Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Management of acute coronary syndrome wikipedia , lookup
Heart failure wikipedia , lookup
Hypertrophic cardiomyopathy wikipedia , lookup
Coronary artery disease wikipedia , lookup
Cardiac surgery wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Myocardial infarction wikipedia , lookup
Lutembacher's syndrome wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
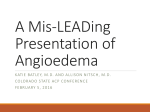
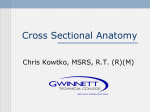
Superior vena cava syndrome caused by heart tumor 71 Superior Vena Cava Syndrome Caused by Right Atrial Carcinosarcoma in Emergency Department: A Case Report and Literature Review Kuo-Hsin Lee1,2, Cheuk-Kwan Sun1,2, I-Ting Tsai1,2 Superior vena cava syndrome, which comprises a group of nonspecific signs and symptoms caused by obstruction of the superior vena cava (SVC), is usually a complication of SVC compression by pulmonary or mediastinal tumors. Usual manifestations including shortness of breath, dyspnea, headache, and facial edema occur only after days to weeks after the beginning of SVC obstruction. Although a detailed medical history and physical examination may shed light on the diagnosis, imaging studies are usually required for establishing the diagnosis and pinpointing the causes. Herein, we report a case of facial edema resulting from obstruction of superior vena cava caused by right atrial carcinosarcoma with initial presentation mimicking anaphylaxis in the emergency department. Final diagnosis was made one month later after disease progression. The patient died of distant brain metastasis six months later despite aggressive treatment. For early diagnosis, emergency physician should have a high level of suspicion for non-specific symptoms hinting the diagnosis. Chest x-ray and contrast-enhanced chest computed tomography should be considered for differential diagnosis. Key words: superior vena cava syndrome, cardiac carcinosarcoma Introduction Superior vena cava syndrome (SVCS) result- ing from external compression or intra-luminal obstruction of the superior vena cava with subsequent engorgement of the collateral vessel of the chest, neck, and head is a group of nonspecific signs and symptoms including facial flushing and edema, dyspnea, and cough. In addition, strider, nasal congestion, epistaxis, tongue swelling, hoarseness, dysphagia, visual disturbances, headache, and periorbital edema have also been described(1,2). SVCS is a complication of many disease conditions including malignancies and hematological disorders as well as iatrogenic causes such as placement of transvenous pacemaker and central venous catheters(3). Early diagnosis of SVCS might be difficult in a patient without known risk factors. Besides, superior vena cava obstructed by primary cardiac tumors is rare in the literature. We report a case of SVCS caused by right atrial carcinosarcoma with initial presentations of facial erythematous edema and congestive heart failure. Definite diagnosis was made one month after his first visit to the emergency department. Case Report A 74-year-old man presented to our emergency Received: November 22, 2011 Accepted for publication: June 13, 2012 From the 1Department of Emergency Medicine, E-Da Hospital, Kaohsiung, Taiwan, 2I-Shou University, Kaohsiung, Taiwan Address reprint requests and correspondence: Dr. I-Ting Tsai Department of Emergency Medicine, E-Da Hospital 1 Yida Road, Jiaosu Village, Yanchao District, Kaohsiung City 82445, Taiwan (R.O.C.) Tel: (07)6150011 ext 3166 Fax: (07)6150915 E-mail: [email protected] 72 J Emerg Crit Care Med. Vol. 23, No. 2, 2012 department with complaint of acute-onset fever up to 39℃. According to his history, mild exertion corticosteroid was administrated and epinephrine was inhaled. He was discharged after partial im- eyelids were noted for 2 weeks. He had visited a local hospital for initial help where upper respiratory for intermittent recurrent facial flushing, dyspnea, and cough. Fever up to38.6℃ was noted with a dyspnea with intermittent noisy breathing sound, facial flushing with edema, and bilateral puffy tract infection was diagnosed and oral medication was prescribed. He was borderline-hypertensive and mildly hyperthermic with a blood pressure of 141/82 mmHg, body temperature of 37.2℃, pulse rate of 91 beats per minute, and respiratory rate of 18 per minute. Physical examination showed nonspecific findings except facial edema and flushing. Initial laboratory study showed normal white blood cell count (9.6 × 103 per cubic millimeter), mildly elevated C-reactive protein level (29.1 mg/L) with normal liver and renal function tests. Under the impression of anaphylaxis and angioedema based on his facial edema, respiratory symptoms, and history of medication, intravenous Fig. 1 provement of dyspnea and facial edema. Seven days later, he came back to our emergency department blood pressure of 109/67 mmHg, pulse rate of 93 beats per minute, respiratory rate of 21 per minute. Physical examination revealed facial swelling with jugular vein engorgement, systolic murmur and gallop, decreased bilateral breathing sound with basal rales. No abdominal distension or edema over lower extremities was found. Laboratory data displayed only moderately elevated C-reactive pro- tein level (79.4 mg/L). Chest x-ray showed mild bilateral pleural effusions, borderline cardiomegaly and superior mediastinal widening (Fig. 1). The diagnosis was facial cellulites, highly suspicious of congestive heart failure. He was discharged with oral antibiotics and diuretics. One month after his Erect chest x-ray showing widening of superior mediastinum (white arrows) and bilateral mild pleural effusions (black arrowheads) Superior vena cava syndrome caused by heart tumor 73 first presentation to our emergency department, he came to our emergency department again for ponents over right atrium. Contrast-enhanced chest computed tomography scan showed masses in the plete ECG showed sinus rhythm with low voltage on limb leads. Echocardiography was arranged for opacification of collateral veins, compatible with superior vena cava syndrome. No space-occupying persistent dyspnea, intermittent facial edema, and exacerbation of bilateral pleural effusions. Com- the impression of congestive heart failure. Echocardiography showed a huge mass with cystic com- Fig. 2 Fig. 3 right atrium, right ventricle, superior vena cava, and right internal jugular vein with engorgement and lesion was noted over bilateral pulmonary arteries (Fig. 2 & Fig. 3). To prevent embolic event, Axial contrast-enhanced CT of the chest demonstrating a right atrium mass (black arrow), opacification of hemi-azygous vein with dilatation (black arrowhead), bilateral pleural effusions and pericardial effusions at the atrial level A superior vena cava mass (white arrow) together with opacification of venous collaterals (white arrowheads) at the level of aortic arch 74 J Emerg Crit Care Med. Vol. 23, No. 2, 2012 emergent operation for removal of tumors in right atrium, right ventricle, and superior vena cava by contrast-enhanced chest computed tomography scan requires at least two key findings, including Repeated Contrast-enhanced chest computed tomography scan two months postoperatively showed erals on the other(9). Right atrial tumor, which was identified in was performed. Pathological analysis of the tumor masses confirmed the diagnosis of carcinosarcoma. tumor recurrence in right atrium with extension into mediastinum. The patient expired four months after operation due to increased intracranial pressure caused by brain metastasis. Discussion We described a patient of SVCS with a number of apparently unrelated non-specific symptoms and signs that posed a challenge to the emergency physician in differential diagnosis. For instance, increased work of breathing and dilated jugular vein on lying down resulting from the increase in venous return and jugular venous pressure can mimic congestive heart failure or pericardial disease. Facial and neck flushing with edema might be diagnosed as a dermatological or otolaryngeal condition such as idiopathic angioedema, facial cellulites, or deep neck infection(4). On the other hand, anaphylaxis may also present with facial flushing and edema, periorbital edema, or stridor that is difficult to distinguish from SVCS with unknown risk factors(5). The majority of patients with SVCS have an abnormal chest radiograph, with the most common findings being mediastinal widening and pleural effusion(6). However, the widened upper mediastinum without trachea deviation as well as the abnormal cardiac contour and mass density in the plain chest film of our patient may be interpreted as tortuous great vessels. On the other hand, contrast-enhanced chest computed tomography scan has the advantages of being non-invasive, rapid, and able to precisely identify the location and degree of superior vena cava/brachiocephalic venous obstruction as well as the extent of lesion(7,8). Clinical diagnosis of SVCS the lack of opacification of the superior vena cava on the one hand and opacification of venous collat- our patient by echocardiography, is a rare cause of SVCS (10). Moreover, since typical cardiovascular signs and symptoms of right atrium tumor are those of right heart failure (i.e. fatigue, peripheral edema, hepatomegaly, ascites, and prominent "a waves" in jugular venous pulses), its presentation initially as SVCS but not right heart failure is uncommon(11). Left ventricular inflow obstruction, right heart failure, pulmonary emboli, systemic embolic event, dysrhythmia, conduction blockade have been reported to be fatal complications associated with cardiac tumors(12). Unrecognized SVCS caused by tumor occupation of right atrium and superior vena cava delayed diagnosis of the underlying disease may lead to worsened outcome of our patient. The symptoms and signs of cardiac tumors are also highly variable and tumor plop sound by auscultation may be the only physical finding. Cardiac carcinosarcoma was a rare but aggressive malignancy that has only been sporadically reported. To our best knowledge, SVCS caused by cardiac carcinosarcoma has not been reported in the literature. As in most cases of cardiac tumor, the diagnosis of malignancy is not made preoperatively. The aims of operation are to relieve ventricular inflow obstruction, prevent embolism, and obtain tissue for diagnosis. In general, sarcomas proliferate rapidly and cause death through widespread infiltration of the myocardium, obstruction of blood flow through the heart, and distant metastases. Although complete resection is the treatment of choice, most patients develop recurrent disease and eventually succumb even after complete tumor resection. The median survival is typically 6 to 12 months, although long-term survival has been reported with complete resection(13). Superior vena cava syndrome caused by heart tumor Conclusion High level of vigilance towards typical symptoms and signs and an incidental finding on chest radiograph such as mediastinal widening are keys to the diagnosis of SVCS. Our report described a patient with initial presentation of a number of seemingly nonspecific signs and symptoms that delayed the diagnosis. Suspicious picture on chest radiograph in the emergency department may warrant the performance of contrast-enhanced chest computed tomography scan for early differential diagnosis. References 1. Wi l s o n L D, D e t t e r b e c k F C, Ya h a l o m J. Clinical practice. Superior vena cava syndrome w i t h m a l i g n a n t c a u s e s. N E n g l J M e d 2007;356:1862-9. 2. Rice TW, Rodriquez RM, Light RW. The superior vena cava syndrome: clinical characteristics and evolving etiology. Medicine (Baltimore) 2006;85:37-42. 3. Bell DR, Woods RL, Levi JA. Superior vena cava obstruction: a 10-years experience. Med J Aust 1986;145:566-8. 4. Kim KM, Park CS, Kim TB, Cho YS, Moon HB. A variant of idiopathic angioedema presenting as persistent facial swelling over 1 year. Allergy 2008;63:378-9. 5. Khalili B, Boggs PB, Bahna SL, Marsala AJ, Tapolyai M, Bryn RO. Superior vena cava syndrome: A masquerader of anaphylaxis. J Allergy 6. 7. 8. 9. 10. 11. 12. 13. 75 Clin Immunol 2007;119(Supple 1):S29. (Abst) Rice TW, Rodriguez RM, Barnette R, Light RW. Prevalence and characteristics of pleural effusions in superior vena cava syndrome. Respirology 2006;11:299-305. Kim HJ, Kim HS, Chung SH. CT diagnosis of superior vena cava syndrome: importance of collateral vessels. AJR Am J Roentgenol 1993;161:539-42. Qanadli SD, El Hajjam M, Bruckert F, et al. Helical CT phlebography of the superior vena cava: diagnosis and evaluation of venous obstruction. AJR Am J Roentgenol 1999;172:1327-33. Bechtold RE, Wolfman NT, Karstaedt N, Choplin RH. Superior vena caval obstruction: detection using CT. Radiology 1985;157:485-7. Ramnarine IR, Davidson L, van Doorn CA. Primary cardiac carcinosarcoma: a rare, aggressive tumor. Ann Thorac Surg 2001;72:927-9. Kuon E, Kreplin M, Weiss W, Dahm JB. The challenge presented by right atrial myxoma. Herz 2004;29:702-9. Sughimoto K, Shiikawa A, Ohkado A, Nanaumi M. Multiple cardiac myxomas with pulmonary arterial obstruction and acute right heart failure. Jpn J Thorac Cardiovasc Surg 2004;52:530-3. Zhang PJ, Brooks JS, Goldblum JR, et al. Primary cardiac sarcomas: a clinicopathologic analysis of a series with follow-up information in 17 patients and emphasis on long-term survival. Hum Pathol 2008;39:1385-95. 76 J Emerg Crit Care Med. Vol. 23, No. 2, 2012 延遲診斷由右心房癌肉瘤所引起的 上腔靜脈症候群:急診室個案報告 李國新1,2 孫灼均1,2 蔡易廷1,2 上腔靜脈症候群的臨床表現通常是一群非特異性的症狀其典型表現像臉部頸部紅腫,呼吸喘及咳嗽 都是急診室裡常見的主訴。上腔靜脈症候群症狀可能都持續一段時間且需要理學檢查和詳細的病史來與 其他疾病作鑑別診斷。我們報告一個由右心房癌肉瘤引起上腔靜脈症侯群的病例在急診的臨床表現類似 過敏反應,一個月後才確定診斷。儘管積極的治療病人最終半年後病人還是死於遠處腦部轉移。像這種 懷疑上腔靜脈症候群的情形,胸部X光和胸部顯影電腦段層應及早於急診室中安排作為鑑別診斷的工具 是有價值的。 關鍵字: 上腔靜脈症候群,心臟癌肉瘤 收件:100年11月22日 接受刊載:101年6月13日 1 義大醫院急診醫學部 2義守大學 通訊及抽印本索取:蔡易廷醫師 高雄市燕巢區角宿里義大路1號 義大醫院急診醫學部 電話:(07)6150011轉3166 傳真:(07)6150915 E-mail: [email protected]