Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
A pilot phase II study of digitoxin for
Androgen-Independent Prostate Cancer (AIPC)
Principal Investigators:
Johan Haux and Hans Hedelin
Departments of Medicine and Surgery
KSS
SE-541 85 Skövde
Sweden
Table of contents
1.
1.1.
1.2.
1.3.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
Introduction
Background
Digitalis and cancer
Rationale
Objective
Study design
Inclusion criteria
Exclusion criteria
Concurrent medication
Precautions
Study drug
Objective response
Primary endpoint
Secondary endpoint
Statistical considerations
Criteria for removal from protocol treatment
Adverse events
Patient information and informed consent
References
Flow chart
Clinical Research File
1. Introduction
1.1.
Background
Prostate cancer is the most common cancer among men in Sweden. Every year about
7600 men are diagnosed with prostate cancer. The incidence has increased the last years
mainly due to increased diagnostic activity and an increased life span of the population
(1). Since more than 50 years androgen ablation has been a cornerstone in the treatment.
Most patients with metastatic disease will initially respond to endocrine therapy,
however, the effect is temporary and the median time of duration of response is about 18
months. Survival time after secondary progress, i.e. when the disease has become
androgen independent, is approximately 1 year (1).
Until recently no clinical studies had shown any impact on survival that could be
attributed to second line therapy. In 2004 it was reported from two studies, TAX 327
and SWOG 9916, that taxotere has significant effects in men with hormone independent
prostate cancer. Prior to taxotere, no chemotherapy drug has ever shown a survival
benefit for men with prostate cancer resistant to hormone therapy.
The TAX 327 study showed that the median survival was 16.5 months in the
mitoxantrone group, 18.9 months in the group given docetaxel every 3 weeks, and 17.4
months in the group given weekly docetaxel (2).
In the SWOG 9916 study it was shown that in an intention-to-treat analysis, the median
overall survival was longer in the group given docetaxel and estramustine than in the
group given mitoxantrone and prednisone (17.5 months vs. 15.6 months, P=0.02 by the
log-rank test (3). Thus, we have a lot more to wish concerning effectiveness of drugs for
this disease.
Most often patients with AIPC present without measurable disease. Thus, conventional
criteria for objective response are frequently not applicable. On the other hand
biochemical response can be assessed by repeated serum PSA (S-PSA) measurements.
Actually, eligibility and response guidelines for phase II clinical trials in these patients
have been developed by the Prostate-Specific Antigen (PSA) Working group (4). PSA
has been shown to be useful in this setting when new treatments are evaluated in patients
with AIPC.
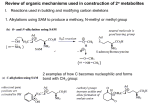
1.2. Digitalis and cancer
During our work on anti-cancer molecules utilized by the innate immune system in
humans, we found a rationale to examine the effects of digitalis on malignant cells
(5,6,7). Since ancient times reports have indicated that digitalis may have anti-cancer
effects and in our laboratory studies digitalis induced apoptosis in different types of
cancer cells in clinically relevant concentrations (8,9). For prostate cancer we used 4
different human cell lines, three androgen independent (DU-145, PC-3 and TSU – prl)
and one androgen dependent LNCaP. These four cell lines were sensitive for digitoxin
(10). The digitoxin treated prostate cancer cells that survived also accumulated in the
G2M phase of the cell cycle. That might indicate that they will be more sensitive for
irradiation as we have shown for breast cancer cell lines (11). The cell death induction
by digitoxin is not dependent on functional p53. Subsequent studies from several
different institutes, among them the MD Anderson Cancer Center in Texas, have
confirmed that prostate cancer cells are sensitive for digitalis (12,13,14)
Further, we found that digitoxin seems to be the most potent of the clinically used
digitalis derivatives concerning the anti-cancer effects. That has also been supported by
other studies (15).
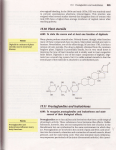
Since several decades the inhibition of the ubiquitous Na+/K+ATP:ase has been the well
known working mechanism of digitalis (16). Interestingly, already in 1993 it was
proposed that the Na+/K+ATP:ase might be the actual androgen receptor of the prostate
(17). It is evident that not just the inhibition of the Na+/K+ATP:ase can explain all the
anticancer effects (18). Recently we have learnt much more concerning mechanisms of
action of digitalis. Digitoxin is a potent inhibitor of the transcription factor NF-kB and
inhibits production of pro-inflammatory cytokines such as TNF-a and IL-8 (19,20). The
last years we have learnt that infection/inflammation and the associated proinflammatory cytokines have great impact, not only on well known inflammatory
diseases such as Mb. Crohn, ulcerative colitis, but also on cancer (21,22). Inhibition of
these pro-inflammatory cytokines also inhibit angiogenesis (23). Thus, drugs that
inhibit NF-kB, such as thalidomide, and now digitoxin, are of interest for several,
seemingly diverse diseases, but on the molecular level dependent on some of the same
mechanisms (24). The latest screening procedures on gene level for potential anti-cancer
drugs also point out digitoxin (25).
The common picture is that drug candidates that exhibit anti-cancer effects in vitro fail
in clinical cancer studies. Thus, to learn more about eventual impact on cancer we
performed a study to examine cancer in a population taking digitoxin for cardiac
conditions. However, the age is high and the morbidity and mortality due to cardiac
disease are high in the population taking digitoxin. Eventual anti-cancer effects would
easily “drown” in this study set-up. Despite that, an anti-cancer effect of digitoxin was
detected for kidney/urinary tract cancers and leukemia/lymphoma (26).
The indications for digitoxin treatments today are cardiac congestion and
supraventricular tachyarrhtmias. Studies on healthy volunteers that take digitoxin show a
decrease of diastolic blood pressure and heart rate, especially during rest (27). Thus,
digitoxin in doses used for the cardiac indications seems not to give any alarming side
effects in humans without cardiac problems (28).
The anti-cancer effects of digitoxin are dose-dependent; the higher the dose, the more
potent the anti-cancer effects. Thus, for cancer treatment as high concentrations as
possible, without inducing toxic symptoms, should be used. For practical reasons one
should aim at a concentration just beneath the recommended upper limit for treatment of
cardiac disease (about 25 ng/l) (29).
1.3. Rationale
There are no curative therapies for patients with androgen independent prostate cancer
(AIPC). New therapies for these patients are urgently needed. Digitoxin shows potent
anti-cancer activities in androgen dependent and independent prostate cancer cell lines.
Digitoxin targets many of the mechanisms of interest for new anti-cancer agents and
may represent a novel type of drug therapy for prostate cancer that should be evaluated
in clinical studies.
2. Objective
Investigate if digitoxin has an effect on hormonal refractory carcinoma of the prostate.
The primary endpoint is the proportion of complete or partial responders as determined
by repeated S-PSA assessments.
3. Study design
This is a pilot phase II, non-randomized, single-arm study of digitoxin for AndrogenIndependent Prostate Cancer (AIPC).
In the first stage we plan to accrue 15 patients. If no responder is found among these, the
study is closed and the drug is regarded as inactive for this indication. If one or more
patients respond, additional 15 patients will be accrued, see section 12 for statistical
considerations.
The patients will start with the same dose of digitoxin. Digitoxin tablets, 0.1 mg, will be
taken two tablets in the morning and three in the evening day one and day two, thus a
total amount of 1.0 mg digitoxin the first two days. On day three a daily maintenance
dose of 0.1 mg will be started.
If at four weeks there is no evidence of digitalis toxicity and the blood concentration is
< 20 ng/ml, the maintenance dose may be increased to aim at a steady-state
concentration just below the upper recommended limit, 25 ng/ml. Serum digitoxin levels
will be obtained just before daily dose every four weeks or whenever there is any sign of
digitalis toxicity. Therapeutic plasma concentration of digitoxin is 15-25 ng/ml (29).
There will be one scheduled visit to nurse or physician every 4th week, and whenever
needed.
Physical examination will performed at all visits and according to standard routines.
Laboratory studies included a complete blood count, electrolytes, creatinine, glucose,
albumin, calcium, alkaline phosphatase, bilirubin, ASAT, ALAT, S-PSA and
S-digitoxin will be checked during the study at different time intervals, see section 17,
flow chart.
The patients will be treated with digitoxin according to the schedule until progression of
the AIPC, unacceptable side effects occur, or until death, whatever comes first.
Efficacy assessments will include analysis of S-PSA, evaluation of eventual measurable
tumors clinically and with radiological examinations, the patients’ performance status
and weight. Pain medication will be analyzed. Eventual effects on skeletal lesions will
also be followed by diagnostic radiology.
4. Inclusion criteria
4.1. Age 50-80 years
4.2. Life expectancy greater than 3 months
4.3. Histologically proven carcinoma of the prostate (any T or N category) with
evidence of progression following primary hormonal treatment, i.e. hormone resistant.
4.4. S-PSA level at trial entry should be greater than or equal to 5 ng/ml. S-PSA
progression should be documented by two consecutive increases in S-PSA before
enrollment. Each increase in S-PSA should be at least one unit and it should be at least 4
weeks between the samples.
4.5. The patient has WHO performance status 0-2, for definition see Appendix.
4.6. Patient is receiving hormone therapy (i.e. an LHRH agonist and/or anti-androgen)
and/or orchiectomy has been performed. Ongoing endocrine treatment should continue.
4.7. Patients must be physically, mentally and emotionally able to give informed
consent.
4.8. Signed informed consent has been given.
4.9. Prior radiation therapy will be allowed, but radiotherapy during the study is not
allowed. No concurrent other chemotherapy is given in the study.
5. Exclusion criteria
5.1. The patient has a relevant concurrent disease or baseline laboratory results, which
put the patient at risk to take digitoxin.
5.2. Patients with heart disease already on a cardiac glycoside are not eligible.
5.3. No other prior malignancy is allowed except for adequately treated basal cell
cancer.
6. Concurrent medication
All concomitant medications will be recorded in the patient file from dosing day 1 until
the end of treatment. Anti-androgen therapy that the patient is on at study entrance
should be continued. No new drugs should be given, except analgesics, chronic
treatments for concomitant medical conditions, or agents required for life-threatening
medical problems. The hormonal treatment the patient is on at study entrance should be
continued.
7. Precautions
7.1. Electrolyte imbalance:
Calcium; Hypocalcaemia from any cause predisposes the patient to digitalis toxicity.
Potassium; Hypokalemia sensitizes the myocardium to digitalis. Therefore, it is
important to maintain normal serum potassium levels.
In general avoid rapid shifts in serum potassium or other electrolytes.
Magnesium; Hypomagnesaemia may predispose to digitalis toxicity.
7.2. Cardiac Problems
Patients with incomplete AV block may develop advanced or complete heart block.
Patients with acute myocardial infarction, severe pulmonary disease, or advanced heart
failure may be more sensitive to digitalis and prone to rhythm disturbances.
7.3. Contraindications
Previous toxic responses to digitalis preparations, ventricular fibrillation, ventricular
tachycardia, or allergy to digitalis are contraindications.
7.4. Drug Interactions
A variety of drugs may affect the serum concentration of cardiac glycosides via various
mechanisms;
Beta blockers: These drugs may inhibit AV nodal conduction and can result in complete
heart block.
Potassium-sparing diuretics: Spironolactone may increase or decrease toxic effects of
digitalis glycosides. Changes cannot be predicted and patients should be carefully
monitored.
Sympathomimetics: Concomitant use with digitoxin can increase the risk of cardiac
arrhythmias because enhanced ectopic pacemaker activity.
Thiazide and loop diuretics and amphotheracin B increase potassium loss, possibly
resulting in hypokalemia and will be used with caution.
Thyroid hormones: Thyroid hormones may decrease the therapeutic effectiveness of
cardiac glycosides.
8. Study Drug
8.1. Digitoxin is a single cardiac glycoside extracted from the leaves of Digitalis
purpurea. Digitoxin is
8.2. Structural formula
8.3. Source of Drug:
We purchase it from Nycomed.
8.4. Pharmacology
More than 200 years ago, William Withering introduced the rationale use of Foxglove
extracts, digitalis for cardiac conditions. Digitoxin is extracted from Digitalis purpurea.
The activity of digitoxin on the myocardium is dose-related and involves a direct action
on myocardium, the specialized conduction system, and indirect actions mediated by the
autonomic nervous system. These indirect actions involve a vagomimetic action that
results in increased carotid sinus nerve activity.
Digitoxin has a direct inotropic effect on the myocardium The cellular basis for the
inotropic effects appears to be inhibition of sodium and potassium ATPase that increase
calcium available to activate the contractile proteins, actin and myosin.
The mechanism behind the anti-cancer effects of digitalis is currently under
investigation. However, we already know that digitalis interacts with signaling
mechanism involving tyrosinase receptors in a complex way, and inhibit the
transcription factor NF-kB. Apoptosis is induced in an array of different human cancer
cells and angiogenesis is inhibited.
Digitoxin is greater than 90% absorbed following oral administration. Concurrent food
intake slows absorption of digitoxin but is complete, except when taken with meals high
in bran fiber. Cardiac glycosides are widely distributed in tissues. High digitoxin
concentrations are found in the myocardium, skeletal muscle, liver, brain and kidneys.
50-80% of administered digitoxin is degraded by the liver to inactive metabolites that
are excreted by the kidneys. About 8% is converted to digoxin.
Digitoxin has a serum half life of 7-9 days. As a result, clinical effects do not fully
develop until steady state levels (approximately 5 half lives) are achieved, and 3-5
weeks are needed for complete dissipation of digitoxin effects following
discontinuation. Digitoxin is greater than 95% bound to plasma proteins. The bound
drug is in equilibrium with the unbound fraction. At equilibrium, the concentrations in
cardiac tissue are 15 to 30 times those in the plasma; the concentration in skeletal
muscle is about half that in the heart.
9. Objective response
Responses will be categorized according to biochemical response by PSA assessments.
The event of progression and time to progression are defined based on PSA progression
(biochemical progression), objective progression (new metastases) or subjective
progression whatever comes first. Any response has to be confirmed after 4 weeks.
A. Biochemical response
Complete S-PSA response (CR)
Normalisation of PSA (less than 5 ng/ml) on two successive evaluations (minimum
interval of 4 weeks).
Partial response (PR)
Decrease from baseline S-PSA value by 50% or more, but without normalization on two
consecutive evaluations with 4 weeks interval.
Progression (PD)
Increase from nadir S-PSA during digitoxin treatment by ≥ 50% at two consecutive
evaluations with 4 weeks interval.
Stable disease (SD)
S-PSA change which does not qualify for CR, PR or progression.
B. Subjective effect
At each clinical visit WHO performance status is assessed.
Subjective response: increase of performance status
Subjective progression: deterioration of the performance status
The type and amount of analgetics are recorded and will also be analyzed.
10. Primary endpoints
The primary endpoints are;
A. The proportion of complete or partial responders as determined by S-PSA
assessments, i.e. response rate: That proportion of patients who responded to treatment
with complete response (CR) or partial response (PR).
B. Survival; time to death: from date of registration to date of death due to any cause.
11. Secondary endpoints
Time to response: from date of registration to date of first observation of response of
disease.
Time to progression; from date of registration to date of first observation of progressive
disease.
12. Statistical Considerations
This is a pilot phase II, non-randomized, single-arm study. The purpose is to assess the
eventual anti-tumor activity of digitoxin in a population of patients with AIPC.
A two-stage design is used to minimize the expected number of patients treated in the
event that the regimen proved to be successful or disappointing (30). The regimen
should be rejected if the estimated true response rate is less than 5 % and would be
accepted as active if the true response rate is greater than 20%. In the first stage we
accrue 15 patients. If no responder is found among these, the study is closed and the
drug is regarded as inactive for AIPC. If one or more patients respond, additional 15
patients will be accrued.
If three or fewer patients among these 30 respond, the drug will be regarded as inactive,
if four or more respond we consider the drug is promising. An alpha error of 0.05 and a
beta error of 0.10 are used; thus, the null hypothesis is that the true response rate is ≤5%
versus the alternative hypothesis that the true response is ≥20%. With this design, the
probability of rejecting the null hypothesis when it is true is 0.058 and the power is
0.865 when the response probability is 20 %. Kaplan-Meier estimates of time to
progression and overall survival will also be determined.
13. Criteria for removal from protocol treatment.
13.1. Progression of disease.
13.2. Unacceptable toxicity requiring discontinuation of digitoxin.
13.3. The patient may withdraw from the study at any time for any reason. All reasons
for discontinuation of treatment must be documented in the patient record.
14. Adverse events
14.1. Definition of adverse event
An adverse event (AE) is any unintended symptom or medical complaint or clinically
relevant change in a laboratory test that is considered drug related or not.
Progression of the prostate cancer is not considered AE and should not be entered on the
AE form, however, clinical symptoms, whether or not related to AIPC are considered as
AE:s.
Serious Adverse Event (SAE) definition;
1. Death
2. Permanent or severe disability
3. In-patient hospitalization (hospitalization for study purposes is not to be considered
a serious adverse event.)
The investigator shall report all Serious Adverse Events (SAE:s) immediately. The
initial report shall be promptly followed by detailed, written reports.
The investigator is responsible for the prompt notification to the competent Authority
(Pharmacovigilance Unit, Medicinal Product Agency, P.O. Box 26, S-751 03 Uppsala,
Sweden, phone: +46 18175600, fax: +46 185485666)
and the Ethics Committee (Regionala etikprövningsnämnden i Göteborg, Box 100, 405
30 Göteborg).
The investigator has to keep detailed records of all Adverse Events (AE:s) reported to
him and to perform an evaluation with respect to seriousness, causality and
expectedness.
By the question “Have you had any health problems since your previous visit?” adverse
events may be obtained. Adverse events will be recorded with information about
seriousness, date of onset, duration, maximum intensity, action taken and outcome. The
causal relationship with the study drug will be assessed, and classified as;
1. Probable: Time relationship exists. No other causative factors.
2. Possible: Time relationship exists, but other causative factors may exist.
3. Unlikely: Time relationship non-existent or other factors certain or
probable to have been causative.
4. Cannot be classified: Insufficient information available for
evaluation.
5. Overdose: The symptoms are related to overdose of the drug.
All changes in the patients´ medication such as change of dose or new medication
should be recorded in the patient record.
Serious Adverse Events, SAE:
Serious adverse events should be reported by the investigator to the competent authority
within 1 working day, by phone, fax or e-mail, se above for addresses.
15. Patient information and informed consent
Patient information och informerat samtycke.
Digitoxin är en form av digitalis som ursprungligen kommer från Digitalis purpurea (Fingerborgsblomman).
Preparatet används vid hjärtsvikt och hjärtrytmrubbningar.
Det finns beskrivningar alltsedan medeltiden som tyder att digitalis kan ha effekt vid cancersjukdomar. De
senaste åren har vi och andra också visat att prostata cancer celler är känsliga för digitoxin i koncentrationer som
inte har några negativa effekter på kroppen i övrigt. Dessa försök är gjorda i laboratorium i cellkulturer.
Ett tidigt tecken på att prostata cancer cellerna blir motståndskraftiga mot hormonell behandlingen är att PSA
(prostata specifikt antigen) värdet stiger. I den situationen finns det idag ingen etablerad behandling som visat
sig vara effektiv. Avsikten med denna studie är därför att undersöka om behandling med digitoxin i tablett form
kan motverka prostatacancern. För att undersöka om digitoxin har denna effekt kommer halten av PSA i serum
att regelbundet följas. Den pågående hormonella behandlingen kommer inte att avbrytas
Om man inte har någon hjärtsjukdom och normala salthalter i blodet ger digitoxin sällan några biverkningar.
Alla som ingår i studien kommer också att noga undersökas (inklusive EKG, elektrokardiogram) för att se att det
inte föreligger några risker med att ta digitoxin. Blodprover (koncentrationen av digitoxin och PSA-värdet)
kommer att undersökas med 4 veckors mellanrum. Laboratorieförsöken har visat att ju högre digitoxin
koncentration desto starkare är effekten mot cancer cellerna. För höga koncentrationer digitoxin i blodet ger
allvarliga biverkningar. Digitoxin koncentrationen i blodet skall därför helst hållas högt inom det terapeutiska
intervallet, alltså mellan 20-25 ng/ml, därför görs upprepade mätningar av digitoxin koncentrationen och dosen
digitioxin som tas justeras.
Om PSA värdet stiger eller om det finns andra tecken på att prostatacancern växer, avbryts behandlingen Samma
symptomlindrande behandling som om man inte var med i studien kommer att ges vid behov.
All information som samlas in under studien kommer att bevaras med samma sekretessregler som gäller för den
vanliga sjukhusjournalen. Informationen kommer att avidentifieras när den presenteras.
Huvudansvarig
Johan Haux, leg.läk., med.dr.
KSS Tel:0500-431000
Informerat samtycke "Digitoxin behandling som prostata cancer behandling."
Jag har fått muntlig information och läst igenom den skriftliga informationen och förstått
vad studien går ut på. Jag ger härmed mitt samtycke till att deltaga i studien.
Mitt deltagande är helt frivilligt och jag kan när som helst dra mig ur utan att behöva ange skäl till det.
Ort och
datum
Namnteckning
16. References
1. Vårdprogram för Prostatacancer,
2004 (PDF-format),
Onkologist centrum södra sjukvårdsregionen.
http://www.ocsyd.lu.se/Vardprog/vardmeny.html
2. Tannock IF, de Wit R, Berry WR, Horti J, Pluzanska A, Chi KN, Oudard S, Theodore
C, James ND, Turesson I, Rosenthal MA, Eisenberger MA; TAX 327 Investigators.
Docetaxel plus prednisone or mitoxantrone plus prednisone for advanced prostate
cancer.
N Engl J Med. 2004 Oct 7;351(15):1502-12.
3. Petrylak DP, Tangen CM, Hussain MH, Lara PN Jr, Jones JA, Taplin ME, Burch PA,
Berry D, Moinpour C, Kohli M, Benson MC, Small EJ, Raghavan D, Crawford ED.
Docetaxel and estramustine compared with mitoxantrone and prednisone for
advanced refractory prostate cancer.
N Engl J Med. 2004 Oct 7;351(15):1513-20.
4. Bubley GJ, Carducci M, Dahut W, Dawson N, Daliani D, Eisenberger M, Figg WD,
Freidlin B, Halabi S, Hudes G, Hussain M, Kaplan R, Myers C, Oh W, Petrylak DP,
Reed E, Roth B, Sartor O, Scher H, Simons J, Sinibaldi V, Small EJ, Smith MR, Trump
DL, Wilding G, et al. Eligibility and response guidelines for phase II clinical trials in
androgen-independent prostate cancer: recommendations from the Prostate-Specific
Antigen Working Group.
J Clin Oncol. 1999 Nov;17(11):3461-7.
5. Medvedev AE, Johnsen AC, Haux J, Steinkjer B, Egeberg K, Lynch DH, Sundan A,
Espevik T. Regulation of Fas and Fas-ligand expression in NK cells by cytokines and
the involvement of Fas-ligand in NK/LAK cell-mediated cytotoxicity.
Cytokine. 1997 Jun;9(6):394-404.
6. Johnsen AC, Haux J, Steinkjer B, Nonstad U, Egeberg K, Sundan A, Ashkenazi A,
Espevik T. Regulation of APO-2 ligand/trail expression in NK cells-involvement in
NK cell-mediated cytotoxicity.
Cytokine. 1999 Sep;11(9):664-72.
7. Haux J, Johnsen AC, Steinkjer B, Egeberg K, Sundan A, Espevik T. The role of
interleukin-2 in regulating the sensitivity of natural killer cells for Fas-mediated
apoptosis.
Cancer Immunol Immunother. 1999 May-Jun;48(2-3):139-46.
8.Haux J.
Digitoxin is a potential anticancer agent for several types of cancer.
Med Hypotheses. 1999 Dec;53(6):543-8. Review.
9. Haux J, Lam M, Marthinsen ABL, Strickert T, Lundgren S.
Digitoxin, in non toxic concentrations, induces apoptotic cell death in Jurkat T cells
in vitro.
Z-ONKOL. Zeitschrift für Onkologie. 1999; 31/1 (14-20).
10. Haux J, Solheim O, Isaksen T, Angelsen A.
Digitoxin, in non-toxic concentrations, inhibits proliferation and induces cell death in
prostate cancer cell lines.
Z-ONKOL. Zeitschrift für Onkologie. 2000; 32/1 (11-16)
11. Haux J, Marthinsen ABL, Gulbrandsen M, Alfredsen AS, Johansen H, Strickert.
Digitoxin sensitizes malignant breast cancer cells for radiation in vitro.
Z Onkol 1999;31: 61-65
12. McConkey DJ, Lin Y, Nutt LK, Ozel HZ, Newman RA.
Cardiac glycosides stimulate Ca2+ increases and apoptosis in androgen-independent,
metastatic human prostate adenocarcinoma cells.
Cancer Res. 2000 Jul 15;60(14):3807-12.
13. Yeh JY, Huang WJ, Kan SF, Wang PS.
Inhibitory effects of digitalis on the proliferation of androgen dependent and
independent prostate cancer cells.
J Urol. 2001 Nov;166(5):1937-42.
14. Smith JA, Madden T, Vijjeswarapu M, Newman RA.
Inhibition of export of fibroblast growth factor-2 (FGF-2) from the prostate cancer
cell lines PC3 and DU145 by Anvirzel and its cardiac glycoside component, oleandrin.
Biochem Pharmacol. 2001 Aug 15;62(4):469-72.
15. Johansson S, Lindholm P, Gullbo J, Larsson R, Bohlin L,
Claeson P. Cytotoxicity of digitoxin and related cardiac glycosides in human tumor
cells.
Anticancer Drugs. 2001 Jun;12(5):475-83.
16. Pharmacotherapy: “A Pathophysiologic Approach”
Joseph T. Dipiro, Robert L. Talbert, Gary C. Yee, Gary R. Matzke, Barbara G. Wells, L.
Michael Posey
Appleton & Lange; 3rd edition 1998
17. Farnsworth WE.
Na+,K(+)-ATPase: the actual androgen receptor of the prostate?
Med Hypotheses. 1993 Oct;41(4):358-62. Review.
18. Haux J.
Digitalis; impinges on more than just the (ion-) pump.
Med Hypotheses. 2002 Dec;59(6):781-2.
19. Srivastava M, Eidelman O, Zhang J, Paweletz C, Caohuy H, Yang Q, Jacobson KA,
Heldman E, Huang W, Jozwik C, Pollard BS, Pollard HB. Digitoxin mimics gene
therapy with CFTR and suppresses hypersecretion of IL-8 from cystic fibrosis lung
epithelial cells.
Proc Natl Acad Sci U S A. 2004 May 18;101(20):7693-8.
20. Yang Q, Huang W, Jozwik C, Lin Y, Glasman M, Caohuy H, Srivastava M,
Esposito D, Gillette W, Hartley J, Pollard HB.
Cardiac glycosides inhibit TNF{alpha}/NF-{kappa}B signaling by blocking recruitment of TNF receptor-associated
death domain to the TNF receptor.
Proc Natl Acad Sci U S A. 2005 Jul 5;102(27):9631-6.
21. Balkwill F, Mantovani A.
Inflammation and cancer: back to Virchow?
Lancet. 2001 Feb 17;357(9255):539-45. Review.
22. Haux J.
Infection and cancer.
Lancet. 2001 Jul 14;358(9276):155-6.
23. Gordon JN, Goggin PM.
Thalidomide and its derivatives: emerging from the wilderness.
Postgrad Med J. 2003 Mar;79(929):127-32. Review.
24. Haux J
Old drugs – new uses
http://pmj.bmjjournals.com/cgi/eletters/79/929/127#233
25. Johnson PH, Walker RP, Jones SW, Stephens K, Meurer J, Zajchowski DA, Luke
MM, Eeckman F, Tan Y, Wong L, Parry G, Morgan TK Jr, McCarrick MA, Monforte J.
Multiplex gene expression analysis for high-throughput drug discovery: screening
and analysis of compounds affecting genes overexpressed in cancer cells.
Mol Cancer Ther. 2002 Dec;1(14):1293-304.
26. Haux J, Klepp O, Spigset O, Tretli S. Digitoxin medication and cancer; case
control and internal dose-response studies.
BMC Cancer. 2001;1(1):11.
27. Grossmann M, Jamieson MJ, Kirch W. Effects of digoxin and digitoxin on
circadian blood pressure profile in healthy volunteers.
Eur J Clin Invest. 1998 Sep;28(9):701-6.
28. Grossmann M. Effects of cardiac glycosides on 24-h ambulatory blood pressure in
healthy volunteers and patients with heart failure.
Eur J Clin Invest. 2001;31 Suppl 2:26-30. Review.
29. http://www.felleskatalogen.no
30. Gehan EA. Update on planning of phase II clinical trials.
Drugs Exp Clin Res. 1986;12(1-3):43-50.
18. CRF
Clinical Research File
”En fas 2 studie av tablett behandling med digitoxin för hormonrefraktär prostata
cancer.”
Besöks nummer:
dato:
WHO perfomance status (märk av);
0.Fully active, able to carry out all pre-disease activities without restriction.
1. Restricted in strenuous activity but ambulatory and able to carry out any light work or
pursue sedentary occupation.
2. Ambulatory and capable of all self-care but unable to carry out any light work. Up
and about more than 50% of waking hours.
3. Capable of only limited self-care; confined to bed or chair more than 50% of waking
hours.
4. Completely disabled. Unable to carry out any self-care and confined totally to bed or
chair
Vikt:
Blodtryck:
Lab. status (se ”flow chart”):
PSA värde:
Digitoxin koncentration:
Eftersök eventuella ”adverse events”; ”Har du haft några hälsoproblem sedan förra
besöket?”