Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
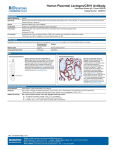
Placental M-CSF, GM-CSF and G-CSF alterations in Small for Gestational Age infants. U. Rajesh ٭, A.L. Seager, R.H. Jones, T.V. Macfarlane,B. Manshian, M. Moller, G. Morgan, C.A. Thornton. Singleton Hospital ,Swansea. Institute of Life Science, School of Medicine, Swansea University, Swansea. ٭ SGA Physiologic adaptive response to various stimuli acting to limit 50-70% of fetuses with a birth weight below the 10th centile for gestational age are constitutionally small (Ott WJ 1988, Wilcox AJ,1983). Heterogenous group of fetuses that have failed to achieve their growth potential-IUGR Fetuses that are constitutionallly small throughout pregnancy-SFD Background Cytokines provide an important communication system in coordinating immune and inflammatory responses. Several cytokines have been identified in placenta and/or uterus. A number of colony stimulating factors (CSFs), which are named for their major target cells, Granulocyte -G-CSF Granulocyte-macrophage- GM-CSF Macrophage-MCSF Background M-CSF -Macrophage Colony Stimulating FactorIt is a Haematopoietic cytokine mediating placental growth, development and proliferation of myeloid haematopoietic cells. M-CSF is secreted by uterine gland cells, and the levels increased in the first few days of pregnancy, with receptor present on invasive trophoblast cells. Pollard et al., Nature. 1987. Background There is evidence for expression of M-CSF, GMCSF and G-CSF in the Feto-Maternal interface. Ringler,1989, Robertson 1990 Few studies have shown alterations in levels of M-CSF, GM CSF in placental tissue in intrauterine disease. Hayashi 1996 &1998, Stallmach 1995. Objectives To evaluate whether M-CSF, GM-CSF and G-CSF levels in placentas of SGA (Small for Gestational Age) differ from AGA (Appropriate for Gestational Age) controls. To correlate alterations in these essential cytokines in placentas of SGA infants while attempting to classify clinical phenotypes of SGA. Understand placental role in pathophysiology of SGA better. Methods Definitions of SGA LREC approval Consent Recruitment IUGR Constitutionally small for dates (SFD) Controls (AGA) Fundal Ht Customised growth chart Methods Cord Blood &Placenta Collection Placental Explant culture Sandwich ELISA Quantikine kit (R&D Systems, UK) used Quantify cytokines in stored supernatants Cord blood serum analysis • SPSS Version 13 Mann Whitney U test Results n=65 14=Term SFD 12=Term IUGR 5=Preterm IUGR 32=Term Controls 2=Preterm Controls Results Parameters IUGR SFD Controls n=17 n=14 n=34 Maternal Age 26 29 28 Parity- Primi- gravidas 10 5 12 9 8 19 8 5 15 37 38.5 39 Mean Birth Weight (g) 2167 2720 3230 Head Circumference 33 34 34 Placenta weight 442 527 657 SCBU admission 7 0 2 Mode of Delivery- Vaginal C. Section Gestation (Wks) TERM G-CSF (pg/0.2g tissue /ml) GM-CSF(pg/0.2g tissue/ml) Results IUGR SFD Control IUGR SFD Control Placental M-CSF(pg/0.2g tissue/ml) Results p=0.005 P=0.090 IUGR SFD CONTROL Serum M-CSF(pg/ml) Results Conclusions First report distinguishing clinical phenotypes of SGA (IUGR and SFD) and correlating with cytokine alterations. The reduced M-CSF in placenta of IUGR and SFD infants probably reflects poor placental development and function. Increased M-CSF in maternal serum has been noted in IUGR pregnancies. Does Maternal M-CSF down regulate the placental and fetal production of M-CSF? Future directions Study maternal blood along with cord blood and placenta to correlate changes Redistribution Doppler studies to identify severe IUGR and correlate findings. Further study of amniotic fluid, placenta, cord blood &maternal serum for cytokine changes. Therapeutic implications Methods of diagnosing and treating pre eclampsia Methods are provided for the diagnosis and treatment of patients with increased risk of gestational hypertension or pre eclampsia. The methods involve measuring serum M-CSF levels, and administration of M-CSF. MUMBLES ILS Thank you cds GM-CSF Group Mean(pg/ml) G-CSF M-CSF Mean(pg/ml) Std.Deviation Mean(pg/ml) Std.Deviation Std.Deviation 1 49.69 52.73 22968.3 16305.58 579.95 351.12 2 49.02 51.2 24.659.8 26863.4 774.96 319.85 3 38.98 27.38 24177.4 22310.1 1455.63 1349.22 Extra stuff GM-CSF Group Mean(pg/ml ) Std.Devia tion 1 49.69 52.73 2 49.02 51.2 3 38.98 27.38 G-CSF M-CSF Mean(pg/ml ) Std.Deviatio n Mean(pg/ml ) Std.Deviatio n 22968.3 16305.58 579.95 351.12 26863.4 774.96 319.85 22310.1 1455.63 1349.22 24.659.8 24177.4 Background In humans, the expression and localization of mRNA for M-CSF have been demonstrated in mesenchymal cells of the chorionic villous stroma, particularly in cytotrophoblasts lining the villous core and in the cytotrophoblastic core in the first trimester; in villous mesenchymal cells in the second trimester; and in cells lining the villous vessels in the third trimester. Kanazaki et al., Human Reprod., 7:563-567 (1992); Daiter et al., J. Clin. Endocrinol. Metab. 74:850-858 (1992). Circulating levels of macrophage M-CSF during pregnancy are also higher than those of non-pregnant women. Yong et al., Blood, 180:2897-2902 (1992).