Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Sexually dimorphic nucleus wikipedia , lookup
Hormone replacement therapy (menopause) wikipedia , lookup
Hypothyroidism wikipedia , lookup
Testosterone wikipedia , lookup
Graves' disease wikipedia , lookup
Progesterone wikipedia , lookup
Bioidentical hormone replacement therapy wikipedia , lookup
Hormone replacement therapy (male-to-female) wikipedia , lookup
Hormone replacement therapy (female-to-male) wikipedia , lookup
Hypopituitarism wikipedia , lookup
Hyperandrogenism wikipedia , lookup
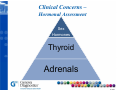
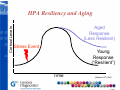
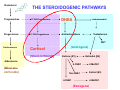
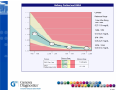
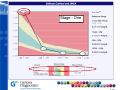
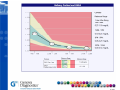
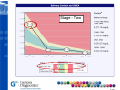
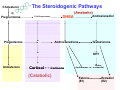
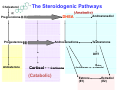
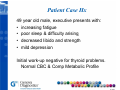
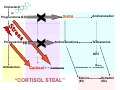
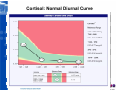
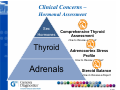
Adrenal Dysfunction: The Role of Stress Dr. Stephen Goldman Genova Diagnostics © 2012 2008 Adrenal Dysfunction: The Role of Stress Dr. Stephen Goldman Genova Diagnostics Sex Hormones Thyroid Ad Adrenals l © 2012 2008 Dr. Stephen Goldman Teresa McBride, ND © 2012 2008 Technical Issues Clinical Questions Clinical Questions will be answered during the final fifteen (15) minutes of the webinar. webinar 2010 © 2012 Clinical Concerns – Hormonal Assessment Sex Hormones Th id Thyroid Adrenals 2010 © 2012 Adrenal Dysfunction: Si Signs & Symptoms S t • Tired for no reason. • Trouble getting up in the morning, even when you go to bed at a reasonable hour hour. • Feeling rundown or overwhelmed. • Difficulty bouncing back from stress or illness. • F Feell more awake, k alert l t and d energetic ti after ft 6PM than you do all day. 2010 © 2012 Adrenal Dysfunction: P th h i l Pathophysiology • The adrenal glands produce the hormones cortisol and DHEA. • Over secretion of cortisol triggered by daily stress from work, family or other sources can wear down the internal system and cause fatigue. • During this process DHEA may be compromised, i d causing i other th ffunctions ti tto suffer. 2010 © 2012 Corttisol Le evels HPA Resiliency and Aging Aged espo se Response (Less Resilient) Stress Event Young Response (“Resilient”) Time (Seeman TE 1994) 2010 © 2012 What Constitutes “Stress? • “Fight Fight or flight flight” responses; fear fear, anxiety, worry • Depression, Depression feelings of defeat or helplessness • Pain syndromes • Infection, inflammation • Hypoglycemia H l i • Inadequate sleep • Disrupted light cycles p • Toxic exposure 2010 © 2012 2010 © 2012 STRESS HPA Axis Hypothalamus & Pituitary ACTH Adrenal Cortex DHEA (anabolic) Cortisol C ti l (catabolic) Stress 2010 © 2012 Cholesterol Pregnenolone Progesterone THE STEROIDOGENIC PATHWAYS 17-OH-Pregnenolone 17-OH-Progesterone 17 OH Progesterone DHEA Androstenediol Androstenedione Testosterone DHT Corticosterone Cortisol (Glucocorticoids) (A d (Androgens) ) Estrone ((E1)) Estradiol ((E2)) Aldosterone 2-OHE1 (Mineralocorticoids) 16α-OHE1 4 OHE1 4-OHE1 2-MeOE1 Estriol (E3) 4 MeOE1 4-MeOE1 (Estrogens) Cholesterol Pregnenolone Progesterone 17-OH-Pregnenolone 17-OH-Progesterone 17 OH Progesterone DHEA Androstenediol Androstenedione Testosterone DHT Corticosterone Cortisol (Glucocorticoids) (A d (Androgens) ) Estrone ((E1)) Estradiol ((E2)) Aldosterone 2-OHE1 Cortisol & DHEA derive from same precursors 16α-OHE1 4 OHE1 4-OHE1 2-MeOE1 Estriol (E3) 4 MeOE1 4-MeOE1 (Estrogens) Saliva Plasma Blood (bound + free) Basement membrane Saliva Saliva (only free) Basement membrane 2010 © 2012 2010 © 2012 Stage - One 2010 © 2012 2010 © 2012 Stage - Two 2010 © 2012 Stage - Three 2010 © 2012 Cholesterol The Steroidogenic Pathways (Anabolic) Pregnenolone Androstenediol DHEA 17-OH-Pregnenolone Progesterone Androstenedione Testosterone DHT Aldosterone Cortisol Cortisone (Catabolic) Androsterone Estrone (E1) Androstanediol Estradiol (E2) Cholesterol The Steroidogenic Pathways (Anabolic) Pregnenolone Androstenediol DHEA 17-OH-Pregnenolone Progesterone Androstenedione Testosterone DHT Aldosterone Cortisol Cortisone (Catabolic) Androsterone Estrone (E1) Androstanediol Estradiol (E2) Cholesterol Pregnenolone (Anabolic) Progesterone Androstenediol DHEA 17-OH-Pregnenolone Androstenedione Testosterone DHT Aldosterone Cortisol Cortisone (Catabolic) Androsterone Estrone (E1) Androstanediol Estradiol (E2) “Cortisol Steal” • St Stress off acute t immobilization i bili ti iin rats t inhibition i hibiti of 17α-hydroxylase and 17,20 lyase (Orr Te 1994) • Severe illness relative shift in pregnenolone away from androgens and mineralocorticoids, and toward glucocorticoids increased serum and urine cortisol (Parker LN 1985) • Serum cortisol:DHEA-S ratio higher in elderly hip patients compared p with controls;; reduced fracture p immunity in these patients (Butcher SK 2005) 2010 © 2012 Patient Case Hx 49 year old male, executive presents with: • increasing fatigue • poor sleep & difficulty arising • decreased libido and strength • mild ild d depression i Initial work-up negative for thyroid problems. p Metabolic Profile Normal CBC & Comp 2010 © 2012 Tests • Diagnostic g – Adrenocortex Stress Profile – Complete Hormones (urine) • Health Related Issues – Comprehensive Thyroid Assessment – Sex Hormones – result in deficiencies (precursor hormones) 2010 © 2012 Salivary Cortisol and DHEA 2010 © 2012 Cholesterol Pregnenolone Progesterone 17-OH-Pregnenolone 17-OH-Progesterone 17 OH Progesterone DHEA Androstenediol Androstenedione Testosterone DHT Corticosterone Cortisol (Glucocorticoids) (A d (Androgens) ) Estrone ((E1)) Estradiol ((E2)) Aldosterone 2-OHE1 Cortisol & DHEA derive from same precursors 16α-OHE1 4 OHE1 4-OHE1 2-MeOE1 Estriol (E3) 4 MeOE1 4-MeOE1 (Estrogens) Cholesterol Pregnenolone 17-OH-Pregnenolone Progesterone Androstenediol DHEA Androstenedione Testosterone DHT Aldosterone Cortisol Cortisone “CORTISOL CORTISOL STEAL STEAL” Androsterone Estrone (E1) Androstanediol Estradiol (E2) Stress and Steroid Synthesis “Wear and Tear” vs. “Rest and Recovery” 2010 © 2012 STRESS N Normal Stress Response l St R (+) Hypothalamus & Pit Pituitary it Sympathetic response (alarm) (cortisol p ) receptors) (-) (ACTH) (negative feedback loop) Adrenal Cortex DHEA CORTISOL (Anabolic) (C t b li ) (Catabolic) 2010 © 2012 A i Actions off Cortisol C i l – Catabolic C b li • Maintains blood glucose levels during stress (gluconeogenesis) g ) additional reactions (g glucose to brain, heart, lungs, skeletal muscle • Promotes hepatic protein synthesis and gluconeogenesis; stimulates protein catabolism elsewhere in body • Stimulates glycogenolysis, lipolysis • Participates with aldosterone in Na reabsorption maintenance of perfusion pressures to critical organs during stress 2010 © 2012 A i Actions off Cortisol C i l – Catabolic C b li • Anti-inflammatory – downregulates phospholipase p p p A2,, inflammatory y cytokines y • Inhibitory feedback to hypothalamus and pituitary downregulation of CRH and ACTH • Cortisol highest in a.m., with gradual decline over course off day; d normall di diurnall curve indicates healthy adaptation to stress 2010 © 2012 Cortisol: Normal Diurnal Curve 2010 © 2012 Actions of DHEA – Anabolic • • • • • • Prohormone P h ffor sex steroids t id Anti-glucocorticoid Immune supporting Anti-atherogenic Anti atherogenic, lowers serum triglycerides Enhances insulin sensitivity; anti-obesity effect M i t i tissue Maintains ti strength t th and d repair, i supports t bone density • Neuroprotective; enhances memory • Promotes sense of well-being g 2010 © 2012 DHEA • Long-term indicator of DHEA status • Maximal values at 20 and 30 years of age; thereafter, both DHEA and DHEA-S decrease markedly… 2010 © 2012 DHEA & DHEA S (serum): Effects of Aging DHEA & DHEA‐S (serum): Effects of Aging Serum DHEA (nmol/L) DHEA-fatty acid esters (nM) Serum DHEA-S (nmol/L) Serum androstenediol (nM) (Labrie F 2005) 2010 © 2012 DHEA (March, 2007 study of African-American women (March women, aged 49-65 years)… “DHEA-S and E2 declined between the ages of 49 and 65 years, whereas total testosterone, SHBG and the Free Androgen Index remained stable…Lower DHEA-S levels were independently associated with a higher degree of physical disability and depressive symptoms.” (Haren MT 2007) 2010 © 2012 Clinical Concerns – Hormonal Assessment Sex Hormones Comprehensive Thyroid A Assessment t How to Review a Report Th id Thyroid Adrenocortex Stress Profile How to Review a Report Adrenals Steroid Balance How to Review a Report 2010 © 2012 HPA Axis STRESS HPT Axis Hypothalamus & Pituitary Hypothalamus & Pituitary ACTH TSH Adrenal Cortex Thyroid T4 DHEA (anabolic) Cortisol C ti l (catabolic) Liver & Kidney rT3 T3 Cell Nucleus 2010 © 2012 Adrenocorticol Hyperactivity • Life-saving in the short-term! (catabolism frees up energy reserves) • Persistent cortisol production immune suppression, pp , hyperglycemia, yp g y , insulin resistance,, central adiposity, hypertension, memory p ((hippocampal pp p damage), g ), impairment hyperlipidemia, impaired hepatic T4T3 conversion 2010 © 2012 Hypothalamus TRH Pituitary TSH H Liver or Li Kidney (5’deiodinase) (Se) rT3 T3 T3 (Inactive) (Active) ~ 85% Thyroid Gland 5% T3 (5 deiodinase) 95% T4 Cell Nucleus 2010 © 2012 TRH Hypothalamus Pituitary TSH H Liver or Li Kidney 95% T4 rT3 T3 T3 (Inactive) (Active) 5% T3 STRESS Thyroid Gland Cell Nucleus 2010 © 2012 Adrenocorticol Hypoactivity • High CRH is also possible in adrenal hypoactivity (lack of inhibitory cortisol feedback p persistent output p of CRH excessive adrenalin production) g , hypotension, yp , • Low cortisol fatigue, hypoglycemia, sugar cravings, increased inflammatory response, conversion T4 to T3. 2010 © 2012 TRH Hypothalamus Pituitary TSH H Liver or Li Kidney 95% T4 rT3 T3 T3 (Inactive) (Active) 5% T3 Chronic Stress Thyroid Gland Cell Nucleus 2010 © 2012 Factors Promoting Conversion of T4 to T3 Micro-nutrients: selenium, potassium, iodine, iron, zinc Vitamins: A E A, E, riboflavin Hormones: cortisol (physiologic doses) growth hormone, testosterone i insulin, li glucagon l melatonin 2010 © 2012 Case Study 55yo Female • Menopausal x 3 years • G3P1 (SAB2) y • Menarche @ 13yo • + Fam Hx Breast CA and Prostate CA • Patient with excellent diet of vegetables and fruits Symptoms: • Problems with climacteric symptoms, decreased libido, sleep problems • Began on TD Cream – BiEst (1mg), Progesterone (20mg), Testosterone (0.5mg) – 6 months prior • Symptoms persist, particularly evening anxiety and sleep disturbance. 2010 © 2012 Case Studyy Cortisol = Low normal DHEA = Low ((age-adjusted) g j ) 2010 © 2012 Case Study Imbalance = Sex Hormones • Measure Sex Hormones with Complete Hormones (Urine) – Balance Progesterone, Estrogens, & Testosterone Imbalance = Adrenal Hormones • Support Adrenals – – – – Supplement with DHEA 10mg qD B-Vitamins ((B2, B6, B12, Folate)) + Vitamin C Adrenal Herbs (Ashwaghanda, Rhodiola) Heart Rate Variabilityy BioFeedback 2010 © 2012 Case Studyy 2010 © 2012 Cholesterol Pregnenolone (Anabolic) Progesterone Androstenediol DHEA 17-OH-Pregnenolone Androstenedione Testosterone DHT Aldosterone Cortisol Cortisone (Catabolic) Androsterone Estrone (E1) Androstanediol Estradiol (E2) STRESS N Normal Stress Response l St R (+) Hypothalamus & Pituitary Sympathetic response (alarm) (cortisol p ) receptors) (-) (ACTH) (negative feedback loop) Adrenal Cortex DHEA CORTISOL 2010 © 2012 Personalizing Hormone P li i H Diagnosis & Treatment: The Whole Picture Patrick Hanaway, Hanaway MD © 2012 2008 Questions & Answers Register for upcoming LiveGDX Webinars g online @ www.gdx.net 2010 © 2012 2010 © 2012 2010 © 2012 2010 © 2012 LiveGDX 2010 © 2012 Upcoming LiveGDX Webinars The Endocrine Pyramid • 5/23/12 –Thyroid Dysfunction: » Nutrients & Toxins • 6/27/12 – Sex Hormone Dysfunction: y » The Role of Stress, Nutrients & Inflammation Sex Hormones Thyroid Adrenals 2010 © 2012