Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
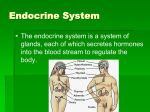
Basic Mechanism of Endocrine Disorders Qi Hongyan Content Describe the endocrine system and the process of negative feedback in regulation of hormones production and secretion. Discuss the pathogenesis of hyperthyroidism, hypothyroidism and diabetes mellitus. Endocrine System Endocrine system uses chemical substances called Hormone as a means of regulating and integrating body functions. It participates in the regulation of digestion, use, and storage of nutrients; growth and development; electrolyte and water metabolism; and reproductive functions. Endocrine System Regulation of endocrine system Nerve system Immuno system Endocrine system Historical retrospect 1、Gland Endocrinology ( 1850-1950) 2、Tissue Endocrinology 1950- 3、Molecular Endocrinology Hormones Hormones generally are thought of as chmical messengers that are transported in body fluids. They are highly specialized organic molecules produced by endocrine organs that exert their action on specific target cells. Classifications of Hormones Steroid hormones : estrogen, androstenedione, testosterone… Peptides or proteins : PTH, insulin, oxytocin, GH, FSH, ACTH… Amine and amino acids derivatives: TH, dopanime… Relationship of free and carrier-bound hormones Endocrine cell Free hormone Hormone receptor Biological effects Carrier-bound hormone Activation mechanism of Hormones Carol mattson porth Pathophysiology 7th edition Activation mechanism of Hormones Carol mattson porth Pathophysiology 7th edition Hypothalamus and hypophysis Thyrotropin releasing hormone (TRH) Corticotropin releasing hormone (CRH) Growth hormone releasing hormone (GHRH) Somatostatin as inhibiting hormone (e.g. GH) Gonadotropin releasing hormone (GnRH) Hypothalamus and hypophysis Pituitary gland (Hypophysis) Anterior lobe (Adenohypophysis) Glandular cells (originate from Rathke’s pouch) Secretes six important peptide hormones Posterior lobe (Neurohypophysis) Glial-type cells (neural origin) Secretes two important peptide hormones Hormones of hypophysis Adenohypophysis Somatotropes – human growth hormone (hGH) Corticotropes – adrenocorticotropin (ACTH) Thyrotropes – Thyroid stimulating hormone (TSH) Gonadotropes – gonadotropic hormones Luteinizing hormone (LH) Follicle stimulating hormone (FSH) Lactotropes – prolactin (PRL) Neurohypophysis Antidiuretic hormone(ADH) oxytocin Regulation of endocrine system Hypothalamus Hypophysis TRH TSH Gland Thyroid Hormone T3/T4 CRH ACTH Adrenal cortisol GHRH/GIH GH GnRH FSH/LH Ovarian Testis E2、AD、 Testosterone DA PRL ADH OXYTOCIN Regulation of endocrine system - Hypothalamus - + Pituitary + Endocrine glands + Hormone - Endocrine Dysfunction • Hypofunction: defects of gland, defects of enzyme for the hormone synthesis, inflammation, neoplastic growth, defects of receptor… • Hyperfunction: excessive hormone production •Primary:defects of target gland responsible for producing the hormone •Secondary:alteration of regulation for producing the hormone •Tertiary:hypotalamic dysfunction Regulation of cortisol secretion Hypothalamus (CRH) regulates the secretion of ACTH secretion, which increases in stress ACTH acts through the second messenger cAMP It controls the rate limiting step of converting cholesterol to pregnenolone Circadian rhythm – more in early morning & low in midnight Hyperadrenalism – Cushing’s syndrome Mobilization of fat from lower parts of body & extra deposition in upper portions – buffalo torso Moon face Striae – due to tearing of subcutaneous tissue, by diminished collagen fibers Increased blood glucose level Muscle weakness Loss of protein synthesis in lymphoid tissue suppresses immune system Hyperadrenalism – Cushing’s syndrome Regulation of GH secretion Carol mattson porth Pathophysiology 7th edition Growth hormone Control of GH Stress, exercise nutrition, sleep Somatostatin (SS) inhibits GH causes inhibition of glucose uptake and utilization, increased a.a. uptake and protein synthesis Robert Wardlow 8’ 11”. Gigantism Excessive GH during childhood Growth plate stimulation Tumor of somatotrophs Abnormalities of GH secretion Gigantism Acromegaly GH late in life Causes excessive growth of flat bones Rondo Hatton Abnormalities of GH secretion Acromegaly GH deficiency: nanism NEUROHYPOPHYSIS ADH or vasopressin Supraoptic nucleus Increased water reabsorption in kidney Vasoconstriction in high dose Thyroid Function and Disease Anatomy of the Thyroid Gland Follicles: the Functional Units of the Thyroid Gland Follicles Are the Sites Where Key Thyroid Elements Function: • Thyroglobulin (Tg) • Tyrosine • Iodine • Thyroxine (T4) • Triiodotyrosine (T3) The Thyroid Produces and Secretes 2 Metabolic Hormones Two principal hormones Thyroxine (T4 ) and triiodothyronine (T3) • Required for homeostasis of all cells • Influence cell differentiation, growth, and metabolism • Considered the major metabolic hormones because they target virtually every tissue Thyroid-Stimulating Hormone (TSH) Regulates thyroid hormone production, secretion, and thyroid growth Is regulated by the negative feedback action of T4 and T3 Biosynthesis of T4 and T3 The process includes Dietary iodine (I) ingestion Active transport and uptake of iodide (I-) by thyroid gland Oxidation of I- and iodination of thyroglobulin (Tg) tyrosine residues Coupling of iodotyrosine residues (MIT and DIT) to form T4 and T3 Proteolysis of Tg with release of T4 and T3 into the circulation Iodine Sources Available through certain foods (eg, seafood), iodized salt, or dietary supplements, as a trace mineral The recommended minimum intake is 150 g/day Active Transport and I- Uptake by the Thyroid Dietary iodine reaches the circulation as iodide anion (I-) The thyroid gland transports I- to the sites of hormone synthesis I- accumulation in the thyroid is an active transport process that is stimulated by TSH Oxidation of I- and Iodination of Thyroglobulin (Tg) Tyrosyl Residues I- must be oxidized to be able to iodinate tyrosyl residues of Tg Iodination of the tyrosyl residues then forms monoiodotyrosine (MIT) and diiodotyrosine (DIT), which are then coupled to form either T3 or T4 Both reactions are catalyzed by TPO Thyroperoxidase (TPO) TPO catalyzes the oxidation steps involved in I- activation, iodination of Tg tyrosyl residues, and coupling of iodotyrosyl residues TPO has binding sites for I- and tyrosine TPO uses H2O2 as the oxidant to activate I- to hypoiodate (OI-), the iodinating species T4: A Prohormone for T3 T4 is biologically inactive in target tissues until converted to T3 Activation occurs with 5' deiodination of the outer ring of T4 T3 then becomes the biologically active hormone responsible for the majority of thyroid hormone effects Carriers for Circulating Thyroid Hormones More than 99% of circulating T4 and T3 is bound to plasma carrier proteins Thyroxine-binding globulin (TBG), binds about 75% Transthyretin (TTR), also called thyroxine-binding prealbumin (TBPA), binds about 10%-15% Albumin binds about 7% High-density lipoproteins (HDL), binds about 3% Carrier proteins can be affected by physiologic changes, drugs, and disease Free Hormone Concept Only unbound (free) hormone has metabolic activity and physiologic effects Free hormone is a percentage of total hormone in plasma (about 0.03% T4; 0.3% T3) Total hormone concentration Normally is kept proportional to the concentration of carrier proteins Is kept appropriate to maintain a constant free hormone level TR ch 17 TR ch 3 Distribution of TH receptors SNC: TRß1 e TRß2 + TR1 TR2 Hypothalamus- hypophysis: TRß1 e TRß2 Heart: TRß1 e TRß2 + TR1 Liver: TRß1 e TRß2 Kindy: TR1 + TRß1 e TRß2 Gonad: TR1 Muscle: TR1 Biological Role of Thyroid Hormones (THs) • THs initiate or sustain differentiation and growth, they are essential for childhood growth and for neural development and maturation and function of the CNS • THs stimulate oxygen consumption by mitochondria, mitochondrial protein synthesis and mitochondrogenesis THs stimulate Metabolic Activities in Most Tissues exerting calorigenic effetcs, stimulate lypolisis and metabolism of cholesterol THs Influences Cardiovascular Hemodynamics THs influence the Female Reproductive System Thyroid Hormone Plays a Major Role in Growth and Development Thyroid hormone initiates or sustains differentiation and growth Stimulates formation of proteins, which exert trophic effects on tissues Is essential for normal brain development Essential for childhood growth Untreated congenital hypothyroidism or chronic hypothyroidism during childhood can result in incomplete development and mental retardation Thyroid Hormones and the Central Nervous System (CNS) Thyroid hormones are essential for neural development and maturation and function of the CNS Decreased thyroid hormone concentrations may lead to alterations in cognitive function Patients with hypothyroidism may develop impairment of attention, slowed motor function, and poor memory Thyroid-replacement therapy may improve cognitive function when hypothyroidism is present Thyroid Hormone Influences Cardiovascular Hemodynamics Thyroid hormone Mediated Thermogenesis (Peripheral Tissues) Release Metabolic Endproducts T3 Elevated Blood Volume Increased Cardiac Output Cardiac Chronotropy and Inotropy Local Vasodilatation Decreased Systemic Vascular Resistance Decreased Diastolic Blood Pressure Laragh JH, et al. Endocrine Mechanisms in Hypertension. Vol. 2. New York, NY: Raven Press;1989. Thyroid Hormone Influences the Female Reproductive System Normal thyroid hormone function is important for reproductive function Hypothyroidism may be associated with menstrual disorders, infertility, risk of miscarriage, and other complications of pregnancy Doufas AG, et al. Ann N Y Acad Sci. 2000;900:65-76. Glinoer D. Trends Endocrinol Metab. 1998; 9:403-411. Glinoer D. Endocr Rev. 1997;18:404-433. Thyroid Hormone is Critical for Normal Bone Growth and Development T3 is an important regulator of skeletal maturation at the growth plate T3 regulates the expression of factors and other contributors to linear growth directly in the growth plate T3 also may participate in osteoblast differentiation and proliferation, and chondrocyte maturation leading to bone ossification Thyroid Hormones Stimulate Metabolic Activities in Most Tissues Thyroid hormones (specifically T3) regulate rate of overall body metabolism T3 increases basal metabolic rate Calorigenic effects T3 increases oxygen consumption by most peripheral tissues Increases body heat production Metabolic Effects of T3 Stimulates lipolysis and release of free fatty acids and glycerol Stimulates metabolism of cholesterol to bile acids Facilitates rapid removal of LDL from plasma Generally stimulates all aspects of carbohydrate metabolism and the pathway for protein degradation Overview of Thyroid Disease States Hypothyroidism Hyperthyroidism Overview of Thyroid Disease States Euthyroidism Primary Hypothyroidism Primary Hyperthyroidism hypothalamus hypothalamus hypothalamus hypophysis hypophysis hypophysis thyroid thyroid thyroid Hypothyroidism Hypothyroidism is a disorder with multiple causes in which the thyroid fails to secrete an adequate amount of thyroid hormone The most common thyroid disorder Usually caused by primary thyroid gland failure Also may result from diminished stimulation of the thyroid gland by TSH Hypothyroidism: Types Primary hypothyroidism From thyroid destruction Central or secondary hypothyroidism From deficient TSH secretion, generally due to sellar lesions such as pituitary tumor or craniopharyngioma Infrequently is congenital Central or tertiary hypothyroidism From deficient TSH stimulation above level of pituitary—ie, lesions of pituitary stalk or hypothalamus Is much less common than secondary hypothyroidism Bravernan LE, Utiger RE, eds. Werner & Ingbar's The Thyroid. 8th ed. Philadelphia, Pa: Lippincott Williams & Wilkins; 2000. Persani L, et al. J Clin Endocrinol Metab. 2000; 85:3631-3635. Primary Hypothyroidism: Underlying Causes Congenital hypothyroidism Agenesis of thyroid Defective thyroid hormone biosynthesis due to enzymatic defect Thyroid tissue destruction as a result of Chronic autoimmune (Hashimoto) thyroiditis Radiation (usually radioactive iodine treatment for thyrotoxicosis) Thyroidectomy Other infiltrative diseases of thyroid (eg, hemochromatosis) Drugs with antithyroid actions (eg, lithium, radiographic contrast agents, interferon alpha) HYPOTHYROIDISM Hyperthyroidism Hyperthyroidism refers to excess synthesis and secretion of thyroid hormones by the thyroid gland, which results in accelerated metabolism in peripheral tissues Hyperthyroidism Underlying Causes Signs and symptoms can be caused by any disorder that results in an increase in circulation of thyroid hormone Toxic diffuse goiter (Graves disease) Toxic uninodular or multinodular goiter Painful subacute thyroiditis Silent thyroiditis Toxic adenoma Iodine and iodine-containing drugs and radiographic contrast agents Trophoblastic disease, including hydatidiform mole Exogenous thyroid hormone ingestion Graves Disease The most common cause of hyperthyroidism Accounts for 60% to 90% of cases Affects more females than males, especially in the reproductive age range Graves disease is an autoimmune disorder possibly related to a defect in immune tolerance Pathogenesis Graves ophthalmopethy 5-10% of patients without ipertiroidismo 50-75% of patients associated with ipertiroidismo, Graves ophthalmopethy Graves Disease T3 Na/K-ATP酶 UCP Producing Calorie Reduce body weight metabolism Nerves Cardiovascular gastro digestion Thyroid dysfunction Thyroid Carcinoma Incidence Thyroid carcinoma occurs relatively infrequently compared to the common occurrence of benign thyroid disease Thyroid cancers account for only 1% of cancers The annual rate has increased nearly 11 new cases/year/100000 Mortality is 0,4-0,8/100000 inn men and women, respectively Thyroid carcinomas Papillary (80%) Follicular (about 10%) Medullary thyroid (5%-10%) Anaplastic carcinoma (1%-2%) Primary thyroid lymphomas (rare) Metastatic from other primary sites (rare) Molecular mechanism in papillary thyroid carcinoma PC 40% N 15% FC PC PC 20% AC Diabetes mellitus PANCREATIC ISLET Alpha cells (25%) Glucagon Beta cells (60%) Insulin & amylin Delta cells (10%) Somatostatin Control of insulin secretion Increased blood glucose stimulates insulin secretion Some amino acids (arginine & lysine) when present along with ↑ glucose stimulates insulin secretion Hormones like glucagon, GH, cortisol etc act directly or indirectly to ↑ insulin secretion Insulin and glucagon Carol mattson porth Pathophysiology 7th edition FUNCTION OF INSULIN Insulin being an anabolic hormone stimulates protein & fatty acids synthesis. Insulin decreases blood sugar 1. By inhibiting hepatic glycogenolysis and gluconeogenesis. 2. By stimulating glucose uptake, utilization & storage by the liver, muscles & adipose tissue. Metabolic effects of Insulin Effect of insulin on carbohydrate metabolism Insulin promotes glucose uptake & metabolism in muscle cells, adipose tissues etc. by translocating the GLUT Insulin promotes glucose uptake & storage in liver Insulin inactivates liver phosphorylase which prevents glycogen break down It ↑ activity of glucokinase, causing the phosphorylation of glucose & then glucose get trapped inside It ↑ activity of enzymes for glycogen synthesis (glycogen synthase) Insulin promotes conversion of excess glucose into fatty acids & inhibits gluconeogenesis in liver The brain cells are permeable to glucose & can use glucose without the intermediation of insulin Effect of insulin on fat metabolism Since insulin ↑ utilization of glucose by most cells, causes ↓ utilization of fat, leading to fat storage In liver cells excess glycogen prevents the further formation of glycogen & the glucose thus entering gets converted to pyruvate by glycolysis & forms the acetyl CoA which leads to the formation of fatty acids On adipose tissue insulin inhibits the action of lipases, preventing the hydrolysis of fats Glucose entered into adipose tissue gets converted to α–glycerol phosphate, which helps in the formation of triglycerides & thus the storage of fat. Effect of insulin on protein metabolism & growth Insulin promotes protein synthesis & storage. It inhibits the catabolism of proteins Insulin stimulates transport of many of the amino acids (especially valine, leucine, isoleucine, tyrosine, & phenylalanine) into the cells Insulin & growth hormone interact synergistically to promote growth – GH also cause the uptake of amino acids, but a different selection as from that of insulin DEFINITION The term diabetes mellitus describes a metabolic disorder of multiple etiologies characterized by chronic hyperglycemia with disturbances of carbohydrate, fat and protein metabolism resulting from defects of insulin secretion, insulin action or both. DIABETES EPIDEMIOLOGY Diabetes is the most common endocrine problem & is a major health hazard worldwide. Incidence of diabetes is alarmingly increasing all over the globe. 5% of the general population are diagnosed with diabetes. WHO CLASSIFICATION 2000 Is based on etiology not on type of treatment or age of the patient. Type 1 Diabetes (idiopathic or autoimmune -cell destruction) Type 2 Diabetes (defects in insulin secretion or action) Other specific types Gestational diabetes Carol mattson porth Pathophysiology 7th edition TYPE 1 DIABETES: ETIOLOGY Type 1 diabetes mellitus is an autoimmune disease. It is triggered by environmental factors in genetically susceptible individuals. Both humoral & cell-mediated immunity are stimulated. GENETIC FACTORS Evidence of genetics is shown in Ethnic differences Familial clustering High concordance rate in twins Specific genetic markers Higher incidence with genetic syndromes or chromosomal defects AUTOIMMUNITY Circulating antibodies against -cells and insulin. ICA islet cell autoantibody IAA autoantibody to insulin GADA autoantibody to glutamic acid decarboxylase IA-2 autoantibody to tyrosine phosphatases IA-2 ENVIRONMENTAL SUSPECTS Viruses Coxaschie B Mumps Rubella Reoviruses Nutrition & dietary factors Cow’s milk protein Contaminated sea food Chemistry compounds or drugs TYPE 2 DIABETES: ETIOLOGY Interaction of genetic and environmental factors that impair insulin secretion and produce insulin resistance Impaired glucose uptake by skeletal muscle Increased in hepatic gluconeogenesis GENETIC FACTORS Insulin resistance •Mutation of insulin receptor substance IRS: IRS-1 mutation Ala 513 Pro、Gly 819 Arg 、Gly 972 Arg、 Arg 1221 Cys IRS-2 mutation Gly 1057 Asp •Mutation of Glucose transporter GLUT4 •Mutation of Insulin receptor •Mutation of uncoupling protein UCP B cell defects Mutation of glucokinase GCK Mutation of GLUT2 Defects of mitochondrion Defects of insulin synthesis Mutant insulin Abnormal amylin secretion ENVIRONMENTAL SUSPECTS Obesity Assume of high caloric food Stress Age ecc. Carol mattson porth Pathophysiology 7th edition Clinic features of diabetes principal Polyuria Polydipsia Polyphagia Weight loss in spite of polyphagia others Hyperglycemia Glucosuria Ketosis Acidosis COMPLICATIONS OF DIABETES Acute complications Diabetes ketoacidosis hypoglycemia Chronic complications Retinopathy Neuropathy Nephropathy Ischemic heart disease & stroke Diabetic foot ulcers Macrovascular complication Infection DIET REGULATION Regular meal plans with calorie exchange options are encouraged. 50-60% of required energy to be obtained from complex carbohydrates. Distribute carbohydrate load evenly during the day preferably 3 meals & 2 snacks with avoidance of simple sugars. Encouraged low salt, low saturated fats and high fiber diet. Antidiabetic Agents 1. Insulin Secretagogues a ) Sulphonylurea group b) Non Sulphonylurea Insulin Secretagogues 2. Insulin sensitizers a ) Metformin b) Thiazolidinedione 3. Digestive enzyme inhibitor -Glucosidase inhibitor Insulin : Acarbose Carol mattson porth Pathophysiology 7th edition Carol mattson porth Pathophysiology 7th edition