. Kurisu S, Sato H, Kawagoe T, Ishihara M, Shimatani Y, Nishioka K, Kono Y, Umemura T, Nakamura S. Tako-tsubo-like left ventricular dysfunction with ST-segment elevation: a novel cardiac syndrome mimicking acute myocardial infarction. Am Heart J. 2002;143: 448 – 455. 4. Sharkey SW, Lesser JR, Zenovich AG, Maron MS, Lindberg J, Longe TF, Maron BJ. Acute and reversible cardiomyopathy provoked by stress in women from the United States. Circulation. 2005;111: 472– 479. 5. Akashi YJ, Tejima T, Sakurada H, Matsuda H, Suzuki K, Kawasaki K, Tsuchiya K, Hashimoto N, Musha H, Sakakibara M, Nakazawa K, Miyake F. Left ventricular rupture associated with Takotsubo cardiomyopathy. Mayo Clin Proc. 2004;79:821– 824. 6. Vidi V, Rajesh V, Singh PP, Mukherjee JT, Lago RM, Venesy DM, Waxman S, Pyne CT, Piemonte TC, Gossman DE, Nesto RW. Clinical characteristics of tako-tsubo cardiomyopathy. Am J Cardiol. 2009;104: 578 –582. 7. Parodi G, Del Pace S, Salvadori C, Carrabba N, Olivotto I, Gensini GF; Tuscany Registry of Tako-Tsubo Cardiomyopathy. Left ventricular apical ballooning syndrome as a novel cause of acute mitral regurgitation. J Am Coll Cardiol. 2007;50:647– 649. Acute MR in Takotsubo Cardiomyopathy 397 8. Haghi D, Röhm S, Suselbeck T, Borggrefe M, Papavassiliu T. Incidence and clinical significance of mitral regurgitation in Takotsubo cardiomyopathy. Clin Res Cardiol. 2010;99:93–98. 9. Prasad A, Lerman A, Rihal CS. Apical ballooning syndrome (Tako-Tsubo or stress cardiomyopathy): a mimic of acute myocardial infarction. Am Heart J. 2008;155:408 – 417. 10. Schiller NB, Shah PM, Crawford M, DeMaria A, Devereux R, Feigenbaum H, Gutgesell H, Reichek N, Sahn D, Schnittger I. Recommendations for quantitation of the left ventricle by two-dimensional echocardiography. American Society of Echocardiography Committee on Standards, Subcommittee on Quantitation of Two-Dimensional Echocardiograms. J Am Soc Echocardiogr. 1989;2:358 –367. 11. Piérard LA, Lancellotti P. The role of ischemic mitral regurgitation in the pathogenesis of acute pulmonary edema. N Engl J Med. 2004;351: 1627–1634. 12. Boltwood CM, Tei C, Wong M, Shah PM. Quantitative echocardiography of the mitral complex in dilated cardiomyopathy: the mechanism of functional mitral regurgitation. Circulation. 1983;68:498 –508. 13. Zoghbi WA, Enriquez-Sarano M, Foster E, Grayburn PA, Kraft CD, Levine RA, Nihoyannopoulos P, Otto CM, Quinones MA, Rakowski H, Stewart WJ, Waggoner A, Weissman NJ. Recommendations for evaluation of the severity of native valvular regurgitation with twodimensional and Doppler echocardiography. J Am Soc Echocardiogr. 2003;16:777– 802. 14. Yock PG, Popp RL. Noninvasive estimation of right ventricular systolic pressure by Doppler ultrasound in patients with tricuspid regurgitation. Circulation. 1984;70:657– 662. 15. Rudski LG, Lai WW, Afilalo J, Hua L, Handschumacher MD, Chandrasekaran K, Solomon SD, Louie EK, Schiller NB. Guidelines for the echocardiographic assessment of the right heart in adults: a report from the American Society of Echocardiography endorsed by the European Association of Echocardiography, a registered branch of the European Society of Cardiology, and the Canadian Society of Echocardiography. J Am Soc Echocardiogr. 2010;23:685–713. 16. Bland JM, Altman DG. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet. 1986;1:307–310. 17. Gianni M, Dentali F, Grandi AM, Sumner G, Hiralal R, Lonn E. Apical ballooning syndrome or takotsubo cardiomyopathy: a systematic review. Eur Heart J. 2006;27:1523–1529. 18. Song BG, Park SJ, Noh HJ, Jo HC, Choi JO, Lee SC, Park SW, Jeon ES, Kim DK, Oh JK. Clinical characteristics, and laboratory and echocardiographic findings in takotsubo cardiomyopathy presenting as cardiogenic shock. J Crit Care. 2010;25:329 –335. 19. Akashi YJ, Musha H, Kida K, Itoh K, Inoue K, Kawasaki K, Hashimoto N, Miyake F. Reversible ventricular dysfunction takotsubo cardiomyopathy. Eur J Heart Fail. 2005;7:1171–1176. 20. El Mahmoud R, Mansencal N, Pilliére R, Leyer F, Abbou N, Michaud P, Nallet O, Digne F, Lacombe P, Cattan S, Dubourg O. Prevalence and characteristics of left ventricular outflow tract obstruction in Tako-Tsubo syndrome. Am Heart J. 2008;156:543–548. 21. Schwammenthal E, Nakatani S, He S, Hopmeyer J, Sagie A, Weyman AE, Lever HM, Yoganathan AP, Thomas JD, Levine RA. Mechanism of mitral regurgitation in hypertrophic cardiomyopathy: mismatch of posterior to anterior leaflet length and mobility. Circulation. 1998;98: 856 –565. 22. Maron MS, Olivotto I, Zenovich AG, Link MS, Pandian NG, Kuvin JT, Nistri S, Cecchi F, Udelson JE, Maron BJ. Hypertrophic cardiomyopathy is predominantly a disease of left ventricular outflow tract obstruction. Circulation. 2006;114:2232–2239. 23. Chandrasegaram MD, Celermajer DS, Wilson MK. Apical ballooning syndrome complicated by acute severe mitral regurgitation with left ventricular outflow obstruction— case report. Cardiothorac Surg. 2007;2:14. 24. Brunetti ND, Ieva R, Rossi G, Barone N, De Gennaro L, Pellegrino PL, Mavilio G, Cuculo A, Di Biase M. Ventricular outflow tract obstruction, systolic anterior motion and acute mitral regurgitation in Tako-Tsubo syndrome. Int J Cardiol. 2008;127:e152–157. 25. Otsuji Y, Handschumacher MD, Schwammenthal E, Jiang L, Song JK, Guerrero JL, Vlahakes GJ, Levine RA. Insights from three dimensional echocardiography into the mechanism of functional mitral regurgitation: direct in vivo demonstration of altered leaflet tethering geometry. Circulation. 1997;96:1999 –2008. 26. Kwan J, Shiota T, Agler DA, Popović ZB, Qin JX, Gillinov MA, Stewart WJ, Cosgrove DM, McCarthy PM, Thomas JD. Geometric differences of the mitral apparatus between ischemic and dilated cardiomyopathy with 398 Circ Cardiovasc Imaging July 2011 significant mitral regurgitation: real-time three-dimensional echocardiography study. Circulation. 2003;107:1135–1140. 27. Marwick TH, Lancellotti P, Pierard L. Ischaemic mitral regurgitation: mechanisms and diagnosis. Heart. 2009;95:1711–1718. 28. ACC/AHA 2006 guidelines for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (writing committee to revise the 1998 Guidelines for the Management of Patients With Valvular Heart Disease): developed in collaboration with the Society of Cardiovascular Anesthesiologists: endorsed by the Society for Cardiovascular Angiography and Interventions and the Society of Thoracic Surgeons. Circulation. 2006;114:e84 –231. CLINICAL PERSPECTIVE Downloaded from http://circimaging.ahajournals.org/ by guest on May 10, 2017 Despite the favorable outcome of takotsubo cardiomyopathy (TTC) in general, the presence of significant acute mitral regurgitation (MR) increases the risks of acute deterioration and adverse outcome in TTC. However, the mechanism of acute MR in TTC remains unclear. In this study, we elucidated the mechanisms of acute MR in TTC; apical tethering and systolic anterior motion of the mitral valve are 2 independent mechanisms that can lead to acute MR in TTC. Our finding of simultaneous improvement of apical tethering and MR severity in the patients with TTC is particularly important for the understanding of the mechanism of acute MR. Based on the study results, TTC should be regarded as a potential cause of acute MR. In addition, pulmonary artery systolic pressure is significantly higher in patients with TTC with MR than in those without MR. Therefore, early detection of MR is important for proper management of patients with TTC. The current American College of Cardiology/American Heart Association guidelines recommend mitral valve surgery in symptomatic patients with severe acute MR; however, the present results support the idea that aggressive medical treatment of TTC would be the first priority because acute MR in TTC is reversible. These findings imply that echocardiography should be systematically performed in patients with TTC to identify MR and assess its mechanism. Mechanisms of Acute Mitral Regurgitation in Patients With Takotsubo Cardiomyopathy: An Echocardiographic Study Masaki Izumo, Smruti Nalawadi, Maiko Shiota, Jayanta Das, Suhail Dohad, Eiji Kuwahara, Yoko Fukuoka, Robert J. Siegel and Takahiro Shiota Downloaded from http://circimaging.ahajournals.org/ by guest on May 10, 2017 Circ Cardiovasc Imaging. 2011;4:392-398; originally published online April 15, 2011; doi: 10.1161/CIRCIMAGING.110.962845 Circulation: Cardiovascular Imaging is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Copyright © 2011 American Heart Association, Inc. All rights reserved. Print ISSN: 1941-9651. Online ISSN: 1942-0080 The online version of this article, along with updated information and services, is located on the World Wide Web at: http://circimaging.ahajournals.org/content/4/4/392 Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in Circulation: Cardiovascular Imaging can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for which permission is being requested is located, click Request Permissions in the middle column of the Web page under Services. Further information about this process is available in the Permissions and Rights Question and Answer document. Reprints: Information about reprints can be found online at: http://www.lww.com/reprints Subscriptions: Information about subscribing to Circulation: Cardiovascular Imaging is online at: http://circimaging.ahajournals.org//subscriptions/