Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
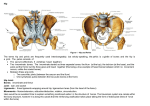
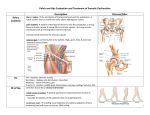
OMM 15- ST Pelvis, Hip, Thigh Hip: a region (junction of proximal femur and lateral pelvis) Diarthrosis (Synovial): ball and socket Look for acute, chronic, overuse, traumatic. Associated pop/click or pain (severity/radiation) Referred pain: SI dysfunction (trochanteric area); lumbar radiculopathy Action Flexion Extension Abduction Adduction External rotation Internal Rotation Muscle Ilopsoas Gluteus maximus Gluteus medius/minimus Add brevis, longus, magnus, pectineus, gracilus Internal and external obturator, quadrates femoris, Superior and Inferior gemelli Gluteus medius and minimus Instruction Bend Knee to chest Lie face down, bend knee and lift Lie flat, move leg outward Lie flat, move leg inward Lie flat, bend knee across middle Lie flat, bend knee away from midline Hip Exam Inspection: ◦ the hips anteriorly and posteriorly (standing) ◦ note any asymmetry in iliac crest heights,or level of gluteal folds ◦ After appropriate draping, look for: skin changes; redness, swelling, bruising, muscle atrophy Palpation: while standine and supine, note any instability, tenderness, crepitus Strength testing/ROM: active and passive Examine the ROM of the hips by asking the patient to perform the following movements: ◦ FLEXION - 90 degrees (knee extended); 120 degrees (knee flexed) ◦ EXTENSION – 30 degrees ◦ ADDUCTION – 30 degrees ◦ ABDUCTION – 45 degrees ◦ INTERNAL ROTATION – 40 degrees ◦ EXTERNAL ROTATION -45 degrees Special testing: Thomas test: Iliopsoas tightness (thigh off table), key is to hold opposite knee tightly to chest Ober’s test: IT band tightness Evaluation: When evaluating patients with hip pain it is likely to be from these sources: ◦ hip joint (intra and extra-articular) ◦ soft tissues around the hip and pelvis ◦ pelvic bones ◦ sacroiliac joint ◦ referred pain from lumbosacral spine The hip joint is one part of the pelvic girdle:(ilium, pubic ramus, and sacrum) and contains two joints the SI (sacrum and ilium) and the hip joint (head of the femur into the pelvis) (Watch patient walk)-evaluation of gait can give insight to source of problem and potential dysfunctional compensatory patterns OMM 15- ST Pelvis, Hip, Thigh I. Anterior Hip Pain A. Degenerative Joint Disease (osteoarthritis, DJD): Loss of articular cartilage at the hip joint Etiology: repetitive overuse, infection genetic , idiopathic History: Gradual onset, anterior groin pain but may be buttock or lateral thigh, initially relieved by rest ,worse with weight bearing may proceed to night pain and limited range of motion Physical Findings: Limited ROM (Internal rotation), then loss of flexion and extension Imaging: x-ray Treatment: Strengthening, physical therapy for ROM, anti-inflammatories, surgical B. Osteonecrosis AVN: loss of trabecular bone in the femoral head/neck usually during 3rd and 4th decade Etiology idiopathic: Trauma (hip dislocation or femoral neck fracture), alcohol abuse, steroid use, RA, SLE; other risks: sickle cell, radiation, Crohn’s Disease – these things result in compromise to the blood supply to the bone History: Gradual onset, groin pain but may be buttock or lateral to hip, may be sudden if femoral neck collapses Physical Findings: pain with internal and external rotation of hip and abduction. If femoral neck has collapsed they have pain with Limited ROM (Internal rotation, flexion, and abduction), Imaging: x-ray AP pelvis and frog view; sclerosis or femoral neck collapse Treatment: Strengthening, physical therapy for ROM – Surgical replacement C. Stress Fractures Etiology: Chronic overuse ◦ usually compression sided ◦ in Runners, Dancers, Recruits Diagnosis delayed 5-13 weeks risk of complications: ◦ AVN, nonunion, coxa vara, chronic pain History ◦ Anterior groin pain (87%) ◦ Weight bearing activity (recent increase, hills/mileage for femoral neck stress fractures) Insidious onset Prior stress fractures Females: Menstrual cycles, Weight changes, Eating disorders Physical Examination: pain at extreme ROM (70%), antalgic gait (22%) Hop test: Femoral Neck Fulcrum test: femoral shaft Technique Patient sits on exam table with knee extended Examiner position Place one hand under sitting patient's femur Other hand placed over knee Maneuver Apply firm pressure upward on femur Apply firm pressure downward on knee Use Xrays for healing, bone-scan for injury, Treatment: strict rest, non weightbearing, fixation (tension vs compression side) OMM 15- ST Pelvis, Hip, Thigh D. Avulsion Fractures (anterolateral) Etiology: ASIS (sartorius), AIIS (rectus), Ischial (hamstring) Mechanism: Chronic, Acute concentric/eccentric History: Males, adolescents, local pain, limit motion Physical Findings: tenderness, limit ROM & weakness Imaging: AP pelvis, Oblique (iliac crest), CT scan Treatment: Ice, stretch, gradual return, (>2cm then ORIF) – surgical repair E. Hip Pointer Etiology: Direct trauma ASIS, iliac crest Mechanism: Collision in sports History: Anterior/lateral pain after direct blow, pain localized, pain with laughing Physical Findings: Local swelling, pain, ecchymosis Imaging: xray (R/o fracture) Treatment: Pain control, NSAIDS, injections F. Inflammatory Conditions: Local manifestations of systemic disorders Symptoms – dull aching pain in groin, lateral thigh, or buttocks. Pain is often episodic with morning stiffness, improvement with moderate activity, and stiffness of hip joint motion Exam – pain with internal rotation and restriction Diagnostics – AP pelvis and frog leg views may show decreased bone mineralization or joint effusion; CBC, CRP,ANA; aspirate joint effusion and send for C&S, cell count with diff, crystal analysis Differential – broad ankylosing spondylitis, infection, inflammatory bowel disease, Reiter’s syndrome, RA, stress fracture, SLE, gout Treatment – tx underlying condition, NSAIDS, immunosuppressive agents; surgery G. Labral Tear Etiology: Tear of the fibrocartilaginous labrum usually due to high impact trauma. Tear usually anterior labrum Mechanism: Running, Hyperextension at hip, trauma History: Deep sharp anterior hip pain, deep clicking or snapping, sense of instability Physical Findings: Anterior hip pain with hip into extension, pain with anterior stress Imaging: XR/MRI Treatment: Rest, NSAIDs, Surgical repair II. Posterior and Medial Hip Problems A. Dislocation: Dislocation of femoral head from acetabulum Etiology: Genetic, instability of joint ◦ Most are posterior; injury causes the hip to be adducted, flexed, and internally rotated. An anterior dislocation would leave the hip abducted, flexed, and externally rotated Mechanism: Direct blow with hip abducted; non-contact History: Pain, inability to move, numbness Physical Findings: Short leg, hip adducted, severe pain, inability to move; Evaluate sciatic nerve function by asking patients to move toes and ankle and checking sensation on plantar and dorsal aspects of foot B. Hamstring strain Etiology: Muscle tearing Mechanism: Acute overstretching, running, sprinting Factors: inflexible, fatigue, imbalance, incomplete rehab History: Local pain, deformity, popping sensation Physical Findings: Local pain, deformity, poor ROM & strength Imaging: x-ray (avulsion), MRI, US Treatment: Ice, stretching OMM 15- ST Pelvis, Hip, Thigh C. Groin strain (Adductors) Etiology: Tearing of Adductor muscle (Micro or macro tears) Mechanism: Powerful over stretch, abduct, external rotation common in soccer History: Pain which radiates along the medial thigh, inability to run, cut, start & stop Physical Findings: Pain over muscle group, increases with resistance, possible defect Imaging: MRI – if not resolving with conventional measures Treatment: Rest, ice, stretch D. Piriformis Syndrome Etiology: Irritation to piriformis leading to sciatica symptoms Mechanism: Anatomical variance, tightness, overuse History: Cramping pain in buttock, tight hamstrings, tender piriformis, pain with sitting, radiating into leg Physical Findings: pain stretching piriformis, weakness, sciatic tenderness, normal neurologic exam Imaging: MRI (r/o other causes) if not responding to treatment Treatment: Rest, stretching, pain control, OMT III. Lateral Hip Pain A. Tensor Fascia Latae Syndrome Etiology: Overuse tendinitis, Bursitis Mechanism: Running, after foot strike, hip 30o History: Pain during gait cycle. Physical Findings: Local pain, weakness of hip flexors; Positive Ober’s Test Imaging: xray (r/o fracture) Treatment: Ice, pain control, stretching B. Greater Trochanteric Bursitis: Pain that originates over the greater trochanteric bursa that may radiate the entire length of the leg (knee and ankle but not foot) Etiology: Trauma to the bursa Mechanism: trauma acute or repetitive History: Localized pain, worse rising from chair , lessens with early movement then worsens with extended movement; patients report night pain and cannot lay on affected side ;increases with hip flex/ext Physical Findings: Local pain, swelling at greater trochanter, pain cephalad to this suggest tendinosis of gluteus medius tendon Imaging: x-ray only to rule out other injury Treatment: Rest, Ice, NSAIDS, Injection, Correct biomechanics Differential: Osteoarthritis – painful internal rotation Sciatica – pain posteriorly or on top of foot Snapping hip – clicking at site Trochanteric fracture – limp persists with walking and positive Trendelenburg Risks: lumbar spine disease, intraarticluar hip pathology, previous surgery around lateral hip ( internal fixation device), RA Metastatic disease C. Lateral femoral cutaneous nerve entrapment (meralgia paresthetica) Pain and burning (dysesthesia) or hypoesthesia over lateral thigh; they may complain of groin pain and pain at SI joint; no motor involvement this is sensory nerve Risks: obesity, tight clothing, surgery, trauma; nerve exits pelvis near ASIS Primarily Affects: young muscular women who extend their hips frequently, women with scoliosis Joggers, rarely pathologic intra-abdominal/pelvic process, Truck drivers Etiology: Entrapment/ impingement of lateral femoral cutaneous nerve Mechanism: Inguinal impingement, abdominal (mass) History: Tingling, numbness lateral thigh. May be painful. Physical Findings: sensation localized, with flexion, extension of the hip Imaging: EMG (optional), studies of abdomen Treatment: Loose fitting clothing, wt loss, medications, nerve block, surgical decompression OMM 15- ST Pelvis, Hip, Thigh D. Snapping Hip: Tendons around the hip subluxate over bony prominences (iliotibial band over greater trochanter) Etiology: Several causes: Bursitis, Labral tear, Physiological Mechanism: Iliopsoas bursitis, overuse, prominence of pelvic brim, muscle tightness History: Pain and snapping around the trochanteric area; iliopsoas felt in groin area, both experience pain Physical Findings: Pain with resisted contraction of Hip flexors; have patient stand , abduct and rotate the hip, the snap is palpated over the lateral hip; snapping of the iliopsoas may be palpated as hip extends from flexed position Imaging: AP and lateral hip to R/O pathology; MRI (rule out Labral tear) Treatment: Ice, Rest, Rehab, Correct biomechanics, NSAIDS, steroid injection, surgery if tx failure and desired Differential: osteoarthritis, loose body, osteonecrosis, tear of actetabular labrum