Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
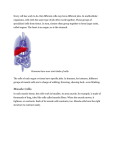
Charcot-Marie-Tooth Disease Current Topics and Treatment Options in Podiatric Medicine and Surgery September 27, 2011 New York, NY Hal Ornstein, DPM, FASPS, FAPWCA Affiliated Foot and Ankle Center, LLP 4545 Highway 9 North Howell, New Jersey 07731 (732) 905-1110 Fax (732) 905-7885 E-mail: [email protected] www.footdoctorsnj.com Many thanks to these individuals for their assistance in preparing this manuscript Katy Statler, DPM (Parts 1 & 2) Sina Safar, DPM (Parts 1 & 2) Sarah Kim, DPM (Part 3) Jake Wynes, DPM and Jasen Langley, DPM Introduction Previous publications and various descriptions date back to the mid 1800s. In 1886, the first discussions of Charcot-Marie-Tooth (CMT) were introduced by Jean-Martin Charcot and his student Pierre Marie from France, with Howard Henry Tooth from England as further contributor. Their work popularized the understanding of this disease and its effects in those afflicted. CMT effects males more than females (prevalence as high as 1/2500) with an autosomal dominant penetrance being the most common at 36/100,000 individuals. Family history usually includes phenotypic presentation of thin legs and high arches. Charcot-MarieTooth has been studied as progressive in nature with manifestations as a peripheral nerve disorder that results in diffuse degeneration of neuronal myelin sheath. Normally, the myelin sheath facilitates rapid and efficient transmission of impulses along the nerve cells. The axon is a long slender projection of a nerve cell, or neuron that conducts electrical impulses away from the neuronal cell body, or soma (Figure 1). Histologically, onion bulb formation (focal myelin swelling) is pathognomonic for this condition (Figure 2). When the myelin sheath and axon are disrupted by CMT, the frequency of signal transduction and impulses slow down, thereby causing muscle atrophy from diminished nerve signal transmission (decreased nerve conduction). CMT is identified as a hereditary neuropathy which is sub-divided based on phenotypic presentation. Hereditary Motor and Sensory Neuropathy (HMSN) and Sensory Autonomic Neuropathies are defined as a group of disorders causing alterations in peripheral nerves. Varying forms of CMT impact long term function and may exacerbate underlying disabilities. Recognizing signs and symptoms early, along with implementing an efficient mode of treatment through an interdisciplinary medical approach, allows for better patient outcomes with respect to overall comfort and sustainable lifestyle. Epidemiology, Pathophysiology, and Presentation CMT currently affects approximately 125,000 people in the United States, mostly males. There is no specific race predilection of this disorder; however African Americans are less likely to be effected. With the most common phenotypic variant of CMT (CMT1A), initial manifestations of this disorder are appreciated around the age of 30. The disease progression may be quite variable yet approximately 70% of the autosomal dominant variants will develop progressive atrophy, 23% will have atrophy arrest, and 7% of this population is left with intermittent symptomatology. . Several phenotypic variants of CMT exist including CMT1, CMT2, CMT3, CMT4, dominant intermediate CMT, and CMTX. CMT1A / 2 are the most common autosomal dominant inherited subtypes. Clinical findings with respect to age of onset, nerve conduction tests, and physical exam help elucidate which variant is diagnosed. CMT1 is further broken down into five subdivisions including CMT1A, B, C, D, and F. Approximately 40% of all HMSN fall under the CMT1A subdivision. This autosomal dominant form presents with the most prominent clinical characteristics and is associated with gene over expression at chromosome 17, causing duplication of myelin protein 22 (PMP-22). Varying gene mutations will govern phenotypic variation. An overabundance of PMP-22 leads to an abnormal structure and function of the peripheral nerve sheath. The end result is atrophy and weakness of muscles of the lower extremity. CMT1B includes 5-10% of the cases of CMT. It is autosomal dominant in which there is a point mutation of the gene that directs the manufacturing of myelin protein zero (MPZ). Patients who fall under this subdivision experience similar symptoms of those who have CMT1A, yet with increased peroneal muscular atrophy. At the present time phenotypic variants CMT1C, CMT1D and CMTF carry similar characteristics of the other autosomal dominant forms of CMT with variation in genes which mediate their function. CMT2 (axonal) typically presents with a later onset (ages 35-85) and is associated with mildly reduced NCV/EMG findings and less nerve hypertrophy / onion bulb formation compared to CMT1. Clinically these patients will present with decreased deep tendon reflexes and variable types of foot deformity. Sensory deficits are more common than motor with loss of vibration and proprioception being the most common findings. In this population it is important to evaluate these patients for trophic ulcerations secondary to diminished protective sensation (Figure 9). CMT2A is the most common; however subtypes A through I exist with more on the research horizon. Many of these subtypes are mediated by genes providing support to axonal function and depend on mode of inheritance and clinical features. Dejerine-Sottas Disease is a rare and severe demyelinating neuropathy, which falls under the category of CMT3 with autosomal dominant and recessive forms causing the disease. PMP22, EGR2, and MPZ genes have been studied. Age of onset (contrary to CMT2), is during infancy and manifests with hypotonia, delayed motor development, sensory loss in a distal to proximal progression with concomitant muscle weakness. CMT3 may be further complicated clinically by presentation areflexia, ataxia and lower extremity contractures. NCV findings are severely diminished with respect to amplitude and frequency. CMT4 is an autosomal recessive form of CMT, manifesting with primarily sensory neuropathy. It is the most rare with the most clinical severity with increased distal muscle weakness and significant Pes Cavus (high arch) foot deformity. Patients generally become nonambulatory once they reach adolescence. The main gene target has not yet been identified; however research has determined that axonal dysfunction is less likely due to mutations in structural myelin proteins. Lastly, CMTX is another form of CMT which is the second most common variant, that effects approximately 3.6/100,000 individuals in the United States and is diagnosed in 10-20% of all cases. CMTX is caused by a point mutation in the connexin-32 gene on the X chromosome. Both sexes may be affected, yet males who inherit one mutated gene maternally, show moderate to severe symptoms of the disease beginning in late childhood or adolescence; whereas the Y chromosome that males inherit paternally do not contain the connexin-32 gene mutation. Females who inherit one mutated gene from one parent and one normal gene from the other parent typically have a variable symptomatology. CMTX presents with gait disturbance, loss of deep tendon reflexes at the ankles with retained L4 reflexes in 50% of females. NCV results show mildly diminished conduction, as compared to NCV results of CMT1A patients. Phenotypic subtypes 1-5 exist with varying clinical presentations. Podiatric manifestations are primarily seen in CMTX2 with atrophy, distal weakness, areflexia, and Pes Cavus foot deformity. CMT patients often complain of foot pain, clumsiness (spinal ataxia) with or without frequent falls, recurrent ankle sprains, and various other gait disturbances. Sensory deficits are primarily with proprioception and vibratory sensation. Subjectively, patients may complain of instability, discomfort, and ankle fatigue. Common presentation of the lower extremity is demonstrated by an “inverted champagne bottle” and “stork leg” deformity (Figure 3). In CMT, the longest axons of the sciatic nerve are preferentially targeted first with muscles of smallest bulk showing initial atrophy. The lateral compartment muscle group of the leg is affected first, followed by the anterior compartment, and (in severe cases) the posterior muscle group. Pertinent anatomy is reviewed here with primary involvement of the Peroneus Brevis (PB) muscle, which is the main everter of the foot (attaching to the base of the fifth metatarsal bone). With significant demyelination this muscle is put into a mechanical disadvantage when the arch is elevated and the thereby this muscle is unable to assist in flattening the arch. The Peroneus Longus (PL) is one of the last muscles to atrophy or weaken. PL inserts proximally onto the first metatarsal and functions to plantarflex (lower) the first metatarsophalangeal joint (MPJ) downward and its function are maintained until the later stages of the disease. Progression in to the anterior compartment involving the Tibialis Anterior (TA) muscle and Extensors (Extensor Digitorum / Hallucis Longus – EDL / EHL: respectively), account for another deformity regarded as equinous which usually manifests as foot drop and “high steppage gait,” as the foot is unable to clear the ground during gait. Late atrophy of the PL, and an inability of PB muscle to function combined with intrinsic muscle wasting and atrophy provides an unstable construct for gait leading to a severe Pes Cavus/ Equinocavovarus deformity (high arch). The greater the degree of varus (inversion) combined with intrinsic muscle wasting accounts for the greater likelihood for ankle instability and digital contractures of the interphalangeal joints (IPJ) referred to as a “claw toe deformity.” This can be further complicated by injury to the lateral foot as a result of this adapted alignment of the foot. Less commonly, studies have reported that the PL is primarily weakened in 42% of cases with weakening of the Tibialis Posterior (TP) muscle in approximately 20% of cases. Atrophy of the TP muscle will result in a variant of CMT with Pes Planovalgus (flat foot), as this muscle is primarily involved in inverting the foot with resistance to pronatory influence. Diagnosis There are various ways of diagnosing CMT including: Deep Tendon Reflex (DTR) assessment which using a reflex hammer will assess the ability of the nerve to stimulate muscles effectively. When this finding is decreased or absent, further tests can be administered to further confirm diagnosis. Nerve Conduction Velocity (NCV), Electromyography (EMG), Manual Muscle Test (MMT), Nerve Biopsies, and Genetic testing are all the most common modalities of diagnosing CMT. Advanced imaging (such as Magnetic Resonance Imaging – MRI), has yet to show promise with respect to diagnosing CMT, yet has prognostic value in CNS imaging to establish rehabilitation potential for these patients. Some studies advocate for its use in demonstrating muscle atrophy secondary to demyelination with correlation with MMT. Clinically, the patient presentation is highly reliable in diagnosing one with CMT. Brewerton and colleagues first associated individuals with symptomatic high arch feet and neurologic abnormality. Their study found that 2/3 of the study population presented with these findings. The history and physical will reveal various findings such as the pathologic foot structure (Pes Cavus / Cavovarus or Equinovarus), presence of digital contractures (claw toe deformity), tripod of foot (suggestive of a rigid forefoot deformity), lateral ankle instability, and gait abnormality. Gait abnormality will require a complete biomechanical exam evaluating the patient for pelvic elevation or pelvic tilt, followed by observation for characteristic shuffling of the feet, high steppage (or Marionette Gait), and signs of excessive ankle / rearfoot inversion. Nerve conduction velocity (NCV) are suggestive when findings are less than 60% of normal with respect to decreased frequency of axonal nerve propagation. The EMG will correlate little with the clinical findings. Sural nerve biopsies may show demyelination of large nerve fibers showing histologic findings of redundant Schwann cells, collagen deposition, and fibroblast proliferation). Treatment Conservative treatments for CMT primarily involve the use of various forms of accommodative bracing and supportive measures for palliative care of symptoms and should include a multi-disciplinary approach with incorporation of Physical Therapy / Physical Medicine and Rehabilitation (PMR). The National Institute of Neurological Disorders and Strokes (NINDS) is one of many research institutions currently striving to identify mutant genes and proteins that lead to the various subtypes of CMT. Currently, no systemic treatments are available for CMT1 yet ongoing research has shown promise in both human and murine models. Sereda and colleagues have shown that progesterone antagonists will reduce PMP-22 over expression and may therefore slow the progression of nerve demyelination. Vitamin C (Ascorbic Acid) has also been studied in vivo in both animals and humans and has shown no effect in a randomized control trial of 81 children and 179 adult patients with CMT1. Finally, Neurotrophin 3 has been studied and shown to improve axonal regeneration of peripheral nerves in mouse models after PMP-22 duplication. One recent study looked at 10 affected children (ages 3-14) with CMT1A and examined the effects of injection Botulinium toxin – A into the TP or PL muscle would prevent progression of Cavovarus deformity. Their findings were that Botulinum toxin was safe yet did not affect foot morphology at 24 months. Given the relative slow progression of this disease, conservative goals are centered on mechanically controlling the deformity. These treatment modalities are reserved for individuals with a controllable deformity or who are deemed poor surgical candidates. This can be accomplished with extra-depth accommodative shoes with multi-density inlays. The benefit of this intervention, will provide support of boney prominences and prevent progression of claw toe deformity by limiting deforming forces secondary to muscle atrophy. The use of custom mold orthoses in conjunction may provide added benefit in controlling triplanar deformity through support of the sagittal plane (plantarflexed forefoot and 1st metatarsal declination), the frontal plane (rearfoot varus and increased lateral column cavus), and transverse plane deformity (forefoot adduction at the midfoot) . Further, custom Molded Ankle Foot Orthoses (MAFO) may be implemented to provide control at the ankle level and assist with drop foot deformity by allowing clearance of the ground during gait and provide a stable construct for propulsion during the last phase of the gait cycle. Proper orthotic devices can greatly reduce the chance of tripping and will help reduce injuries during physical therapy. Physicians have been able to treat CMT patients symptomatically, by physical and occupational therapy as well as by managing pain, fatigue and orthopaedic issues. CMT patients may benefit from physical therapy in various ways especially when working towards relieving functional deterioration. Classically, rehabilitation programs involve a range of exercises including picking up marbles, towel rolling, extensor strengthening exercises, and much more. Strength training may assist patients in decreasing severity of contracture from muscle imbalance. Not only does this training help improve function of weakened muscles but it also helps to maximize the strength of uninvolved muscles. Studies show that even a small increase of strength in effected muscle can result in significant improvement on patients. This leads to greater tolerance of activities such as writing, and ambulation. It is important to note that the results from physical therapy will differ from patient to patient. Progress can be slow with certain patients, while for others’ it may produce a major increase in muscle strength and resistance. Not knowing the ultimate outcome can cause physical therapy to become an exhausting process for CMT patients; however, it is very important for patients to be compliant with the physical therapy program, in order to notice significant improvements in their condition. Many patients with CMT disease become sedentary which may precipitate deterioration of the muscles but also deterioration of their overall health. Although excessive training is contraindicated in CMT patients due to potential injuries that may occur during this type of training, studies have shown that mild to moderate training can improve overall strength and health by decreasing heart disease, body fat, and lowering blood pressure; while increasing muscular and cardiovascular endurance. It is important to consult a physical therapist who can design an exercise program specific for individual’s needs and thus help to avoid injuries. It is also important to manage fatigue in CMT patients because more energy is spent during exercises than that of a comparable healthy individual. When physical therapy is started in the early stages, it can have a dramatic effect in delaying nerve deterioration and muscle weakness. Some CMT patients experience weakness in their arms and hands, causing difficulty with gripping and finger movement. Occupational therapy can make significant difference in the quality of life by using assistive devices such as special rubber grips on doorknobs or clothing with snaps instead of buttons. Typically, suboptimal results have been reported for non surgical management of rigid deformities. When the decision is made to treat a patient surgically with CMT, it is important to factor in several elements including which of the motor units remaining are functional, how flexible or rigid the established deformities are, and whether ligamentous laxity is present. Goals of surgery are that all fixed deformities must be corrected to include muscle / tendon imbalances in order to prevent recurrence. Typical Deformities Outlined: Forefoot Deformities Toe/ digit Deformities Metatarsal Deformities Midfoot Deformities Rearfoot Deformities Ankle / Equinus Deformities Dropfoot Deformities Tendon Deformities Muscle imbalances Correcting these deformities before any further progression takes place will have a positive impact on the outcome of the surgical procedures. Many patients who have a flexible form of a Cavovarus deformity (Figure 4) and plantarflexed 1st ray (figure 6) associated with CMT have been surgically treated with reconstruction involving tendon transfers with or without 1st metatarsal / midfoot / calcaneal osteotomy (taking a wedge of bone from the first metatarsal, midfoot, or calcaneus with realignment) and lesser digit stabilization procedures (lesser toe fusions) (Figure 7). The long term results show positive outcomes with having a lower progression of degenerative changes in comparison of those who had a triple arthrodesis (multiple fusions instead of reconstruction) performed in a span of twenty four years. The goal of the reconstruction compared to the arthrodesis was to efficiently correct the Cavovarus deformity with respect to function, radiographic changes, and gait/walking patterns. A triple arthrodesis procedure was concluded to be left as a last resort / salvage procedure when all other procedures fail (Figure 8). The triple arthrodesis procedure has greater chance of not uniting, foot alignment errors, and various forms of immobility issues secondary to arthritic changes at adjacent joints. Concluding remarks In closing, CMT is a challenging progressive disease process with a variable phenotypic presentation. Presently, there is no cure which will alter the course of the disease, but patients should be aware that there are alternatives available to minimize the manifestation of the disease. It is crucial to assess the patient with respect to patient goals, quality of life, and what interventions a physician can provide to the patient. Once the disease is identified treatment should then be assumed by the primary care physician, neurologist, podiatric surgeon, physical medicine rehabilitation specialist or physical therapist, and even genetic counselor. Patients with Identifying the apex and characteristics of the deformity, along with associated muscular imbalances provide the best chance for optimal prognosis. For instance, young patients tend to benefit from early surgical procedures to include reconstructive approaches; whereas patients who suffer from severe or multi-planar deformities may respond best to triple arthrodesis and adjunctive tendon transfers. It is imperative to treat this debilitating pathology through a methodical and inter-disciplinary approach to achieve the best possible patient outcomes. References 1. Berciano J, Gallardo E, Garcıa A, Pelayo-Negro AL, Infante G, Combarros O. New insights into the pathophysiology of pes cavus in Charcot–Marie–Tooth disease type 1A duplication. J Neurol 2011 2. Brewerton DA, Sandifer PH, Sweetnam DR. Br Med J. 1963 Sep 14;2(5358):659-61 3. Burns J, Ouvrier RA, Yiu EM, et al. Effect of ascorbic acid in patients with Charcot-MarieTooth disease type 1A: a multicentre, randomized, double blind, placebo-controlled trial. Lancet Neurol 2009; 8: 1103. 4. Burns J, Ryan MM, Ouvrier RA. Evolution of Foot and Ankle Manifestations in Children with CMT1A. Muscle Nerve 39: 158 –166, 2009 5. Burns J, Scheinberg A, Ryan MM, Ouvrier RA. Randomized Trial of Botulinum Toxin to Prevent Pes Cavus Progression in Pediatric Charcot-Marie-Tooth Type 1A. Muscle and Nerve. 262 -7, 2010 6. Chetlin R, Gutmann L, Tarnopolsky M, Ullrich I, Yeater, R. Resistance Training Effectiveness in Patients with Charcot-Marie –Tooth Disease: Recommendations for Exercise Prescription; Arch Phys Med Rehabil 2004; 85: 1217-1222 7. Croban et al. CMT Facts IV. Treatment of Familial Neuropathies. Vol 4. 1998. 8. Del Porto LA, Nicholson GA, Ketheswaren P. Correlation between muscle atrophy on MRI and manual strength testing in hereditary neuropathies. Journal of Clinical Neuroscience 17 874– 878, 2010 9. Duval A, Kalempokas K, Penicaud A, Guiochon A, Mantel E, Bachmeyer C. Neuropathic leg ulcer indicating late adult-onset of Charcot-Marie-Tooth disease. J Am Acad Dermatol (64); 1215-1216, 2011. 10. Lupski et al. Finding CMT gene ends a quest and begins a new era. Science Med. March 2010. 11. Guyton, G. Orthopaedic Aspects of Charcot-Marie-Tooth Disease. Foot and Ankle International. Vol 27. 2006; 1003-10. 12. Hewitt SM, Tagoe M. Surgical Management of Pes Cavus Deformity with an Underlying Neurological Disorder: A Case Presentation. JFAS (50) 235–240, 2011 13. McGlamry’s Comprehensive Textbook of Foot and Ankle Surgery. Third Ed. Section 5: Chapter 34 Charcot- Marie- Tooth Disease. 2001; 1071-1089 14. Menotti F, Felici F, Damiani A, Mangiola F, Vannicelli R, Macaluso A. Charcot-Marie Tooth 1A patients with a higher energy cost of walking than healthy individuals; Neuromuscular Disorders 2011; 21:52-573 15. Micaleff J, Attarian S, Dubourg O, et al. Effect of ascorbic acid in patients with Charcot Marie Tooth disease type 1A: a multicentre, randomized, double blind, placebo-controlled trial. Lancet Neurol 2009; 8:1103 16. Mondelli M. Some considerations on atypical cases of Charcot-Marie-Tooth disease and use of genetic testing in idiopathic polyneuropathies. Clinical Neurology and Neurosurgery 112 (2010) 745–746 17. Oatis Carol. Charcot-Marie Tooth Disorders: Pathophysiology, Molecular Genetics and Therapy. John Wiley & Sons, Inc. 1990 18. Ramcharitar SI: Lower Extremity Manifestations of Neuromuscular Diseases. Clinics of Podiatric Medicine & Surgery, 15: 722-724, 1998. 19. Reilly M, Murphy S, Laura M. Charcot-Marie-Tooth Disease. Journal of the Peripheral Nervous System 2011; 16:1-14 20. Sereda MW, Meyer zu Horste G, Suter U, et al. Therapeutic administration of progesterone antagonist in a model of Charcot-Marie-Tooth disease (CMT-1A). Nat Med 2003; 9:1533 21. Van der Linden MH, Van der Linden SC, A, Hendricks HT, Van Engelen BGM, Geurts ACH. Postural instability in Charcot-Marie-Tooth type 1A patients is strongly associated with reduced somatosensation. Gait & Posture 31 (2010) 483–488 22. Walsh B, Fontera W. Brace modification improves aerobic performance in Charcot-Marie Tooth disease: A single-subject design. AM J Phys Med Rehabil 2001;80:578-582. 23. Ward et al. “Long-Term Results of Reconstruction for Treatment of a Flexible Cavovarus Foot in CMT disease.” The Journal of Bone and Joint Surgery. 90:2631-42. 2008. 24. Westmore et al. “Long-Term Results of Triple Arthrodesis in CMT disease.” The Journal of Bone and Joint Surgery. 71-A No 3. 1989. Figure Legend Figure 1. Neuronal structure of non-pathologic axon Figure 2. Onion bulb formation. Electron micrograph of sural nerve from an individual with CMT 1A showing characteristic concentric Schwann cell cytoplasmic processes surrounding a myelinated axon (adapted from Benstead TJ, Grant IA. Charcot-MarieTooth Disease and Related Inherited Peripheral Neuropathies. Can. J. Neurol. Sci. 2001; 28: 199-214) Figure 3. Clinical presentation of CMT patient with classic “stork leg” appearance and Equinocavovarus foot alignment and claw toe deformity. (Adapted from McGlamry’s Comprehensive Textbook of Foot and Ankle Surgery. Third Ed. Section 5: Chapter 34 Charcot- Marie- Tooth Disease. 2001; 1071-1089) Figure 4. Clinical photograph of patient with noticeable Pes Cavus foot deformity. Figure 5. Diagram of subtalar joint (STJ), midtarsal joint (MTJ), and forefoot with first ray including the 1st metatarsal bone and its associated phalanges (proximal, middle, and distal). Figure 6. Radiographic assessment with increased calcaneal inclination angle, talar dorsiflexion, and first metatarsal declination. Figure 7. Forefoot reconstruction consisting of interphalangeal joint arthrodesis 1-4, arthroplasty 5th digit, and dorsiflexory base wedge osteotomy of the 1st metatarsal (Adapted from McGlamry’s Comprehensive Textbook of Foot and Ankle Surgery. Third Ed. Section 5: Chapter 34 Charcot- Marie- Tooth Disease. 2001; 1071-1089) Figure 8. (A) Post operative patient who underwent triple arthrodesis and dorsiflexory base wedge osteotomy with tibialis posterior tendon transfer. (B) 1 year post operatively with hardware removed. No arthritic findings / symptomatology. Figure 9. (A,B) Fibrinous partial thickness ulceration to lateral forefoot at boney prominence secondary to CMT neuropathy CMT and associated drop foot