Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Remote ischemic conditioning wikipedia , lookup
Electrocardiography wikipedia , lookup
Lutembacher's syndrome wikipedia , lookup
Coronary artery disease wikipedia , lookup
Mitral insufficiency wikipedia , lookup
Hypertrophic cardiomyopathy wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
Heart failure wikipedia , lookup
Cardiac surgery wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Jatene procedure wikipedia , lookup
Antihypertensive drug wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
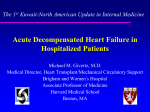
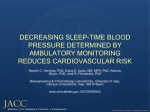
4/26/2016 Pharmacotherapy of the Critically Ill Patient ACUTE DECOMPENSATED HEART FAILURE Brent N. Reed, PharmD, BCPS-AQ Cardiology, FAHA Assistant Professor, Department of Pharmacy Practice and Science University of Maryland School of Pharmacy @brentnreed J Am Coll Cardiol 2013;62:e147-239. DEFINITIONS DEFINITIONS • Acute decompensated heart failure Emergence of new or worsening signs and/or symptoms of heart failure • Cardiogenic shock Heart failure with systemic hypoperfusion Heart Failure with Reduced Ejection Fraction (HFrEF) Heart Failure with Preserved Ejection Fraction (HFpEF) Impaired ejection of blood, formerly known as systolic dysfunction; ejection fraction < 40% Impaired filling of blood, formerly known as diastolic dysfunction; ejection fraction > 40-50% Muscle images from “Heart Failure”, Cleveland Clinic Center for Continuing Education. Heart image from Marieb & Hoehn. Anatomy & Physiology, 9e. Pearson, 2013.v DEFINITIONS EPIDEMIOLOGY OF HEART FAILURE • 5.7 million adults in the US have heart failure • Expected to increase by over half by year 2030 • Over 1 million are hospitalized annually • 1 in 4 are readmitted within 30 days Left Heart Failure Right Heart Failure Biventricular failure Circulation 2015;131(4):e29–322. 1 4/26/2016 DISEASE PROGRESSION PATHOPHYSIOLOGY Heart failure decompensations Venous Congestion Signs and symptoms of venous congestion, congestive end-organ dysfunction Myocardial Function Volume Overload Time Low Cardiac Output Both Adapted from Am J Cardiol. 2005 Sep 19;96(6A):11G-17G. PATHOPHYSIOLOGY PATHOPHYSIOLOGY Mean Arterial Pressure (MAP) Impaired organ function, signs and symptoms of decreased perfusion Volume Overload Low Cardiac Output Volume Overload Both Low Cardiac Output Both PRECIPITATING CAUSES QUESTION #1 • Nonadherence to medications or diet • Pulmonary embolus • Negative inotropes • Endocrine abnormalities List five (5) precipitating causes of acute decompensated heart failure (ADHF). What is the most likely cause in this patient? • Drugs that promote salt retention • Myocardial ischemia • High blood pressure • Arrhythmias • Alcohol or illicit drugs • Infections • Other acute cardiovascular disorders J Am Coll Cardiol. 2013 Oct 15;62(16):e147-239. 2 4/26/2016 THERAPEUTIC GOALS QUESTION #2 • Relieve symptoms What are the therapeutic goals for this patient’s ADHF? • Optimize volume status • Restore hemodynamic stability • Reduce inpatient mortality • Address reason(s) for decompensation • Minimize risk for rehospitalization PATIENT PRESENTATION Fluid Overload Low Cardiac Output • Dyspnea on exertion • Orthopnea • Paroxysmal nocturnal dyspnea • Crackles • S3 gallop • Early satiety • Jugular venous distention • Hepatojugular reflex • Ascites • Peripheral edema • • • • • • • Altered mental status Fatigue Cool extremities Narrow pulse pressure Hypotension Hyponatremia Evidence of impaired endorgan perfusion (renal, hepatic function) Chest x-ray showing significant pulmonary edema Same patient following diuresis (2 days later) University of Virginia Department of Radiology. Available from https://www.meded.virginia.edu/courses/rad/cxr/pathology2chest.html. Accessed 2015 Mar 05. CARDIAC OUTPUT HEMODYNAMIC MONITORING • Preload (volume) • Afterload (impedance) • Contractility (strength) Right Heart Catheterization (RHC) A pulmonary artery (PA) catheter (also known as a SwanGanz catheter) is advanced through the right side of the heart and into a small branch of the pulmonary artery Can obtain a pulmonary capillary wedge pressure (PCWP), which approximates left ventricular enddiastolic pressure (LVEDP), i.e., preload CO – cardiac output; HR – heart rate; SV – stroke volume 3 4/26/2016 PRELOAD VOLUME STATUS normal Cardiac Index (Stroke Volume) Cardiac Index (Stroke Volume) “Dry” “Wet” Shortness of breath Pulmonary congestion Peripheral edema Jugular venous distention (JVD) heart failure overload 8 – 12 Symptoms 18 18 PCWP or LVEDP PCWP or LVEDP mm Hg (Preload) mm Hg (Preload) AFTERLOAD CONTRACTILITY SVR Intrinsic strength of myocardial contraction dyne · s / cm5 (Afterload) Beta Receptor 900 – 1400 normal Cardiac Index (Stroke Volume) heart failure Angiotensin II Receptor Image from Circulation Research. 2011; 109: 217-230 . CONTRACTILITY CARDIAC OUTPUT SVR Can be impaired as a result of damage to myocardial cells. dyne · s / cm5 (Afterload) Remodeling 2.8 – 4.2 Chronic pathological changes to the structure and function of myocardial tissue (e.g., hypertension, neuro-hormonal mediators) Treatment Myocardial infarction Loss of coronary perfusion resulting in a localized zone of myocardial tissue damage Severe impairment may require inotropic drugs, mechanical circulatory support, or transplantation. Cardiac Index “Warm” 2.2 L/min/m2 “Cold” Symptoms Cold, clammy extremities Altered mental status PCWP or LVEDP (Preload) 4 4/26/2016 HEMODYNAMIC SUBSETS QUESTION #3 SVR (Afterload) Optimize chronic oral therapy Cardiac Index “Warm and Dry” “Warm and Wet” Diuretics +/adjunct therapies “Cold and Dry” “Cold and Wet” Diuretics +/vasodilators and/or inotropes Classify this patient into a hemodynamic subset. If a pulmonary artery catheter was inserted, what values for pulmonary capillary wedge pressure and cardiac index would you expect? 2.2 Vasodilators and/or inotropes 18 PCWP or LVEDP (Preload) MANAGING HOME MEDICATIONS IV LOOP DIURETICS I Medication Criteria for Discontinuation ACE inhibitor or ARB • Acute kidney injury unrelated to ADHF • Cardiogenic shock or hypotension • Severe hyperkalemia Beta blocker • ADHF due to initiation or dose increase • Cardiogenic shock or hypotension • Symptomatic bradycardia Aldosterone antagonist • Acute kidney injury unrelated to ADHF • Severe hyperkalemia Isosorbide dinitrate / hydralazine • Cardiogenic shock or hypotension Digoxin • Symptomatic bradycardia • Life-threatening arrhythmia • Elevated serum digoxin concentrations or signs/symptoms of toxicity ACE – angiotensin converting enzyme; ADHF – acute decompensated heart failure; ARB – angiotensin-receptor blocker III Fluid overload should be promptly treated with IV loop diuretics Advantages Disadvantages • Improvements in heart failure signs and symptoms • No improvements in longterm morbidity or mortality • Improvements in hemodynamics • Neurohormonal activation • Renal impairment • Electrolyte abnormalities QUESTION #4 Onset Duration IV Equivalence Bolus (min) IIb J Am Coll Cardiol 2013;62:e147-239. Eur J Heart Fail 2007;9:1064–1069. Ann Intern Med 1985;103:1–6. IV LOOP DIURETICS Agent IIa B Infusion (h) (mg) (mg) (mg/h) Furosemide 2-5 6 20-40 20-200 2.5-40 Torsemide < 10 6-12 20 10-100 2-10 Bumetanide 2-3 4-6 1 1-10 0.5 -2 Recommend an initial therapeutic regimen for this patient’s ADHF, including drug, dose, route, and frequency of administration. What are two parameters you would use to monitor efficacy? Safety? Adapted from Vardeny O, Ng TMH. Pharmacotherapy Principles & Practice. 2013:79-108. • For most patients: up to 2.5x outpatient dose (IVB or CI) • Signs of hypoperfusion: 1x outpatient dose (IVB or CI) • CI vs IVB: tenuous hemodynamics; diuretic resistance (?) 5 4/26/2016 Pharmacokinetic Mechanisms Pharmacodynamic Mechanisms Distal convoluted tubule Decreased gut absorption and/or renal perfusion OVERCOMING DIURETIC RESISTANCE Compensatory sodium reabsorption Glomerulus Proximal convoluted tubule Ultrafiltration or Vasopressin Antagonist (select patients only) Remodeling of the nephron Collecting duct Reninangiotensinaldosterone system Add Targeted Therapies Enhance Blood Flow Arginine vasopressin Loop of Henle Intravenous Vasodilator or Inotrope (refractory patients or those with low cardiac output) Neurohormonal activation Common Mechanisms of Diuretic Resistance Augment Diuresis Change Diuretic Strategy or Add an Alternative Diuretic (most patients exhibiting diuretic resistance) Nephron diagram from: OpenStax College. Anatomy & Physiology [Connexions Web site]. January 3, 2014. Available at: http://cnx.org/content/col11496/1.6/. CHANGING DIURETIC STRATEGY I Effective diuresis Normal Heart Failure IIb III If initial diuresis is inadequate, regimen may be intensified by adding a second diuretic Dose Route Initial (mg) Agent Higher doses required for diuretic effect IIa IIb III B If initial diuresis is inadequate, regimen may be intensified by increasing the dose Convert to a continuous infusion? Image adapted from Cardiology. 96;2001:132-143. J Am Coll Cardiol 2013;62:e147-239. IV VASODILATORS Venous Vasodilation • Mobilizes fluid in periphery • Decongests kidneys Nitroglycerin* Sodium Nitroprusside Nesiritide I IIa B Diminished maximal diuretic response Diuretic Concentration I DIURETIC SYNERGY IIa IIb A III Max Dose* Duration 6-12 (mg) (h) Chlorothiazide IV 250 – 500 1000 Hydrochlorothiazide PO 25 – 50 200 6-12 Metolazone PO 2.5 20 12-24 * Doses may be divided twice daily. • Not required to administer 30 minutes prior to loop diuretic • Enhanced diuresis may increase risk of adverse effects J Am Coll Cardiol 2013;62:e147-239. LOW-DOSE DOPAMINE Arterial Vasodilation • Improved renal blood flow due to reduced impedance Sodium Nitroprusside Nesiritide Selective renal vasodilation* I In absence of hypotension, IV vasodilators may be used as an adjuvant to diuretics *At high-doses (> 100 mcg/min), nitroglycerin exerts venous and arterial dilating effects. J Am Coll Cardiol 2013;62:e147-239. Kidney image from Marieb & Hoehn. Anatomy & Physiology, 9e. IIa IIb B III Low-dose dopamine may be considered in addition to loop diuretic therapy *Like centaurs, this too is a myth. 6 4/26/2016 QUESTION #5 VASOPRESSIN ANTAGONISTS Although the patient responds initially, his symptoms persist. He remains warm and wellperfused with a blood pressure of 118/82 mmHg. What modifications would you make to his regimen? If you add another drug, provide a dose, route, and frequency of administration, as well as two parameters each for safety and efficacy. • Arterial under-filling stimulates AVP release Tolvaptan • Hyponatremia linked to poor outcomes in ADHF • Vasopressin antagonists, such as tolvaptan, improve serum sodium concentrations and some ADHF symptoms • No improvements in long-term outcomes Vasopressin antagonists bind to V2 receptors to prevent aquaporin synthesis. AVP – arginine vasopressin Arch Intern Med 2007;167:1998-2005. Image from Circulation. 2008 Jul 22;118(4):410-21. SALT-1* 140 Tolvaptan 135 130 Placebo 0 10 20 30 40 Day I IIa IIb III B Serum Sodium (mmol/L) Serum Sodium (mmol/L) VASOPRESSIN ANTAGONISTS ULTRAFILTRATION VS. HEMODIALYSIS SALT-2* 140 Tolvaptan Ultrafiltration 135 High Pressure 130 Low Pressure Hemodialysis High Concentration Low Concentration Placebo 0 10 20 30 40 Day Short-term vasopressin antagonist use may be considered in patients with volume overload and severe hyponatremia or those at-risk for cognitive symptoms *Vertical dotted lines indicate the end of the treatment period. Images adapted from N Engl J Med 2006;355:2099-112. J Am Coll Cardiol 2013;62:e147-239. Fluid crosses semipermeable membrane due to pressure differences; No solute removal Fluid and solutes cross semipermeable membrane due to concentration differences Venous system image from Marieb & Hoehn. Anatomy & Physiology, 9e. Pearson, 2013.v ULTRAFILTRATION QUESTION #6 • Isotonic rather than hypotonic fluid removal What is the role of ultrafiltration in patients with ADHF? How is it similar to conventional hemodialysis? How is it different? Should it be considered at this time? • Enhances volume removal and weight loss • Worsens existing renal impairment and increases adverse effects vs. pharmacologic therapy • Should not be used to avoid vasoactive drugs • Must balance with cost, need for venovenous access I IIa IIb B/C III Ultrafiltration may be considered for obvious fluid overload (B), or refractory congestion unresponsive to medical therapy (C) J Am Coll Cardiol 2007;49:675-83. N Engl J Med 2012;367:2296-304. J Am Coll Cardiol 2013;62:e147-239. 7 4/26/2016 LOW CARDIAC OUTPUT INTRAVENOUS VASODILATORS Low CO No Agent Dilation Dosing Nesiritide Arterial, Venous 2 mcg/kg bolus, 0.01 mcg/kg/min Norepinephrine Dopamine Nitroglycerin Venous > Arterial 5–200 mcg/min • High doses required for arterial vasodilation • Tachyphylaxis IV Inotropes Sodium Nitroprusside Arterial, Venous 0.3–3 mcg/kg/min • Accumulation of toxic metabolites in hepatic, renal impairment Optimize chronic medications < 2.2 L/min/m2 Yes Adequate MAP Fluids, Inopressors No (> 50 mm Hg) Yes Adequate SBP IV Vasodilators Nesiritide Nitroglycerin Sodium Nitroprusside Yes (SBP > 90 mmHg, absence of symptomatic hypotension, stable renal function) No Dobutamine Milrinone Adapted from DiPiro JT, et al (eds). Pharmacotherapy: A pathophysiological approach, 9th edition. New York: McGraw-Hill; 2014. INTRAVENOUS INOTROPES Agent Dose CO HR SVR 2.5–5 5–20 5–10 10–20 Milrinone 0.1–0.75 Norepinephrine 0.01–3* / Dobutamine Dopamine (mcg/kg/min) • Favored over inotropes given fewer adverse outcomes • Class disadvantages: hypotension, ± invasive monitoring J Am Coll Cardiol 2013;62:e147-239. J Am Coll Cardiol. 2005; 46: 57–64. INTRAVENOUS INOTROPES t½ (min) Considerations 2 – 10 Blood pressure response varies 2 – 10 Lower doses not renoprotective 60-120 Undergoes renal clearance / 1-2 Use only in low blood pressure I IIa IIb III Until definitive therapy or resolution of the acute precipitating problem, patients with cardiogenic shock should receive intravenous inotropic support IIa IIb III Short-term inotropic support may be reasonable in the setting of low blood pressure and low cardiac output III Use of intravenous inotropes in the absence of impaired perfusion and low cardiac output is potentially harmful C I B I IIa IIb B • Consider only for those with evidence of low output • Increased risk of tachyarrhythmia, mortality Beta Blocker Pharmacologic Effects Chronic Changes to Receptor Profile Metoprolol Inhibits β1 >> β2 receptors Up-regulation of β receptors; improved G-protein coupling Inhibits α1, β1, and β2 receptors Diminished effects at α1; no change in β1, β2 expression BETA BLOCKERS & INOTROPES Parameter Dobutamine BETA BLOCKERS & INOTROPES J Am Coll Cardiol 2013;62:e147-239. Milrinone* *Commonly dosed in mcg/min (1-20). J Am Coll Cardiol 2013;62:e147-239. Carvedilol Disadvantages • 20-minute half-life • High cost Baseline Metoprolol Carvedilol CI (L/min/m2) / PCWP (mmHg) SVR (dyn s/cm5) / MAP (mmHg) HR (bpm) / CI (L/min/m2) PCWP (mmHg) SVR (dyn s/cm5) MAP (mmHg) HR (bpm) CI – cardiac index; HR – heart rate; MAP – mean arterial pressure; PCWP – pulmonary capillary wedge pressure; SVR – systemic vascular resistance. *Original study used enoximone J Am Coll Cardiol 2002;40:1248–58. 8 4/26/2016 QUESTION #7 REFRACTORY HEART FAILURE The patient’s condition worsens. He endorses cold extremities and weak distal pulses with a blood pressure of 92/62 mmHg. His serum creatinine has risen to 2.6 mg/dL and pulmonary artery catheterization reveals a cardiac index of 1.6 L/min/m2. Provide a recommendation for drug therapy, including drug, dose, route, and frequency of administration. Why did you select this agent? Name two monitoring parameters each for efficacy and safety. Despite your best efforts, the patient’s condition continues to deteriorate. Your team consults an interventionalist and cardiac surgeon to determine the best course of action. MECHANICAL CIRCULATORY SUPPORT IIa I IIb III B Percutaneous Mechanical Circulatory Support Intra-aortic balloon pump Impella® TandemHeart® ECMO Temporary MCS may be considered as a bridge to recovery or decision in carefully selected patients with acute, profound hemodynamic compromise • Cardiogenic shock (e.g., MI, ADHF, graft rejection) • Cardiovascular intervention in high-risk patients • Bridge to durable MCS or transplantation • Right ventricular failure ADHF – acute decompensated heart failure; MCS – mechanical circulatory support; MI – myocardial infarction; J Am Coll Cardiol 2013;62:e147-239. Surgical Mechanical Circulatory Support CentriMag® ECMO – extracorporeal membrane oxygenation; Adapted from Eur Heart J. 2014 Jan;35(3):156-67 INTRA-AORTIC BALLOON PUMP Diastolic Phase The balloon inflates during diastole, which increases diastolic pressure thereby enhancing coronary perfusion Ao PA RA LV Can provide left ventricular, right ventricular, or biventricular support (biventricular configuration shown) Ao – aorta; LV – left ventricle; PA – pulmonary artery; RA – right atrium Intra-Aortic Balloon Pump Control • Trigger for each cycle (pressure, ECG) • Augmentation (balloon inflation) • Frequency (1:1, 1:2, or 1:3 cardiac cycles) • Various other parameters To device console 9 4/26/2016 INTRA-AORTIC BALLOON PUMP Systolic Phase The balloon deflates during systole; resulting vacuum-like effect reduces aortic pressure, thereby reducing left ventricular afterload Intra-Aortic Balloon Pump Control • Trigger for each cycle (pressure, ECG) • Augmentation (balloon inflation) • Frequency (1:1, 1:2, or 1:3 cardiac cycles) • Various other parameters To device console CLINICAL CONSIDERATIONS Contraindications* Complications Neurologic devastation Peripheral vascular disease Sepsis/systemic infection Bleeding diatheses Ventricular septal defect (TandemHeart®) • Aortic disease (IABP, Impella®) • • • • • • • • • • • • • • • Thrombosis Bleeding Infection Arrhythmias Malposition Vascular/tissue damage Neurologic complications Perforation (TandemHeart®) Hemolysis (Impella®) Thrombocytopenia (IABP) *Generally considered relative contraindications; differs by device Crit Care Med. 2014 Jan;42(1):158-68 QUESTION #8 Describe how an intra-aortic balloon pump provides hemodynamic support in patients with cardiogenic shock. Pharmacotherapy of the Critically Ill Patient ACUTE DECOMPENSATED HEART FAILURE Brent N. Reed, PharmD, BCPS-AQ Cardiology, FAHA Assistant Professor, Department of Pharmacy Practice and Science University of Maryland School of Pharmacy @brentnreed 10